
Abstract
Objectives
To detail how human anatomy is currently being taught and assessed in Australian and New Zealand medical schools.
Methods
Medical schools in Australia and New Zealand were invited to respond to an online survey of their teaching and assessment of human anatomy in the 2018 academic year. The results are compared with 2008 data. Changes in curricula and teaching methods are reported.
Results
Despite robust media and academic discussion over the last decade, very little has changed in the amount of anatomy teaching or assessment of anatomy in Australasian medical schools. One exception is that most universities have invested in new technology for teaching; however, the use of new technologies is irregular.
Conclusions
Australian and New Zealand medical schools should actively and cohesively respond to the changing requirements for anatomy education, or risk being left behind our international counterparts in the provision of anatomy education, to the detriment of doctors’ training and the healthcare system.
Keywords
Introduction
It is difficult to quantify what represents an adequate amount of anatomy teaching in a medical degree, particularly in increasingly crowded medical curricula. The level of anatomy knowledge of junior doctors has been described in modern medical systems as ‘seriously lacking’ when compared to counterparts in previous decades, and as inadequate for basic clinical procedures (Herle & Saxena, 2011; Standring, 2009). Students have also expressed concern that the current level of anatomy teaching may be insufficient for them to become safe and competent junior doctors (Insull, Kejriwal, & Blyth, 2006; Mitchell & Batty, 2009). In 2008, we undertook a survey of anatomy teaching in Australian and New Zealand medical schools (Craig, Tait, Boers, & McAndrew, 2010). This was prompted by two factors, namely a perceived decline in the hours allocated to teaching gross anatomy – defined as anatomy at a macroscopic level or visible to the eye – in medical schools, and divergent opinions on what constituted sufficient anatomical knowledge to practise effectively as junior doctors.
The 2008 study was the first to provide a profile of the delivery of anatomy content to medical students in Australia and New Zealand. Considerable variability in the quantity and delivery of anatomy teaching was reported. The study highlighted the absence of a national curriculum or framework to guide the teaching of anatomy, including in terms of time, content and assessment. Since that study in 2008, the teaching of human anatomy in medical schools has been discussed extensively in the academic literature and popular media, both in Australia (Farey, Sandeford, & Evans-McKendry, 2014; Garg, 2018) and internationally (Bergman, Van Der Vleuten, & Scherpbier, 2011). In Australia and New Zealand, there is still no input from a national body into core anatomy curriculum, nor are there consistent national assessment standards. The American Association of Anatomists (2019) has revised and published recommended learning objectives for anatomy teaching in medical schools, following on from recommendations formed by a taskforce that first addressed the issue in 1997. In the United Kingdom and Ireland, the Anatomical Society published a Core Regional Anatomy Syllabus, which recommended learning outcomes for undergraduate medicine, and influenced anatomy curricula in a number of universities (Smith et al., 2018; Smith, Finn, Stewart, & McHanwell, 2016). More broadly, the International Federation of Associations of Anatomists is developing core syllabuses for the teaching of anatomy in a number of anatomical areas, with the aim of providing internationally recognised standards for anatomy education in clinical and scientific professions (Moxham, McHanwell, & Berkovitz, 2018; Moxham, McHanwell, Plaisant, & Pais, 2015; Moxham, Plaisant, Smith, Pawlina, & McHanwell, 2014; Tubbs et al., 2014). Gulf Cooperation Council (GCC) countries recognise challenges with little collaboration between anatomy departments across 20 surveyed GCC medical schools. Interestingly, this recent study identified that 55% of surveyed GCC medical schools had changed their curricula between 2005 and 2015, of which 73% decreased their anatomy teaching hours (Al Mushaiqri, 2015).
Since the 2008 study, various authors have referred to a changing landscape of anatomy education (Bokey, Chapuis, & Dent, 2014; Guimaraes et al., 2017) characterised by a shift towards problem-based learning – where knowledge is taught in the context of clinical scenarios and is largely self-led – the loss of suitably trained staff, a decline in the availability and an increase in the cost of cadaveric resources, and advances in electronic and software teaching technologies (Bergman et al., 2011; Guimaraes et al., 2017). In addition, the need to allocate teaching time to other important and developing areas of medicine, such as medical genetics, has constrained available teaching time (Guimaraes et al., 2017). A rapid expansion in the number of medical students (1660 commencing students in the year 2000 more than doubled to 3433 in 2008 with further, though more moderate, increase to 3822 in 2018) has also posed logistical constraints on the traditional dissection-based approach to teaching gross anatomy (Health Workforce Australia, 2014; Medical Deans Australia and New Zealand, 2019).
