
Abstract
Problem
Graduate medical education programs are expected to educate residents to be able to manage critically ill patients. Most obstetrics and gynecology (OB/GYN) graduate medical education programs provide education primarily in a didactic format in a traditional face-to-face setting. Busy clinical responsibilities tend to limit resident engagement during these educational sessions. The revision of the training paradigm to a more learner-centered approach is suggested.
Intervention
A blended learning education program was designed and implemented to facilitate the teaching and learning of obstetric emergencies, specifically diabetic ketoacidosis and acute-onset severe hypertension in pregnancy. The program incorporated tools to foster a community of inquiry. Multimedia presentations were also utilized as the main modality to provide instruction. The blended learning course was designed in accordance with the cognitive theory of multimedia learning.
Context
This intervention was carried out in the Department of Obstetrics and Gynecology, Southern Illinois University. All 15 OB/GYN residents were enrolled in this course as part of their educational curriculum. First, face-to-face instructions were given in detail about the blended learning process, course content, and online website. The residents were then assigned tasks related to completing the online component of the course, including watching multimedia presentations, reading the resources placed online, and participating in online asynchronous discussions. The course culminated with a face-to-face session to clarify misconceptions. Pre- and postcourse quizzes were administered to the residents to assess their retention and understanding.
Outcome
Objective analysis demonstrated significant improvements in retention and understanding after participating in the course. The blended learning format was well received by the residents. Resident perception of social presence in the asynchronous online discussions was demonstrative of low scores relating to peer-to-peer interaction. The multimedia presentations and the availability of learning resources were well received.
Lessons Learned
Outcomes of this study suggest that blended learning is a viable tool to support teaching and learning of obstetric emergencies in an OB/GYN residency program.
Background
A competent doctor in obstetrics should be able to detect the medical and surgical complications of pregnancy and manage the illness with timely and appropriate treatments. Graduate medical education programs are expected to educate residents to be able to manage critically ill patients. Most obstetrics and gynecology (OB/GYN) graduate medical education programs provide a series of formal training, primarily didactic in nature, provided in weekly, hour-long sessions in a traditional face-to-face setting. Given their clinical work schedule in OB/GYN, however, residents' engagement in these face-to-face didactic activities can be relatively low. Learner-centered, active learning approaches are required to improve resident training and clinical performance. However, there have been few attempts to revise the training modality toward learner-centered active learning in OB/GYN graduate medical education.
Blended learning involves learner-centered instructions in which the content of instructions is delivered both face-to-face and online. The main component of instruction is online based, which is controlled by the learner within reasonably set guidelines. This means that the learner can control the time, pace, and place of instruction, resulting in increased access and flexibility. 1 In recent years, there has been increased interest in the benefits of e-learning tools and blended learning in supporting and facilitating medical education.2–6 Although the majority of studies are on the use, role, and outcomes of online learning in the setting of undergraduate medical education, few studies have reported the utility of this learner-centered blended learning process in resident graduate medical education.7–9 As blended learning has the potential to improve learner-centered activities, it is anticipated to have similar beneficial effects in the setting of resident education in OB/GYN.
In this case report, we share our experience of blended learning in a graduate medical education program. We describe how we created a blended learning curriculum to address residents' deficiency of knowledge and skills in OB/GYN, how residents' learning improved with this new curriculum, how residents perceived this new approach, and lessons learned based on our experience.
Context
There are 15 residents and 16 faculty in our OB/GYN graduate medical education program. There are multiple resident learning activities. Weekly sessions include faculty-run face-to-face didactic sessions, resident-led chapter review, and grand rounds. In addition, there are bimonthly journal club meetings during which research articles are presented to the department by a team of residents, facilitated by a faculty member. Despite these educational efforts, the Maternal Fetal Medicine physicians felt that the residents have a deficiency in their knowledge regarding, and not as proficient as one would expect in, the management of several obstetric emergencies. Two of these topics include diabetic ketoacidosis (DKA) and acute-onset severe hypertension in pregnancy and postpartum. When questioned about various emergent scenarios, residents were hesitant and tentative in providing answers.
Needs Assessment
Prior to initiating the educational intervention, we assessed the residents' knowledge and skills in managing DKA and acute-onset severe hypertension in pregnancy and postpartum. As the assessment scores were low, the results demonstrated the need for further instruction in both DKA and acute-onset severe hypertension in pregnancy. The average scores for the DKA and acute-onset severe hypertension modules were 48.0% ± 17.4% and 65.1% ± 12.1%, respectively.
