
Abstract
Bipolar disorder is a complex condition to treat because agents that may be effective for a specific phase may not be effective for other phases, or may even worsen the overall course of the illness. Over the last decade there has been an increase in research activity in the treatment of bipolar illness. There are now several agents that are well established for the treatment of acute mania (lithium, divalproex, carbamazepine, nearly all antipsychotics), acute bipolar depression (lamotrigine, quetiapine, olanzapine/fluoxetine combination), and relapse prevention (lithium, lamotrigine, divalproex, most second generation antipsychotics). There are also novel treatments that are being studied for all three phases. These include eslicarbazepine, cariprazine, MEM-1003, memantine, tamoxifen and pentazocine for acute mania; pramipexole, modafinil, armodafinil, divalproex, lurasidone, agomelatine, cariprazine, lisedexamfetamine, riluzole, RG-2417, bifeprunox, ropinirole, GSK1014802, and magnetic stimulation for bipolar depression; and asenapine, lurasidone, and cariprazine for relapse prevention. Additionally, there are accumulating data that antidepressants, particularly serotoninergic ones, are not particularly effective in acute bipolar depression and may worsen the course of the illness.
Introduction
Bipolar disorder is a severe psychiatric illness that can have both good prognosis forms and bad prognosis forms. For a long time research into the course and treatment of bipolar illness had lagged behind advances in the treatment of major depression. In the 1970s and 1980s much of the data garnered for major depressive disorder was simply applied to the treatment of bipolar patients without adequate testing or research. However, beginning in the 1990s, an expansion of bipolar research has well informed clinical care. This expansion of research has led to several established treatments, and some emerging therapies. This paper reviews the current psychopharmacology of bipolar illness, and explores promising treatments currently in development.
Psychopharmacotherapy of Mania
Reasonable Options for the Treatment of Acute Mania.
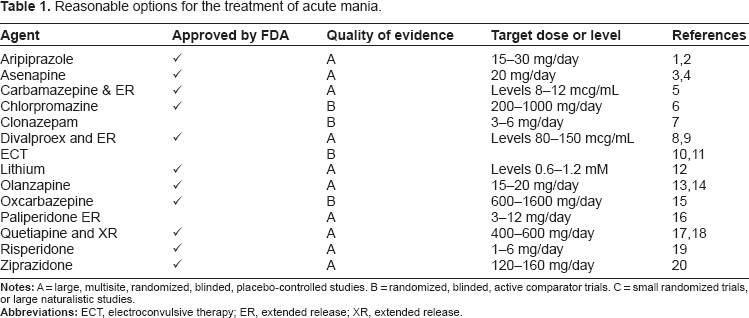
Notes: A= large, multisite, randomized, blinded, placebo-controlled studies. B = randomized, blinded, active comparator trials. C = small randomized trials, or large naturalistic studies.
Abbreviations: ECT, electroconvulsive therapy; ER, extended release; XR, extended release.
In addition to the agents in Table 1, there are several new agents currently being studied for use in acute mania.
Eslicarbazepine (Stedesa™ in the United States; Zebinix®, Exalief® in Europe; chemical name (S)-(-)-10-acetoxy-10,11-dihydro-5H-dibenz[b,f]azepine-5-carboxamide; development name BIA 2-093) is a new dibenzazepine antiepileptic drug. 25 Like most effective mood stabilizing anticonvulsants, 26 it is a high affinity antagonist of the voltage-gated sodium channel. Eslicarbazepine is administered as the acetate salt which is rapidly and nearly completely reduced by esterases in the liver to the S enantiomer, S-licarbazepine or eslicarbazepine, which is the active metabolite of oxcarbazepine. 25 Eslicarbazepine has similar affinity to inactivated sodium channels (channels in just activated neurons) as carbamazepine, and greater efficacy in animal models of seizure than oxcarbazepine. Studies for bipolar disorder are currently underway but the results are not yet available. However, given the known efficacy of both carbamazepine and oxcarbazepine (Table 1), it is highly likely that eslicarbazepine will also be effective in acute mania.
Cariprazine (RGH-188) is an antipsychotic with the profile of D3-preferring dopamine D3/D2 receptor partial agonist.