This current paper reports the results of a follow-up study to the one conducted in 2008 using the same research methods. Like the previous one, the current study seeks to detail how human anatomy is being taught and assessed in Australian and New Zealand medical schools in 2018. The results are compared with 2008 data and changes in curriculum structure, teaching resources, staffing and assessment are reported.
Methods
An online survey invitation was emailed to the Head of Department, or equivalent senior staff member responsible for coordinating anatomy teaching, in each medical school (n = 22) in Australia and New Zealand.
Survey questions replicated the original survey in 2008. Some additional questions were included regarding postgraduate anatomy teaching and the adoption of teaching technology. Respondents were asked to complete the survey in respect of the 2018 academic year. The study was approved by the University of Wollongong’s Human Research Ethics Committee (ethics approval number: 2018/372).
Seventeen of the 22 medical schools in Australia and New Zealand (77%) responded (Table 1). Four of the 19 medical schools that participated in the 2008 survey did not respond in 2018 (Craig et al., 2010). No systematic non-response could be detected in that medical schools which did not respond in 2018 represent both undergraduate and postgraduate entry pathways with course length between four and seven years, located in three different states of Australia and one in New Zealand. The 2018 survey results include one medical school that did not participate in 2008 and one that has been established since 2008. Each medical school was asked to comment on their course structure; teaching time devoted to anatomy; technologies used in the classroom; and staff, methods and standards for assessment.
Medical schools participating in the survey.

Results
Gross anatomy teaching structure
Fifteen of 17 (88%) courses integrated gross anatomy teaching with other content. This was most commonly in a regional or system-based approach linked with clinical cases. Some medical schools integrated anatomy teaching with other disciplines/themes such as, but not exclusively, clinical skills (nine schools, 53%), physiology (six schools, 35%), pathology (four schools, 24%), radiology (three schools, 18%) and histopathology (two schools, 12%). Most commonly gross anatomy teaching was integrated with clinical skills plus another discipline/theme.
Ten of 17 (59%) courses provided all of their gross anatomy teaching within the first half of their course. Only three courses (18%) reported that they taught gross anatomy in the final or penultimate year of the medical course. The average number of gross anatomy teaching hours an Australian or New Zealand medical student received throughout their course was 194.6 (range 62–453, median 173.5). The average number of hours per year of gross anatomy teaching by course length is presented in Table 2.
The average number of hours of gross anatomy teaching by course length (min/max).
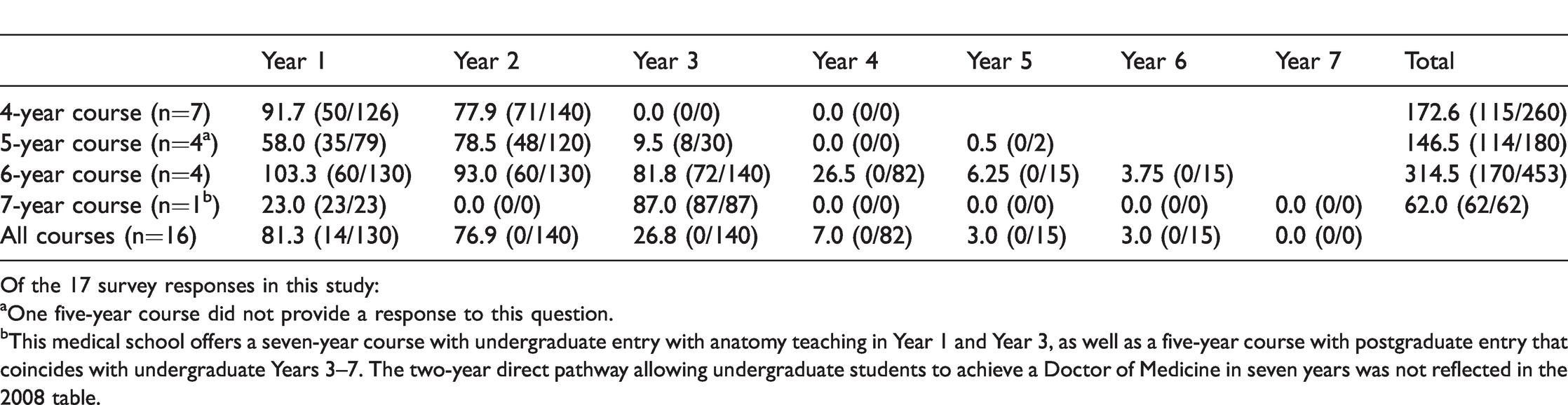
Of the 17 survey responses in this study:
aOne five-year course did not provide a response to this question.