We also reviewed the past 6 years' residency in-training exam scores of the Council on Resident Education in Obstetrics and Gynecology (CREOG). The results revealed that our residents have been performing at the level of the national mean. This has ranged consistently around 60–65%. When evaluating the trend, it appears that the lowest scores are noted in the first year residents, reaching a peak during the second and third years, plateauing thereafter. Specific to obstetric topics on the CREOG exam, the national mean observed for the residents are also similar to the national average (60–65%), with a slight decrease below the national average over the past two years. The CREOG reports do not include how many or what type of questions pertain to obstetric emergencies. Although both overall and obstetric scores are at the level of national mean for all OB/GYN residency programs, there remains room for improvement.
Precourse assessments demonstrated a need for further instruction on these obstetric emergencies. Owing to the severity of these conditions and significant complications if poorly managed, it is important that we, as physician-educators, ensure that appropriate management of obstetric emergencies is acquired during the course of the residency program.
Curriculum Development
Theoretical framework
We designed a blended learning based on two pedagogical perspectives: community of inquiry 10 and multimedia learning. 11
Community of inquiry
The success of any blended learning program is dependent on the community of inquiry, which is both interactive and private. From an interactive standpoint, the community of inquiry supports collaboration and connection. This is consistent with social constructivism in that knowledge formation tends to be social in context as learners collaborate by sharing their experiences and insights. 12 The private component provides sufficient time for reflection to take place prior to engaging in discussion.
There are three elements that were considered to build a community of inquiry: cognitive presence, teaching presence, and social presence. Instructional materials and activities were developed to facilitate learners' cognitive construction of knowledge. The foundation for cognitive presence includes both the private reflective and the social interactive processes. These processes mutually serve to support the cyclic process of recognition of a problem, discourse and debate with peers, and creation and testing of various solutions. 12
Teaching presence requires the instructor to clarify misunderstandings and assist in review and application of the learned content. The instructor facilitates interdependent interaction between the instructional content and delivery medium, students, and instructors. Each of the types of interaction can support learning but needs to function in cooperation with one another as they cultivate communication and collaborative learning.13,14
Social presence is cultivated by allowing the learners to feel comfortable so that they can express themselves openly and cooperatively. Contrary to the fast-paced setting of a face-to-face discussion where opportunities to contribute might be lost, especially by those with a low level of understanding or those who are introvert, the online asynchronous format provides an objective way to reflect and participate in discussion. 10 Social presence should allow those less likely to participate in the face-to-face setting to gain confidence in their level of understanding and learn how to express themselves in the written form 10 with eventual transfer into increased confidence during the face-to-face interaction.
Cognitive theory of multimedia learning
The cognitive theory of multimedia learning states that meaningful learning takes place with a well-designed multimedia presentation. It takes into account the restrictions in the human cognitive architecture as learning new material is dependent on the confines of the learner's working memory.15,16
In line with the limitations of working memory, the cognitive theory of multimedia learning takes advantage of the dual coding theory. The dual coding theory defines separate information and sensory processing channels for words and pictures. 17 An effective multimedia presentation directs narrated words through the auditory channel and pictures and written words through the visual channel. This framework supposes that overload of working memory is limited as words, especially when narrated, and pictures are processed in their respective channels. Therefore, information does not overwhelm working memory of any one particular channel. Because of this, there can be parallel and concurrent active cognitive processing through the selection of words and pictures into working memory and organization of the material, followed by integration into long-term memory. 11
Program development
Instead of providing the traditional instruction in a classroom over a one-hour face-to-face session, a blended instructional unit was designed to be delivered over the course of a week. The web-based instruction began with a precourse quiz to assess the background knowledge. The course content included a self-guided, interactive, self-paced multimedia presentation in accordance with the cognitive theory of multimedia learning.11,18 It also included a supplemental reading material pertaining to the topic, an asynchronous online discussion forum, and a postcourse quiz. Quizzes included both multiple choice and essay questions. These tasks, in addition to the postcourse quiz, were intended to ensure that the material was understood and there was mastery of the cognitive skills.
The course content was housed on the learning management system Moodle. The residents were given a week each to complete the DKA module and acute-onset hypertension in pregnancy and postpartum module. Each unit was designed to culminate in a face-to-face session where misconceptions were clarified, cases were reviewed, and questions were answered. All 15 residents were enrolled in the blended learning module as part of their educational curriculum. The use of Moodle and the course content was introduced to the residents in a face-to-face setting on a Friday. At this time, goals, course content, and the sequence of instruction were reviewed with the residents.