27
Increased relative affinity for D3 over D2 may confer cariprazine with antipsychotic efficacy as well as the potential for augmented effect on negative and cognitive symptoms of schizophrenia,
28
and fewer extrapyramidal symptoms (EPS).
29
It has been found to be effective in animal models for mania.
30
Monotherapy and add-on to mood stabilizer studies in acute mania are ongoing (
MEM-1003 is an L-type calcium channel antagonist that is still in development by Memory Pharmaceuticals. A study of its utility in acute mania has been recently completed, but its results are not available (
Memantine (Nemenda) is a moderate-affinity, uncompetitive N-methyl-D-aspartate receptor (NMDAR) antagonist, 35 approved for moderate to severe Alzheimer's disease. 36 It reduces manic symptoms in an animal model of mania. 37 In one small (n = 33) open, multicenter study of memantine administered in doses of 20-30 mg/day, 20-30 mg/day, or 30-50 mg/day, all patients improved over the 21 days of the study, but patients receiving 20-30 mg/day had the greatest improvement. 38
Tamoxifen (Nolvadex, Istubal, Valodex) is an estrogen receptor antagonist that also inhibits protein kinase C (PKC), a mechanism that is shared by both lithium and valproic acid. 39 Tamoxifen antagonizes manic-like behavior in a rat model of mania. 40 As proof of concept, tamoxifen was administered to manic bipolar subjects in small, placebo-controlled double-blind studies as monotherapy41, 42 and adjunctive to lithium. 43 Despite significant evidence, tamoxifen would only be used in bipolar patients in very unique circumstances. However, these studies do demonstrate the utility of PKC inhibitors as a potentially novel class of antimanic agents. 39
Pentazocine (Talwin, Fortral) a κ opioid receptor antagonist frequently used for pain control was administered openly to manic patients for a single dose. One hour after administration manic symptoms were significantly reduced. 44 While the authors argue that this may suggest an antimanic effect, it should be remembered that stimulants, such as amphetamine, may also reduce manic symptoms acutely,45, 46 but these agents are not believed to be antimanic.
Psychopharmacotherapy of Depression
Bipolar depression is the major clinical challenge in the treatment of bipolar disorder. Depression is more common than either mania 47 or hypomania. 48 However, a series of randomized trials have repeatedly found that antidepressants added to mood stabilizer are not better than mood stabilizer alone. 49 Antidepressants may increase the risk for manic switch, rapid cycling, or a chronic irritable dysphoric state known as antidepressant-associated chronic irritable dysphoria (ACID).50, 51 For individuals with rapid cycling, antidepressant treatment may increase the risk for future depression. 52 In other words, antidepressants do not appear to be helpful for the treatment of bipolar depression, and may be harmful.
Reasonable Treatment Options for the Treatment of Bipolar Depression.
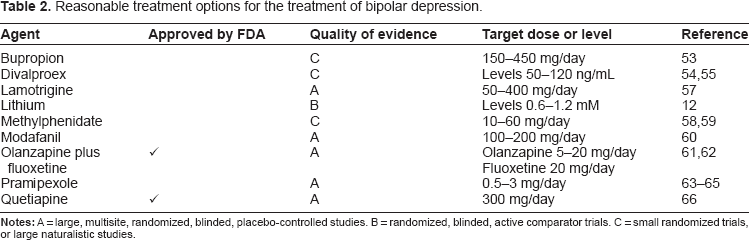
The only other FDA approved treatment for bipolar depression is the olanzapine/fluoxetine combination (Symbiax™). 69 A 24-week open extension found that the risk for manic induction due to the coadministration of fluoxetine was low, but 27.4% relapsed into depression. 70
Modafanil (Provigil), a non-stimulant agent that is used to increase alertness in subjects with daytime sleepiness due to a variety of conditions, has been tested as an adjunctive agent in depressed bipolar subjects who were randomly assigned to have modafanil (n = 41) or placebo (n = 44) added in a blinded manner. 71 Response, defined as at least 50% improvement, was twice as great in modafaniltreated subjects (44%) compared to placebo (23%, P < 0.05). 71 In the brief 6 week-study, there was no apparent increase in the manic or hypomanic-induction rate. 71 The R-isomer of racemic modafinil, armodafinil, has been examined in depressed type I bipolar patients in a double-blind placebo-controlled, add-on study. 72 Despite a high placebo response rate, armodafinil was marginally but significantly superior to placebo. 72
Pramipexole (Mirapex), a dopamine agonist, is effective in both type I and type II bipolar patients in two short-term placebo-controlled studies.73, 74 Among the two reports, total of 15 with type I and 28 patients with type II were studied over 6 weeks. Response occurred in 60%-67% of patients taking pramipexole and 9%-20% taking placebo.73, 74 The 6 week duration or the studies is too brief to determine long term safety, but in a 48 week follow-up of 23 patients (12 with major depression and 11 with bipolar disorder), 27% (two subjects developed hypomania and one developed psychotic mania) experienced a switch. 75 This seems like a high rate, but many of the subjects were also receiving antidepressants.