bThis medical school offers a seven-year course with undergraduate entry with anatomy teaching in Year 1 and Year 3, as well as a five-year course with postgraduate entry that coincides with undergraduate Years 3–7. The two-year direct pathway allowing undergraduate students to achieve a Doctor of Medicine in seven years was not reflected in the 2008 table.
Teaching resources
The most frequently used resource for teaching anatomy in 2018 was prosected human material: 76% of courses used it in every session and 18% used it for most sessions (Table 3). In 2008, 100% of courses surveyed used prosected material for teaching in every or most sessions. Models were also commonly used to teach anatomy: 76% of courses used them in every or most sessions in 2018, similar to the incidence reported in 2008 (79%). Computer generated images and radiologic imaging were used, to some extent, by all courses to teach gross anatomy. However, in 2018, more courses used computer generated images in most or every session (58% in 2018 compared to 28% in 2008). Similarly, the use of medical imaging in most or every session increased from 61% in 2008 to 76% in 2018. The use of plastinated specimens in 2018 increased from 9 of 19 (47%) in 2008 to 11 of 17 courses (65%) that taught with these specific resources.
Resource use for teaching gross anatomy.
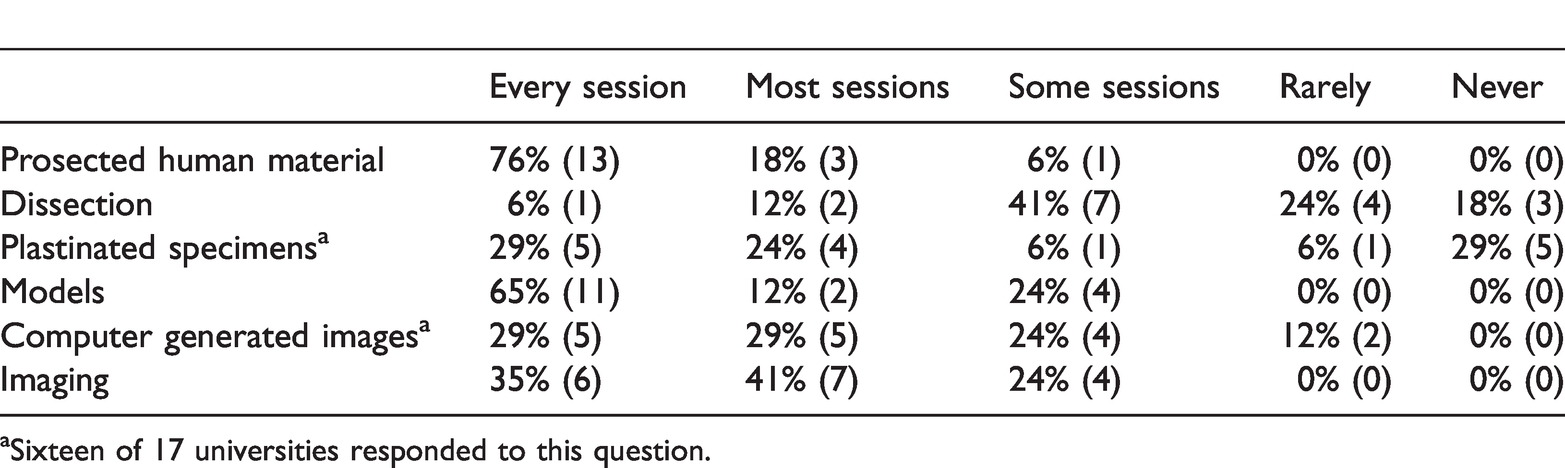
aSixteen of 17 universities responded to this question.
In 2018, human dissection was available in 14 of 17 (82%) medical schools, similar to 2008. Of these, one medical school offered comparative dissection only – using animal cadavers. Another four offered dissection as an optional elective. When dissection was offered as a core module, only 40% of courses provided direct supervision and guidance by a surgeon or anatomist during dissections. More commonly, a dissection manual supplemented by pre-recorded audiovisual instruction was the predominant resource to guide dissection. Reciprocal peer teaching was also employed. The most comprehensive dissection experiences, in terms of supervision, hours and systematic dissection, were described by universities that offered dissection as an elective.