The proposed instructional unit was designed in such a way that it met the necessary elements for a community of inquiry. Case studies and problem-based activities were used as the triggering event for the inquiry phase of cognitive processing. Specific to the social nature of the practice of medicine, cognitive and teaching presence was used as an integral role in all segments of the instructional unit. Cognitive and teaching presence functioned to maintain the focus and rigor of the educational experience. Social presence, in the asynchronous online discussions, was intended to provide the residents an opportunity to express themselves candidly.
Curriculum Evaluation
Data sources
The primary data sources were resident quiz results, online discussion posts, and a reflective journal maintained by the primary author. A program evaluation survey called the constructivist on-line learning environment survey (COLLES) 19 was utilized to assess the extent to which the blended learning approach enriched the knowledge of the residents (Appendix A) after both modules were completed. Additional questions were included in the survey (Appendix B). These questions allowed the residents to provide more in-depth reviews of the course.
Data analysis
Pre- and postcourse quizzes were scored in percentages ranging from 0% to 100% (all correct) based on the number of correct answers provided. A paired
The COLLES was comprised of 24 statements grouped into six scales, each of which addressed key questions about the quality of the online learning environment (relevance, reflection, interactivity, tutor support, peer support, and interpretation). The COLLES contains a 5-point Likert-type response scale—almost never (1), seldom (2), sometimes (3), often (4), and almost always (5)—with scores shown in parentheses. The values of each selected option were summed, and a score was created for each respondent. The additional questions included at the end of the COLLES were described in a qualitative fashion.
The leading author of this article maintained a reflective journal to depict how the curriculum went. The journal included events, thoughts, and ideas. The purpose of the journal was primarily to stimulate the recall of events at a later date when reflecting on the course or reviewing rationale for decisions made during the course.
This study was deemed as nonhuman subjects research by the ethics review board of Southern Illinois University. Residents were informed that this modality would be utilized for their instruction on the topics of DKA and acute-onset severe hypertension.
Findings
Learning outcomes
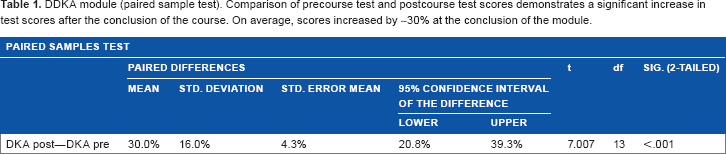
Of the 15 residents, 14 completed the DKA module. Overall, baseline knowledge of the residents was low prior to the blended learning course on DKA, 48.0% ± 17.4%. After the course, mean scores improved, 78.0% ± 11.1% and
DDKA module (paired sample test). Comparison of precourse test and postcourse test scores demonstrates a significant increase in test scores after the conclusion of the course. on average, scores increased by ~30% at the conclusion of the module.
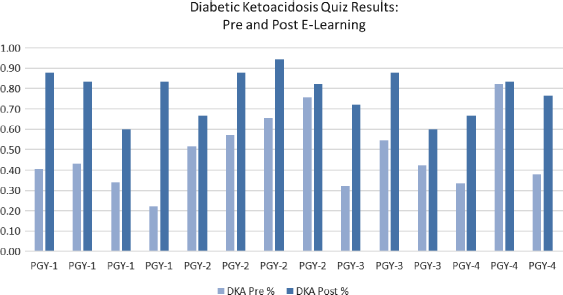
DKA module (individual precourse and postcourse scores).
Of the 15 residents, 12 completed the acute-onset hypertension in pregnancy and postpartum module. Overall, baseline knowledge of the residents was low prior to the blended learning course on acute-onset severe hypertension, 65.1% ± 12.1%. Postcourse quiz scores were significantly improved, 87.9% ± 7.6% and
Acute-onset severe hypertension module (paired sample test). Comparison of precourse test and postcourse test scores demonstrates a significant increase in test scores at the conclusion of the course. On average, scores increased by ~22%.


acute-onset severe hypertension in pregnancy and postpartum module (individual pre- and postcourse quiz results).
Asynchronous online discussion
Of the 14 residents who completed the DKA module, 11 participated in the online asynchronous discussion although there were eight original posts. Of the eight original posts, only two got responses from their peers. The discussions that generated responses were those in which clinical questions were posted. This type of post resulted in an asynchronous discussion by their colleagues (Fig. 3A). These questions were clarified during the face-to-face session (Fig. 3B).

