
Abstract
Obsessive–compulsive disorder (OCD) is a neuropsychiatric illness that often develops in childhood, affects 1%–2% of the population, and causes significant impairment across the lifespan. The first step in identifying and treating OCD is a thorough evidence-based assessment. This paper reviews the administration pragmatics, psychometric properties, and limitations of commonly used assessment measures for adults and youths with OCD. This includes diagnostic interviews, clinician-administered symptom severity scales, self-report measures, and parent/child measures. Additionally, adjunctive measures that assess important related factors (ie, impairment, family accommodation, and insight) are also discussed. This paper concludes with recommendations for an evidence-based assessment based on individualized assessment goals that include generating an OCD diagnosis, determining symptom severity, and monitoring treatment progress.
Introduction
A comprehensive evidence-based assessment is a critical step in accurately identifying the presence and severity of obsessive– compulsive disorder (OCD) in both clinical and research practice. Obsessive–compulsive symptoms can be difficult to assess, given that they are often manifested internally, and individuals with OCD may not be inclined to recognize and report symptoms (ie, limited insight). In response to these challenges, this paper reviews commonly used OCD measures that have been examined in research studies to enhance clinicians' abilities to detect and monitor OCD symptom severity during assessment and treatment. First, the pragmatics of measure administration and psychometric properties are reviewed. Clinician-rated measures are discussed initially, followed by adult self-report measures, and finally parent/child measures. Second, the incorporation of additional important factors in an evidence-based OCD assessment is discussed (ie, impairment, family accommodation, and insight). Finally, this paper concludes with recommendations for an evidence-based assessment based on individualized assessment goals and empirical support.
Several factors are important to consider when developing an evidence-based assessment battery. First, one must identify the primary aim of the assessment and prioritize measures in line with this goal. For example, measures with strong diagnostic sensitivity might be prioritized when screening for symptoms. Comparatively, when confronted with a differential diagnosis (eg, distinguishing OCD from an anxiety disorder or depression), diagnostic specificity would take precedence. Similarly, when monitoring changes in symptom severity during treatment, reliance on assessment tools with demonstrated treatment sensitivity would be prioritized. Thus, a pragmatic framework is useful to inform measure selection to meet the aforementioned aims. Within this framework, the clinician is guided by knowledge of what tool may be most useful, feasible, and accurate in a specific situation.1,2 Accordingly, familiarity with the armamentarium of evidence-based assessment measures for OCD meaningfully enhances a provider's ability to select the appropriate measure to detect and/or monitor the treatment of this disorder.
When describing the psychometric properties of the measures included in this review, the following criteria were used to benchmark categorizations of reliability and validity.3,4 Psychometric evaluation of reliability was based on internal consistency, interrater reliability, and test-retest reliability. For internal consistency, α values ≥0.90 were considered excellent, 0.80–0.89 were considered good, 0.70–0.79 were considered fair, and <0.70 were considered poor. Excellent interrater reliability was considered to be an intraclass correlation (ICC) value of 0.75–1.00. Lower ICC value ranges represented good (0.60–0.74), fair (0.40–0.59), and poor (<0.40) interrater reliability. For test-retest reliability, a correlation of ≥0.80 was considered good, with values of 0.70–0.79 and <0.70 representing acceptable and poor test-retest reliability, respectively. Psychometric evaluation of validity was based on convergent and discriminant validity. Good convergent validity was considered a correlation value of >0.50 between the rating scale and other measures of obsessive-compulsive symptoms and severity. Correlation values of 0.30–0.49 and 0.10–0.29 represented fair and poor convergent validity, respectively. Good discriminant validity was represented by correlations of 0.10–0.29 between the rating scale and measures of nonobsessive-compulsive symptoms and severity. Correlation values that exceeded this range were considered fair (0.30–0.49) and poor (>0.50) discriminant validity. Treatment sensitivity was classified by statistically significant reductions in symptoms following an evidence-based treatment.