Lurasidone (SM-13496) is a new second generation antipsychotic (SGA) that has just been approved by the FDA for the treatment of acute psychosis in schizophrenia. As with all SGAs, lurasidone has high affinity to the serotonin 5HT2A and dopamine D2 receptors. However, unlike most other SGAs, the affinity for the D2 receptor is greater than 5HT2A. 76 It also has high affinity to 5HT7 receptor and is a partial agonist at the 5HT1A receptor. 77 Phase III studies as monotherapy and concomitant treatment with lithium or valproic acid for bipolar depression were started in April 2009 and are known by the acronym PREVAIL (Program to Evaluate Antidepressant Impact of Lurasidone). 76 Results have not been reported yet.
Cariprazine at 0.25-0.75 or 1.5-3 mg/day has been studied for bipolar depression in an 8-week, placebo-controlled study that ended in June 2010 (
Lisedexamfetamine (Vyvance) is FDA approved for attention deficit disorder. It is a prodrug that is slowly metabolized into amphetamine in the blood. Amphetamine
78
and methylphenidate
79
have both been used for bipolar depression. However, the rate of stimulant-associated mania or hypomania may be as high as 40% in the naturalistic setting
80
despite being nonexistent in the setting of acute treatment.79, 81 Nonetheless, a double blind, placebo-controlled study of lisedexamfetamine in bipolar depression was started in January 2010 and is ongoing at this point in time (
Riluzole (Rilutek) is a sodium channel antagonist 82 that is approved by the FDA for amyotrophic lateral sclerosis (ALS). 83 It was tested in an open study of 14 patients with bipolar depression who were receiving lithium for at least 4 weeks. Riluzole was added to the lithium and the dose was increased to 100 mg twice daily for an additional 8 weeks. 84 Compared to their baseline, patients improved significantly beginning in week 5 of riluzole treatment. There appeared to be a dose related effect where 66% of those receiving doses at or greater than 200 mg/day responded, but only 33% of those receiving lower doses responded. 84 However, with an annual cost exceeding $4,000 and a nearly impossible prior authorization hurdle, it is unlikely that riluzole will even be studied in larger trials.
RG2417, an oral formulation of uridine, has been investigated its effectiveness in bipolar depression by Repligen. Due to reports of mitochondrial dysfunction in bipolar illness, Uracil is a pyrimidine that is required for RNA synthesis, and is important for mitochondrial function, uridine is ribosylated uracil. None of their findings have been reported in the scientific literature, but business reports show that the drug has had a favorable outcome in phase IIa studies, and is currently undergoing investigation in phase IIb studies. In the original phase IIa study, 83 depressed bipolar patients were given RG2417 for 6 weeks. The improvement in depressive symptoms was quite modest, but was greatest in the most difficult patients—those who had more depressive episodes, suggesting that it may play a role for adjunctive treatment (
Agomelatine is an agonist of melatonin 1 and 2 receptors and an antagonist of serotonin 2C receptors. It is used as an antidepressant in Europe (Valdoxan, Melitor, Thymanax). In a small open add-on study to lithium or valproic acid, agomelatine shows efficacy for bipolar depression. 85
Several other agents have potential to help people with bipolar depression. Bifeprunox is a partial agonist at the dopamine D2 receptors and the serotonin 5-HT1 A receptors (
Rapid transcranial magnetic stimulation (TMS) has been approved by the FDA for treatment-resistant depression. In several small studies, mostly open and uncontrolled, TMS has been found to be effective in bipolar depression; 88 one small study finds that slow right-sided stimulation may also be effective. 89 It is likely that future controlled studies will document efficacy of TMS in bipolar depression. This is because reduction in left prefrontal brain activity utilization is shared in both bipolar and unipolar depression,90, 91 and TMS corrects that abnormality. 92 Unfortunately, there is inadequate data on the duration of the response, and inadequate guidance regarding continuation TMS.