In the 10 years since the initial survey, almost all universities (82%) had invested in advanced teaching technologies such as ultrasound machines, tablet devices, interactive e-books and casting software to develop presentations. Fifty nine per cent of Australian and New Zealand medical schools reported purchasing progressive technologies such as 3D printing and interactive virtual reality software, including HTV Vive headsets and multi-touch Sectra screens (to allow anatomy exploration and virtual dissection), 4D Augmented Reality software (such as Hololens) and video-enabled glasses to help tutors to guide dissection. Despite these investments, progressive technologies were only partially applied in anatomy teaching. Fourteen of 17 universities (84%) used e-book anatomy atlases and 12 universities (71%) used 3D software to display imaging. Only seven universities (41%) ever used virtual reality, three (18%) used virtual dissection, three (18%) used Hololens and one (6%) used a haptic system in some sessions.
Staffing
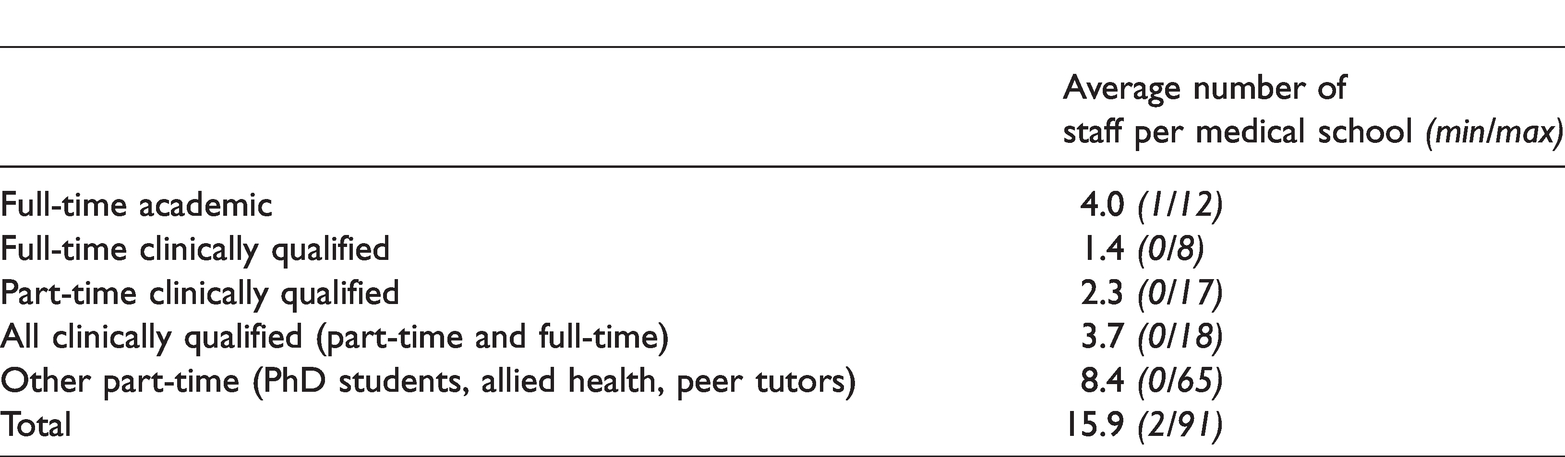
On average, 16 staff per medical school were involved in teaching gross anatomy. Of these, on average, four were full-time academic staff and another 3.7 were clinically qualified staff, either full-time or part-time (Table 4). In 2008, we reported that on average there were three full-time academic staff and 3.5 clinically qualified staff, hence there has been little change in staffing between the study periods.
Type and average number of staff involved in teaching gross anatomy per medical school.