Making an OCD Diagnosis
In order to determine if a patient meets DSM-5 diagnostic criteria for OCD, the patient must experience the presence of recurrent, unwanted, and intrusive thoughts (ie, obsessions) and/or repetitive behaviors or rituals (ie, compulsions) intended to relieve the fear, anxiety, and/or distress associated with obsessions. 5 Additionally, obsessions and compulsions must cause significant distress and impairment in social, academic, and/or family functioning. 5 While diagnostic assessments are often conducted as free-form unstructured clinical interview, there are several standardized structured or semi-structured interviews that have several advantages. Standardized interviews show psychometric superiority, higher validity, and less subjectivity and are more comprehensive compared to unstructured interviews.6-10 Also, when differential diagnoses are a concern, the administration of relevant diagnostic modules from standardized interviews can assist with diagnostic clarification. However, these interviews typically increase patient and clinician burden as they can require one to three hours to administer, depending on the diagnostic categories in question. While free-form clinical interviews are the most common method for determining an OCD diagnosis in clinical practice, standardized interviews are generally used in research. When an individual's presentation is complex and differential diagnoses are a concern, there is benefit to using standardized interviews in clinical practice as well. Most extant diagnostic interviews are derived from DSM-IV criteria, including the Anxiety Disorders Interview Schedule for DSM-IV (ADIS), Anxiety Disorders Interview Schedule for DSM-IV: Child and Parent Versions (ADIS-C/P), and Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I), although more recently, updated versions of these measures have been published to reflect changes in the DSM-V (eg, ADIS-V and SCID-V – Clinician Version).11-15 The ADIS possesses strong psychometric properties, shows excellent discrimination among anxiety disorders, and can reliably produce an OCD diagnosis.11,12,16,17 Shortcomings of the measure include limited focus on other nonanxiety disorders (eg, psychosis), which may be considered as a differential diagnosis. The SCID-I also shows good psychometric properties; however, some research has criticized the measure's ability to produce clinically meaningful information specific to OCD.13,18-21 A third structured interview, the Mini International Neuropsychiatric Interview (MINI) for DSM-IV, has also been validated in adult and youth samples, and a version revised in accordance with DSM-V is available for use with adults.22,23
Clinician-Rated Measures of OCD Symptom Severity
Yale–Brown Obsessive–Compulsive Scale
Clinician-rated measures of OCD symptom severity.
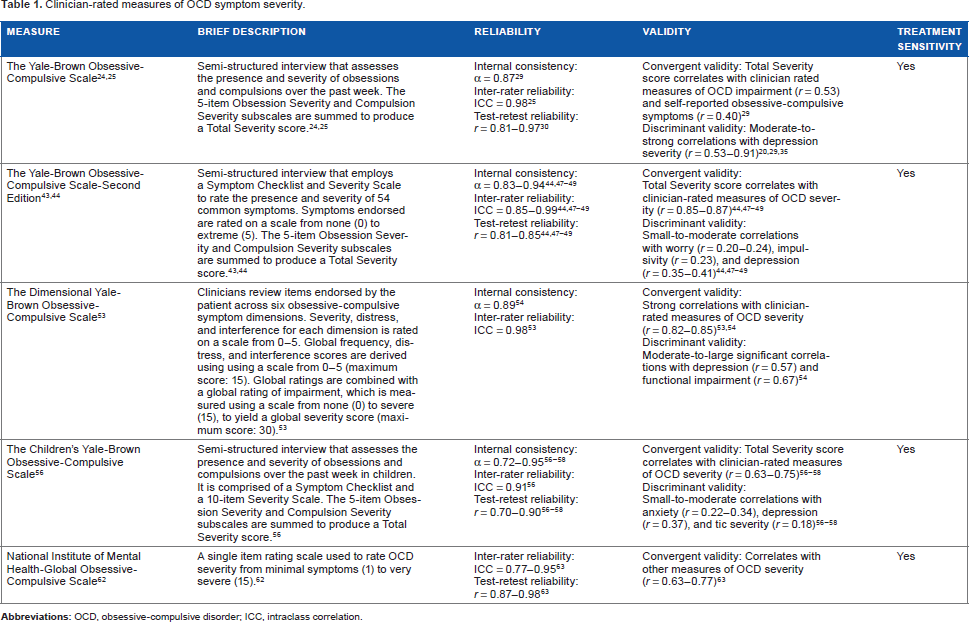
The Y-BOCS is considered the gold standard assessment tool for OCD symptom severity and possesses good psychometric properties (see Table 1).27,28 The Y-BOCS Total Severity score shows good internal consistency, excellent interrater reliability, and good test–retest reliability over a two-week interval.25,29,30 Additionally, the Y-BOCS demonstrates good to fair convergent validity with clinician-rated measures of OCD impairment and self-reported obsessive– compulsive symptoms. 29 Furthermore, the Y-BOCS Total Severity score has demonstrated treatment sensitivity to medication and evidence-based psychotherapy treatment. 31 Benchmarks for defining treatment response have been suggested to be 30%–35% reductions in Y-BOCS Total Severity score, and 40%–55% for diagnostic remission.32,33 At this level of symptom reduction, some research supports high sensitivity and specificity, with over 90% of responders and nonresponders correctly classified. 34