Electroconvulsive therapy (ECT) is an underutilized treatment that effective for both unipolar and bipolar depressed patients who are resistant to pharmacological treatment. Actually, bipolar depression may improve more rapidly than unipolar illness with ultra brief pulse treatment. 93 ECT has also been shown to be effective in bipolar mixed states in which depression and mania coexist. 94 Cognitive complication of ECT can be reduced by utilizing bifrontal (instead of the typical bitemporal) electrode replacement and maintain the same efficacy. 95 However, patient acceptance of ECT remains poor, and use of anesthesia complicates its administration.
Psychopharmacotherapy: Relapse Prevention
Reasonable Treatment Options for Relapse and Recurrence Prevention

Divalproex was studied in a 12-months relapse-prevention study. It was a randomized, placebo-controlled, lithium-comparison study, but it was not an enriched design (ie, it did not preferentially recruit patients that had responded to lithium or divalproex). 96 Neither lithium nor divalproex separated from placebo in this study. However, a post-hoc subanalysis revealed that patients who had a history of previous good acute response to divalproex had significantly fewer relapses if they remained on divalproex compared to those that were randomized to placebo. 97
Oxcarbazepine has been studied in a 52 week randomized assignment comparing its use when added to lithium (n = 26), versus placebo added to lithium (n = 29) in euthymic type I and II bipolar subjects with at least 2 episodes in the previous 12 months. The combination was numerically superior to lithium alone, but none of the parameters reached statistical significance. 98 Given the small size of the study, the data actually suggest that oxcarbazepine added to lithium might be superior to lithium alone. 98
While long-acting injectable antipsychotics have long been advocated for maintenance treatment in difficult patients, 99 it has only been recently that a long-acting injectable antipsychotic has been approved by the FDA for maintenance treatment on bipolar disorder. 100 In two placebo-controlled trials with risperidone Consta™, the drug was associated with reduced relapse rates, reduced symptomatic load, and greater time to relapse than both oral medication or placebo injections. 100 The effect was driven by the prevention of mania, with minimal effect on the prevention of depression.
Asenapine has been approved for acute treatment of mania, and has been studied in a 40-week extension comparing it with olanzapine as monotherapy. 101 Outcome with both active medications was similar. 101
Cariprazine is being studied in a 16-week maintenance trial, but data are not yet available (
Summary
Clinical bipolar research remains an active field. Pharmaceutical development involves known approaches such as sodium channel antagonists and antipsychotic medications, but also novel approaches that involve mitochondrial pathways and second messengers. None of the agents represent a huge breakthrough in treatment because the pathophysiology of bipolar illness remains unknown. The limited investment in this area of research contributes to the relatively slow rate of progression and the dearth of truly novel approaches with the one exception of TMS.
Most new approaches are variations of the current options. These include several antipsychotic agents (cariprazine and lurasidone), stimulants (lisedexamfetamine), and anticonvulsants (oxcarbazepine and eslicarbazepine). These agents provide additional options without significant additional benefit. It remains unclear whether more novel approaches such as modafinil and armodafinil, pramipexole, riluzole, and memantine, will actually provide a clinical leap for bipolar patients.
Additionally, there are access issues with many of the newer medications. TMS is generally not covered by insurance and is quite expensive (generally approximately $10,000 for a 6 week treatment course). Riluzole is similarly extraordinarily expensive. Off label third party approval for such agents as modafinil, armodafinil, pramipexole, or memantine can be difficult or impossible. Eslicarbazepine is not available in the United States. ECT, even with improved techniques, remains stigmatized. Thus, along with newer approaches, administrative changes that reduces hurdles to access will be required.
Nonetheless, over the near future, clinicians can expect their treatment options to expand.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.