Assessment
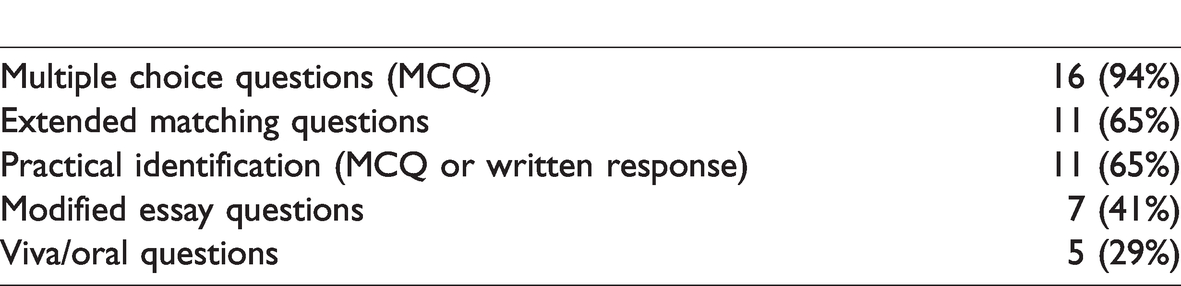
Most courses used a combination of formats for assessment of the comprehension of gross anatomy (Table 5). All courses integrated summative anatomy assessment into the assessment of other core disciplines, usually in a theme-based or clinical scenario setting. Of these, eight (47%) described separate practical or written summative anatomy examinations. Other courses incorporated dedicated anatomy spot tests or oral quizzes as part of formative assessment. Compared to 2008, a similar proportion of medical schools required students to complete specific anatomy assessment in either a formative or summative context. Only three (18%) courses required a specific pass for anatomy to progress to the next phase of the course. This number decreased from the 2008 data (eight courses, 38%).
Format of assessment of gross anatomy comprehension.
Discussion
The results suggest that since anatomy education in Australian and New Zealand medical schools was first profiled in 2008, and despite significant media attention and rigorous academic discussion, very little has changed to the structure of anatomy teaching. There has been little change in the time allocated to gross anatomy teaching, or to the distribution and qualification of teaching staff. No standardised assessment of anatomy knowledge has been instituted. The average anatomy teaching hours in 2018 for all courses was 195, compared to 171 in 2008. We found no association between the total teaching hours and the type of medical course, or with the use of teaching technology. However, we observed that of the medical schools providing anatomy teaching hours above the median, nearly all (88%) used dissection or cadaver specimens in every session, but the incidence of this was lower in medical schools that were below the national median for anatomy teaching hours. One respondent described that an institutional barrier to changing the overall number of hours of anatomy teaching is having a fixed time allocation within the timetable of the medical school; this may be true of other medical courses and is likely to remain unchanged in the absence of a major curriculum review. Inadequate funding to employ or upskill teaching staff in new methods or technologies, and the absence of curriculum standards from a national body to compel revision of current courses are also plausible explanations for the lack of change to the structure of anatomy teaching.
There has been a notable change in the availability and uptake of technological adjuncts that aid learning in the field of anatomical sciences (Guimaraes et al., 2017). Technological adjuncts have the potential to compensate for reduced teaching hours and to facilitate access to traditional methods of learning by cadaveric dissection exposure. However, their reception and uptake has been varied. In 2014, authors representing the Australian Medical Students’ Association expressed the view that ‘time-intensive methods of instruction such as dissection should be a rite of passage for medical students in the absence of evidence demonstrating the superiority of modern teaching methods’ (Farey et al., 2014, p. 814). The observed uptake of technological adjuncts points to the possibility that medical schools are substituting more time efficient, technology-driven learning for less time efficient, face-to-face learning of anatomy. However, we did not find an association between the number of teaching hours and medical schools that most strongly implemented new teaching technology.
A meta-analysis published in 2018 of the efficacy of various teaching methods used in anatomy education over the last 50 years demonstrated that there was no short-term benefit of dissection when measured by knowledge-based examination, compared with other laboratory-based methods of education such as prosection, anatomical models, and virtual or digital media (Wilson et al., 2018). In contrast to the strong preference for dissection experience expressed by many student groups and educators (Garg, 2018; Wilson et al., 2018), evidence suggests this is no longer the ‘gold standard’ for the attainment of anatomical knowledge (Barmaki et al., 2019; Liu et al., 2016; Maresky et al., 2019). We observe that whilst technology-based teaching aids are being adopted by medical schools in Australia and New Zealand, these are likely used as adjuncts only and have not yet replaced traditional methods, as prosected specimens had a similar level of use in both surveys. Recent data from the Association of American Medical Colleges have noted a higher uptake than in Australia and New Zealand of virtual/online tools and anatomical models/simulators, though similar to Australia and New Zealand, use of cadaveric and plastinated specimens remains prominent. Virtual tools were employed frequently in the teaching of areas of subspecialty-specific anatomy that often have more difficult spatial concepts (Association of American Medical Colleges, 2019). In GCC medical schools, dissection is used infrequently (difficulty in obtaining additional cadavers without national donation programmes is one barrier); however, prosections are the most used tool. Prosections refer to a cadaveric specimen that has already been dissected by an experienced anatomist in order to demonstrate particular structures. The prosected specimen can be displayed repeatedly in anatomy laboratory teaching. This differs from dissection which is a method of learning anatomy whereby the student is actively involved in dissecting a cadaveric specimen to identify the various structures; this necessitates a new cadaver specimen for each dissection. Of 11 GCC medical schools that had changed their medical school curricula in the past decade, 73% reported changing their method of teaching anatomy to become ‘more innovative’, although 14 of the 20 surveyed GCC medical schools had never or rarely used simulation software (Al Mushaiqri, 2015).