Despite its widespread use, at least two recognized criticisms of the Y-BOCS exist. First, some evidence suggests that the Y-BOCS has low discriminant validity with depression, as it exhibits moderate-to-strong correlations with depression severity (see Table 1).20,29,35 In part, this may be attributed to the high comorbidity between OCD and depression, with some studies suggesting that 25%-50% of individuals with OCD experience co-occurring Major Depressive Disorder (MDD).35-37 Second, the Y-BOCS has demonstrated inconsistent factor structure across several studies. While some factor analytic studies support the initial two-factor (ie, obsessions and compulsions) structure, others have found evidence for a “disturbance factor” and a “symptom severity factor,” and a three-factor structure comprised “severity of obsessions,” “severity of compulsions,” and “resistance to symptoms.”29,38-42 Despite these criticisms, the Y-BOCS is widely used across settings and continues to serve as the gold standard measure of OCD severity.
Yale–Brown Obsessive–Compulsive Scale – Second Edition
The Yale–Brown Obsessive–Compulsive Scale – Second Edition (Y-BOCS-II) was created in response to advancements in the understanding of OCD phenomenology and in an attempt to address psychometric criticisms of the Y-BOCS.43,44 The Y-BOCS-II retains the Symptom Checklist and Severity Scale, but includes several important revisions to the ordering and detail of item anchors. Benchmarks for clinically significant symptoms are consistent with those for the Y-BOCS.
First, the Symptom Checklist includes the consecutive assessment of obsessions and compulsions, as well as a more inclusive range of obsessive-compulsive symptoms with examples. Specifically, revisions have been made to: (1) better capture discomfort that some individuals experience unless rituals are completed just right, (2) provide enhanced explanations and examples of anchors, and (3) remove a priori symptom headings.45,46 Second, active avoidance behaviors that are commonly seen in adults with OCD are also included in the Symptom Checklist. The Y-BOCS-II considers active avoidance behaviors as compulsions and, in doing so, accounts for minimization of overt compulsions that may result from lack of contact with triggering stimuli. Last, ancillary items from the original Y-BOCS were removed or incorporated in the Symptom Checklist.
The Y-BOCS-II Severity Scale includes changes to the items administered (ie, an updated “obsession-free interval” item is included in lieu of the original “resistance against obsessions” items), better incorporation of behavioral avoidance, and expansion of the rating scale to range from 0 to 5 (0 = none, … 4 = very severe, 5 = extreme). In revising the range of the Severity Scale items, these adjustments provide greater severity distinction and treatment sensitivity for individuals with high OCD severity.