DKA module. (
Of the 12 students who completed the acute-onset hypertension in pregnancy and postpartum module, 11 participated in the online asynchronous discussion. There were seven original posts. Three of these posts got six to seven responses from their peers. The posts were clear and thoughtful. Responses also demonstrated understanding of the problem presented in the problem-based case. In addition, peer-to-peer interaction was evidenced by the presence of linear asynchronous discussions, including suggestions on how to transfer what was learned in a clinical setting (Fig. 4). In comparison to the DKA module, there was more interaction and collaboration between the residents.

Acute-onset severe hypertension in pregnancy and postpartum module. A sample snippet of an asynchronous online discussion thread between residents on how to apply online content to improve patient care.
Residents' learning process
By day 3 of 7 of the DKA course, no resident had completed any of the tasks. Since the first three days were over a weekend, as the course was introduced on a Friday morning, the majority of residents were able to complete the precourse quiz and started viewing some of the multimedia presentations. Review of the activities log on Moodle demonstrated that no resident had logged into the course by day 3 of 7.
The leading author had to continually encourage the residents to participate in the online educational sessions. She personally called and requested her partners' assistance in reminding the residents to complete the tasks. Interestingly, one of her partners mentioned that even when some of the residents were not busy, they still did not spontaneously initiate the course. They had to be reminded to take the precourse quiz.
By day 3 of 7 of the module on acute-onset severe hypertension, half of the residents had completed the precourse quiz and reviewed the online content. By day 5 of 7, all but one had completed the quizzes and reviewed the course content. The last resident completed the postcourse quiz in the early morning of day 7. Also, the 11 residents who participated in the asynchronous online discussion had done so by the evening of day 5.
Unfortunately, the postcourse face-to-face discussion did not occur because of scheduling conflicts for this module. Instead, questions were answered and concepts were clarified online in the asynchronous discussion posts.
Students' evaluation
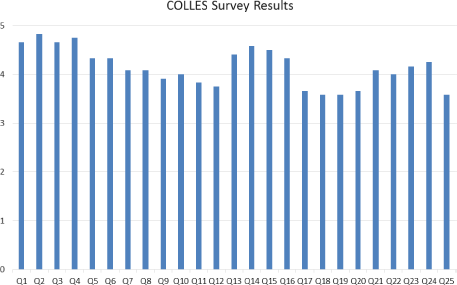
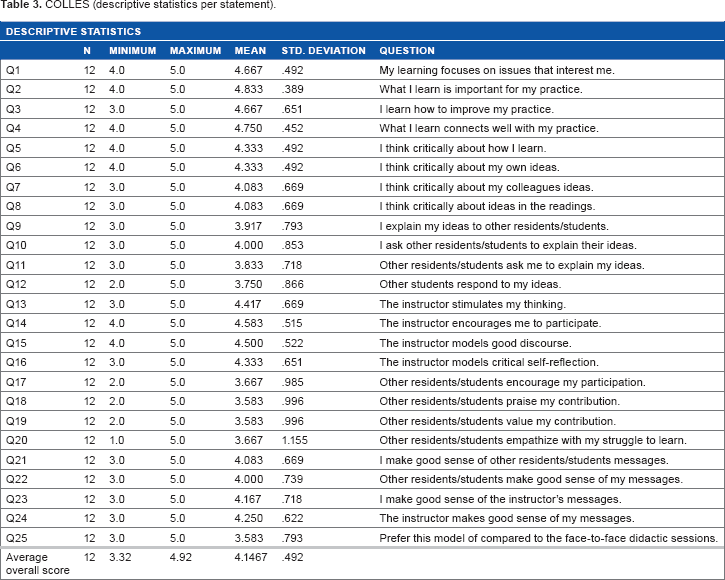
A total of 12 of the 15 residents completed the COLLES. They are the same residents who completed the module on acute-onset severe hypertension. Overall, the use of blended learning as a pedagogic tool was well received by the residents, with an average overall score of 4 out of 5 (Fig. 5). In all, 17 of the 25 statements received at least, on average, a score of 4 (Table 3). Statements regarding peer-to-peer interaction tended to have a lower score. In addition, of the 12 residents who completed the survey, seven gave a neutral score of 3 to question 25: “I prefer this model of learning compared to the typical face-to-face didactic sessions.”