Medical practice has changed markedly in recent decades. There is growing sub-specialisation and progressive use of minimally invasive techniques of diagnosis and treatment. The use of computer and medical imaging to teach anatomy increased in 2018. This perhaps reflects the improved quality of available software programs and greater reliance on medical imaging in the clinical workforce. Similarly, endoscopic and laparoscopic technology provides opportunity to visualise the human body from new vantage points, and support a shift towards anatomy education that enables students to develop 3D maps of the body with adjuncts such as 3D printing, 3D models, 3DTV and Virtual Reality (Guimaraes et al., 2017). It is difficult to sensibly argue that a doctor should enter a surgical or radiological training pathway without having studied a prosected cadaver. However, traditional prosection-based methods of teaching anatomy in isolation are unlikely to adequately equip junior doctors to interact with the available technology and treatments in the clinical environment. In the present survey, eight universities reported offering a postgraduate anatomy qualification. This reflects the trend away from anatomy taught purely by anatomy departments within a medical school, towards anatomy teaching in postgraduate stand-alone qualifications or by universities without medical schools (Flack & Nicholson, 2016). Elective dissection and other postgraduate anatomy courses fulfil a perceived need and may indicate the likely future direction of anatomy education in Australia and New Zealand.
Assessment of comprehension level of anatomy knowledge in Australian and New Zealand medical schools varies substantially between institutions and remains non-standardised at a national level. In the absence of a compelling reason to revise an anatomy curriculum, it is possible that in another 10 years medical schools in Australia and New Zealand will still have made only small, uncoordinated steps towards advancing anatomy education. In the United Kingdom, a specialty training college reported the effectiveness of its approach to establishing a consensus for a national curriculum (Kilroy & Driscoll, 2006). Smith et al. (2018) described the positive reception by students and anatomists in the United Kingdom of a Core Regional Anatomy Syllabus published by the Anatomical Society in 2016. They reported that, even without compulsory compliance, the core syllabus prompted in-house review of learning objectives by institutions involved in teaching anatomy (Smith et al., 2018). We can see a role for a national body or consortium that would develop an evidence-based framework for anatomy education in Australian and New Zealand, including the establishment of a consensus curriculum, or the adoption of core syllabuses such as those being developed by the International Federation of Associations of Anatomists (2019) Core Syllabuses Project or the American Association of Anatomists (2019) Anatomical Competencies Project. There is scope too for a wider capacity building role: to support the development of staff skills, facilitate technology acquisition, standardise assessment benchmarks and promote ongoing quality assurance.
The limitations of this study include those inherent in survey-based data gathering and analysis, such as voluntary response bias and responder recall (Ponto, 2015). Furthermore, the medical schools which responded to the 2018 survey were not identical to those that responded in 2008. This affects our ability to draw direct comparisons between the results of the two studies. Nonetheless, the capacity to highlight trends in anatomy teaching within the Australian and New Zealand medical school community as a whole is not precluded. We would also highlight that quantitative changes, or lack thereof, do not necessarily reflect changes in the quality of teaching. Programmes with rigid time allocations may have adapted their learning activities to meet current learning requirements and improve the quality of their courses, without necessarily increasing technology acquisition or anatomy teaching hours, though this could not be determined from the current study design.
Although modern medical practice continues to rapidly evolve, there appears to be little practical change to anatomy education in Australian and New Zealand medical schools in the past decade. Universities should actively and cohesively invest in solutions to keep pace with the changing requirements of anatomy education to ensure that junior clinicians receive the necessary knowledge for clinical practice or risk becoming ‘stuck in time’.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.