The Y-BOCS-II Total Severity score exhibits strong psychometric properties (see Table 1). Research suggests good to excellent internal consistency, excellent interrater reliability, and good short-term test–retest reliability.44,47-49 Additionally, it shows good convergence with other clinician-rated measures of OCD severity, and good discriminant validity from measures of worry and impulsivity. Discriminant validity from depression is fair.44,47-49 The Y-BOCS-II shows preliminary support for treatment sensitivity in a case report, with further examination in a large treatment sample needed.50,51 Sensitivity of the Y-BOCS-II has been shown to be very high (ie, 85% of OCD patients correctly identified) with comparably lower specificity (ie, 62%–70% of individuals with non-OCD diagnoses correctly identified as not having OCD). 52
The Y-BOCS-II incorporates phenomenological advances in understanding OCD and psychometrically strives to better differentiate from depression compared to the original Y-BOCS. Despite these considerable improvements, the Y-BOCS-II still has mixed support for its proposed factor structure. For example, although the authors of the Y-BOCS-II propose a two-factor structure of obsessions and compulsions, one study identified a two-factor structure comprising symptom severity and interference from symptoms.44,47,48
Dimensional Yale–Brown Obsessive–Compulsive Scale
The Dimensional Yale–Brown Obsessive–Compulsive Scale (DY-BOCS) is a clinician-rated measure of dimension-specific obsessive–compulsive symptom severity. 53 First, individuals are asked to rate the presence and severity of 88 obsessions and compulsions across the following domains: (1) harm, (2) scrupulosity, (3) symmetry/just right perception, (4) contamination, (5) hoarding, and (6) miscellaneous (eg, superstitious beliefs and behaviors). Individuals also rate overall symptom severity in the past week on a scale ranging from 0 (no symptoms) to 10 (symptoms are extremely troublesome). Based on this initial self-report and semi-structured interviewing, clinician ratings are then derived (see Table 1).
The DY-BOCS clinician-rated Global Severity scale shows good internal consistency and excellent interrater reliability (see Table 1).53,54 Convergent validity with clinician-rated measures of OCD severity is good; however, the DY-BOCS shows poor discriminant validity from depression and measures of functional impairment (see Table 1).53,54 Sensitivity and specificity of the measure have not been examined. The psychometric properties of the DY-BOCS have also been examined in a pediatric sample, showing excellent internal consistency and interrater reliability, as well as good convergent validity with clinician-rated measures of OCD severity and good to fair discriminant validity from depression, tic severity, and withdrawal. 55
Children's Yale–Brown Obsessive–Compulsive Scale
The Children's Yale–Brown Obsessive–Compulsive Scale (CY-BOCS) is a semi-structured interview that assesses the presence and severity of OCD in children and parallels the Y-BOCS format, scoring, and interpretation (see Table 1). 56 While similar to the Y-BOCS in structure, its Symptom Checklist was adapted for developmental appropriateness. Although ancillary items are included to assess insight, avoidance, indecisiveness, responsibility, pervasive slowness, and doubting, these items are not included in a rating of overall severity (see Table 1).
Like the Y-BOCS, the CY-BOCS is considered the gold standard measure for assessment of severity of pediatric OCD. The CY-BOCS Severity score has demonstrated excellent to fair internal consistency, excellent interrater reliability, and good to adequate short-term test-retest reliability (see Table 1).56-58 The CY-BOCS shows good convergent validity with clinician-rated measures of OCD severity, as well as good to fair discriminant validity from measures of anxiety, depression, and tic severity.56-58 Furthermore, the CY-BOCS Total Severity score appears to be responsive to evidence-based pharmacotherapy and psychotherapy across multiple trials.31,59 Positive treatment response corresponds with a 25% reduction in CY-BOCS total score, and a 45%-50% reduction in Total Severity score (or a Total Severity score <15) is associated with diagnostic remission. 60 Sensitivity and specificity of the measure have not been examined.