COLLES statistics. Reference questions can be seen in appendix B.
COLLES (descriptive statistics per statement).
With regard to whether or not they liked the course format, 10 residents responded with a yes. Specific comments about the course format are as follows:
“I like online modules with pre- and post-tests.”
“It was easy to follow and the questions helped solidifying the learning.”
“Appreciate short videos—and articles to read pertaining to topic—allows completion as time allows.”
The two residents who did not respond with a yes stated “for the most part” and “not much time to be sitting at a computer.”
Positive aspects of the online course are as follows:
multimedia presentations,
inclusion of clinical pearls that are usually hard to find in textbooks within the multimedia presentations,
short duration of the multimedia presentations,
use of pre- and postcourse assessments, and
online and accessible nature of the course.
Overwhelmingly, what was disliked by five of the responders was the asynchronous online discussion. This was described as cumbersome to follow and disjointed. One participant felt forced to comment on another peer's post and often felt like they did not have anything new to contribute. Although one participant found it overwhelming having the responses on the discussion thread flood their email, they also thought it was nice to see responses.
All residents felt like they learned something. Six residents had no suggestions for the improvement of the course. Suggestions made by the remaining residents are as follows:
ensuring face-to-face discussion at the conclusion of each module,
having more articles or readings that could be saved for future reference,
not placing restrictions on time to complete the tasks,
making the complete course available from the beginning,
shorter precourse quiz, and
decreasing the requirements for asynchronous online discussion.
Implications
Based on the findings, this study demonstrates a positive impact on resident learning after adopting a blended learning approach to education as there was a notable increase in quiz scores. In addition, it appears that the multimedia presentations had a significant impact on learning and understanding. Having resources readily available on one site was a noted strength. Although the precourse quiz was deemed too lengthy by a few residents, it was also described as an effective tool in reinforcing the understanding of the cognitive skills learned by those same residents.
While the findings from the COLLES suggest acceptance of the majority of aspects of blended learning, they seem to be relatively indifferent in comparison to the traditional face-to-face approach to education.
Building a community of inquiry is important and challenging in this blended learning course. In comparison to the DKA module, there was a notable increase in peer-to-peer interaction in the asynchronous online discussions in the acute-onset severe hypertension module. Although this gave the impression of increased resident comfort with, and acceptance of, this mode of communication, the resident perception of peer-to-peer interaction was not as robust as initially assumed. For example, the residents felt like they had run out of things to discuss in the asynchronous online discussion posts. It appears that the asynchronous online discussions did not meet the desired goals of the blended learning format and likely had minimal impact on overall outcome.
As the residents are more task oriented, it is possible that including a more focused task, such as having the residents search the Internet for relevant articles on the topic and provide a brief discussion of their interpretation of the findings and potential impact on management schemes or patient care, might have been more effective in fostering discussion. It is also possible that this would satisfy their desire to have more literature available on the online learning management system.
Residency work hours have been restricted to no more than 80 hours a week. This is to minimize workplace fatigue and to allow time for self-directed learning. Based on discussions with the residents during the week of the DKA module, it seemed as if workplace responsibilities were overwhelming to them despite the reduced work hours. Interestingly, duty hour reports show that residents log in 65 hours a week on average. Despite resident impressions on time constraints, objective data suggested that time should not have been a significant factor in completion of modules.
Wonderings during the DKA module included stimulating learner motivation and encouraging self-directed learning. In order to address this, our introductory face-to-face session for the second module, acute-onset severe hypertension in pregnancy and postpartum, included an explicit conversation with the residents. Specifically, the lead author informed them of her expectations for the course, primarily completing tasks within a reasonable time frame in order to have adequate time to provide feedback to their answers and online discussion posts. The importance of maintaining professionalism, which includes completing tasks in a timely fashion, was also discussed. This conversation likely motivated them to complete the tasks for the acute-onset severe hypertension module expeditiously.
Previous reviews on learning effectiveness in traditional face-to-face instruction have demonstrated a direct correlation with effective communication. 20 Although instructors rate knowledge of subject as most important, students rate communication skills to be most important. 21 In-depth interviews of students demonstrate five attributes that are considered to be important for an effective instructor: rapport, delivery, fairness, knowledge and credibility, and organization. 22 The recurrent theme is that good instructors are good communicators. This is further defined as ensuring that sharing of meaning 20 exists between the sender and the receiver. This concept puts the onus on the sender to ensure that the receiver or student grasps the intended message by keeping them actively involved in the learning process.