Although the CY-BOCS purports a two-factor model of obsessions and compulsions, discrepancies also exist across factor analytic studies. While there is support for the original two-factor structure (obsessions and compulsions), other studies have identified distinct two-factor models consisting of severity and disturbance.58,61 These mixed findings highlight the need to revise the CY-BOCS in order to better incorporate advancements in phenomenological understanding of the disorder and improve the factor structure.
National Institute of Mental Health-Global Obsessive–Compulsive Scale
The National Institute of Mental Health-Global Obsessive-Compulsive Scale (NIMH-GOCS) is a single-item rating to assess overall OCD severity on a scale from 1 (minimal symptoms) to 15 (very severe). 62 Severity levels are clustered into five groups that include: minimal severity (1–3), subclinical severity (4–6), clinical severity (7–9), severe clinical severity (10–12), and very severe clinical severity (13–15). The NIMH-GOCS exhibits excellent interrater reliability, good short-term test-retest reliability, and good convergent validity with other measures of OCD severity (see Table 1).30,63 The NIMH-GOCS has demonstrated treatment sensitivity in medication trials.62,64 Sensitivity and specificity of the measure have not been examined. Although findings regarding the psychometric properties of the NIMH-GOCS are encouraging, critics have noted that the measure does not adequately capture dimensional aspects of symptomatology and requires a certain level of training and expertise for reliable ratings.20,30,65 Both shortcomings limit the clinical utility of this measure for those clinicians with less OCD experience. 30
Self-Report Measures of OCD Symptom Severity
Yale–Brown Obsessive–Compulsive Scale – Self-Report
Self-report measures of OCD symptom severity.

The Y-BOCS-SR shows good to fair internal consistency and good short-term test–retest reliability in nonclinical samples (see Table 2).67-69 It shows good correspondence with clinician-rated measures of OCD severity and possesses a good ability to differentiate between individuals with OCD, anxiety disorders, and healthy controls.67-70 The Y-BOCSSR Total Severity score shows fair discriminant validity with measures of worry in a college sample, with no extant data in a clinical sample. 71 There has been no systematic evaluation of the Y-BOCS-SR's treatment sensitivity. However, it does appear to have utility as a diagnostic screening measure, with research suggesting that a score of 16 or greater may predict OCD diagnosis.67,69,70
Obsessive–Compulsive Inventory – Revised
The Obsessive–Compulsive Inventory – Revised (OCI-R) is a revision of the original Obsessive–Compulsive Inventory (OCI) developed to reduce redundancy and administration burden of the original measure.72,73 The OCI-R comprises 18 items rated on a five-point scale, from which six subscales are derived (see Table 2).
The OCI-R total score demonstrates good internal consistency and good to adequate short-term test–retest reliability (see Table 2).72,74-76 The OCI-R shows good to fair convergence with clinician-rated measures of OCD severity and fair to poor discriminant validity from depression, anxiety, and worry.72,74,76,77 While the OCI-R appears to be similarly reliable and valid when tested in an African-American sample, it is important to note that some research suggests that African-Americans tend to endorse significantly higher levels of symptom severity across subscales, particularly on hoarding and ordering subscales. 78 Initial evidence supports the treatment sensitivity of the OCI-R, with further replication needed. 77 Additionally, the OCI-R presents potential for use as a screening measure, with research suggesting a correspondence between a total score of 21 and an OCD diagnosis. 79
Florida Obsessive–Compulsive Inventory
The Florida Obsessive–Compulsive Inventory (FOCI) consists of a 20-item Symptom Checklist that includes 10 common obsessions and compulsions each derived from the Y-BOCS, as well as a five-item Severity Scale that captures symptom severity and impairment over the past month (ie, time occupied, distress, control, avoidance, and interference; see Table 1). 80
The FOCI Symptom Checklist and Severity scores demonstrate good internal consistency (see Table 1). Good convergent validity of the FOCI Symptom Checklist was evidenced by strong associations with self-reported obsessive-compulsive symptoms, and for the FOCI Severity score, by strong correlation with Y-BOCS Total Severity score.80,81 The measure shows fair discrimination from anxiety and fair to poor discrimination from depression.80,81 There has been no evaluation of the FOCI's test-retest reliability or research-based recommendations for diagnostic cutoff scores. Further, data on receiver operating characteristics analysis to determine diagnostic cut points have not been reported. Support does exist, however, for the measure's treatment sensitivity to CBT 81
Dimensional Obsessive-Compulsive Scale
The Dimensional Obsessive-Compulsive Scale (DOCS) is a 20-item self-report scale developed to better capture dimensional aspects of OCD severity. 74 Research supports a four-factor structure that includes: (1) germs and contamination; (2) responsibility for harm, injury, or bad luck; (3) unacceptable obsessional thoughts; and (4) symmetry, completeness, and exactness.74,82 Each factor is measured across five items related to time, avoidance, distress, impairment, and resistance, with items rated on a 0–4 ordinal scale (see Table 2).
Further, the DOCS has been expanded to include a supplementary scale to assess sexual obsessions, a common symptom that is believed to be phenomenologically distinct from other subtypes of obsessions.83-85 The DOCS-Sexually Intrusive Thoughts (DOCS-SIT) scale contains five items rated on a five-point scale [none (0) to extreme/severe (4)] and items probe duration of obsessions, avoidance, distress, functional impairment, and ability to resist obsessions. 86 The supplementary scale shows good internal consistency, good test-retest reliability, fair to poor convergent validity with other DOCS dimensions, and good discriminant validity from measures of depression and negative affect. 87
The DOCS total score has excellent to good internal consistency in OCD samples; however, short-term test–retest reliability was poor (see Table 2).74,82 Meanwhile, the measure shows good convergent validity with other measures of OCD severity, and fair to poor discriminant validity from anxiety and depression.74,82 The DOCS exhibits treatment sensitivity across studies, and research findings suggest that a total score of 18–20 corresponds to an OCD diagnosis.74,82,88 Diagnostic accuracy of the DOCS is high, showing good ability to discriminate individuals with OCD from controls [area under the curve (AUC) = 0.86] and those with anxiety disorder (AUC = 0.77). 89 Subscale scores reflect common dimensions of OCD, and thus, elevated scores on a single subscale may indicate potential treatment targets. 82 These properties support the use of the DOCS as a clinically informative assessment tool (ie, can determine diagnostic status and treatment response); however, it is limited in a treatment planning context as it provides minimal detail regarding the content of an individual's specific obsessive-compulsive symptoms. 82
Several other self-report rating scales of OCD severity exist, but are less commonly used in research and clinical practice. These measures include the Padua Inventory–Washington State University Revision (PI-WSUR), Vancouver Obsessional Compulsive Inventory (VOCI), Schedule of Compulsion, Obsessions, and Pathological Impulses (SCOPI), Clark-Beck Obsessive–Compulsive Inventory (CBOCI), and Obsessive– Compulsive Scale of the Symptom Checklist-90 – Revised (OCD-SCL-90-R).90-94
Youth/Parent Reports of OCD Severity
Given the phenomenological distinction in symptom presentation and comorbidity patterns between youth and adults, several measures have been specifically designed and/or adapted for use in youth populations.95-97 When assessing OCD in youth, it is critical to use developmentally appropriate tools. This promotes item comprehension, accurate reporting, and accounts for important distinctions in symptom presentation between adults and youth (eg, the phrase “need for symmetry/evening” may not be as relatable to youth as the phrase “like your books or toys lined up in a specific way”). Additionally, the inclusion of multiple informants is important among youth with OCD in order to fully capture symptom presentation and severity. For example, parents are often better reporters of visible compulsions at home, family accommodation, and/or overall impairment of youth's symptoms. Comparatively, youth are often better reporters of intrusive thoughts and symptoms occurring primarily at school or other non-home settings, unless limited by poor insight.