Although these factors are specifically directed toward traditional face-to-face education, it can be adapted to distance education. Although we do not have data on the previous pedagogy, which was primarily face-to-face didactic sessions, we soon realized the importance of ensuring teacher presence in facilitating the community of inquiry and resident involvement in the online module, thereby fostering learning effectiveness. 13 We found this to be successful for the module on acute-onset severe hypertension and plan to implement this in future modules.
Conclusions
This pilot study suggests that blended learning can be a viable tool to support teaching and learning of OB/GYN residents. Although not a sought out outcome of this study, the benefit of this pedagogy is likely because of the benefits of multimedia presentations as an educational tool as they provide a framework that integrates learning theory with the human cognitive architecture.15,16 Blended learning not only provides education but also encourages self-directed learning and student interaction with the goal of incorporating knowledge into long-term memory. Although we would have liked to compare the outcomes of prior pedagogy to the blended learning approach, we did not perform pre- and posttesting of the previous face-to-face didactic approach. This was not feasible because of concerns that exposure to the subject matter in a face-to-face session would result in pretest cueing prior to the online modules.
There are four main limitations of this study. First, the study setting included only one graduate medical education program. Other programs with different curricula or with a different resident population may have different findings. The second limitation of this study is the small sample size, as it was implemented in a small teaching hospital. Whether or not findings would be reproducible in a larger residency program is unknown. Third, it was difficult to tease out the impact of prior experience in the management of these medical complications and resident precourse scores. This was, in part, because of the small sample size of the residency program and their team approach in managing patients on labor and delivery. Specific to the management of DKA, the obstetric service often consulted endocrinology, which limited direct resident involvement. In addition, charts of patients with acute-onset severe hypertension were reviewed. We noted that multiple residents and attending physicians were involved in the care of women with acute-onset severe hypertension. These factors hindered our ability to fully examine the resident experience with these medical issues and correlate them with their precourse scores. Last, post-module assessments were performed immediately after the completion of the module. Whether or not this short-term improvement will result in long-term retention and comprehension is unknown. This will be determined as follow-up assessments are planned later in the academic year. Upcoming blended learning modules will include the incorporation of questions from past modules into the precourse quizzes of newer topics. As we are interested in long-term retention, questions will be incorporated at least six months after the initial module was presented. In addition, to assess understanding and transferability, we have designed chart reviews. The purpose of these chart reviews is to objectively assess the impact of the modules on the resident's management scheme after the topics are presented.
This blended learning approach to teaching and learning was effective in improving the knowledge and understanding of DKA and acute-onset severe hypertension in pregnancy and postpartum. Although some might reason that the online learning sessions may be performed during resident off hours, thus increasing the time for more clinical responsibilities, we submit that the value of this pedagogy is the flexibility it provides to the residents. Because of the online nature of this pedagogy, the residents can be active in their learning process, controlling the time, pace, and place of instruction. This should not mean that the residents spend their off hours for these educational tasks. Rather, the residents should perform these tasks during previously appointed educational protected time and idle times on the wards.
Whether or not similar improvements will be noted in other obstetric or gynecologic topics is yet to be clarified. In addition, the topics of interest for this study were cognitive in nature. Topics that have a psychomotor component may not be amenable to this format. Based on the findings of this pilot study, especially the potential of blended learning to further resident knowledge and understanding, a blended obstetric curriculum is being developed. Future studies will be indicated to determine the role of blended learning in various topics, both obstetric and gynecologic.
Author Contributions
Conceived and designed: FT, HH. Analyzed data: KD. Wrote first draft: FT. Contributed to writing: FT, HH. Agree with manuscript results and conclusions: FT, HH, KD, EN. Jointly developed structure and arguments: FT, HH. Made critical revisions and approved final version: FT, HH. All authors reviewed and approved of the final manuscript.
Supplementary Materials
Appendix A
COLLES. Survey tool designed to assess student perception of online learning.
Appendix B
COLLES follow-up survey questions. Supplemental questions so learners can expand on their responses to COLLES survey.
Appendix C
Grading rubric for asynchronous online discussion.
Footnotes
Acknowledgments
We greatly thank our colleagues Ms. Kathy Groesch, RN, Dr. Pavlo Antonenko, PhD, and Dr. Paula Diaz-Sylvester, PhD, who provided insight that greatly assisted the research.