CY-BOCS-Child Report/Parent Report
The CY-BOCS-Child Report (CR)/Parent Report (PR) are adapted self-report versions of the CY-BOCS intended for use by youth respondents and parents. 58 The measure parallels the clinician-rated version and asks individuals to rate their own or their child's symptom severity using a multiple-choice Likert scale response format.
Parent/child measures of OCD symptom severity.

Obsessive–Compulsive Inventory – Child Version
The Obsessive–Compulsive Inventory – Child Version (OCI-CV) comprises 21 items to assess the presence and frequency of obsessive–compulsive symptoms (see Table 3). 98 It has six subscales that include: (1) doubting/checking, (2) obsessions, (3) hoarding, (4) washing, (5) ordering, and (6) neutralizing. Items are summed to produce a total score.
The OCI-CV total score shows good internal consistency and good to adequate short-term test–retest reliability (see Table 3). Convergent validity is fair to poor as evidence by significant correlations with clinician-rated measures of OCD severity. Additionally, the OCI-CV total score has fair to good discriminant validity with measures of irritability and depression.98,99 The OCI-CV has demonstrated treatment sensitivity to medication and CBT. 71 Diagnostic accuracy of the OCI-CV has not been examined.
Children's Florida Obsessive–Compulsive Inventory
The Children's Florida Obsessive–Compulsive Inventory (C-FOCI) is the parallel child-report version of the FOCI, with some minor distinctions. 100 First, there is a Symptom Checklist that includes 17 obsessions and compulsions that are rated as absent/present over the past month (see Table 3). Symptoms endorsed on the Symptom Checklist are rated on the Severity Scale, which collectively rates obsessions and compulsions on a six-point scale (0 = none to 5 = extreme) across five items related to time occupied, distress, control, avoidance, and interference (see Table 3).
The C-FOCI shows fair internal consistency across both the Symptom Checklist and Severity Scale (see Table 3). The C-FOCI Severity Scale has been shown to have moderate associations with clinician-rated OCD severity, as has the Symptom Checklist, suggesting fair convergent validity. 100 The measure's good discriminant validity is supported by weak and nonsignificant associations of the Severity Scale and Symptom Checklist with parent-reported measures of externalizing symptoms. 100 There is further support for the measure's treatment sensitivity to CBT, with significant declines relative to baseline, which is noted on both the Symptom Checklist and Severity Scale when used in treatment trials. 100 Diagnostic accuracy of the C-FOCI has not been examined.
Children's Obsessive–Compulsive Inventory – Revised
The Children's Obsessive–Compulsive Inventory – Revised (ChOCI-R) is a revised version of the original ChOCI and is appropriate for use with children and adolescents.101,102 There exist parallel self- and parent-report versions of this questionnaire. The ChOCI-R consists of two sections (obsessions and compulsions), each comprising 16 questions (see Table 3). The first section begins with 10 questions each about the presence of common obsessions and compulsions, which are rated on a three-point scale (ie, not at all = 0 to a lot = 2). The severity of endorsed obsessions and compulsions are separately rated using six questions on a scale from 0 to 4. Severity items assess time spent, impairment, distress, resistance, control, and avoidance.
Internal consistency of the ChOCI-R's child- and parent-report Total Impairment score is good (see Table 3). Both child- and parent-report Total Impairment scores exhibit good convergent validity with clinician-rated measures of OCD symptom severity. Discriminant validity from emotional disorders was fair to poor, and good from externalizing problems, with weak associations observed. Although exhibiting good to fair reliability and appropriate validity, further research is needed to examine treatment sensitivity of the ChOCI-R. While the sensitivity and specificity of the original ChOCI has been shown to be high (ie, sensitivity of 88% and specificity of 95% compared to controls), these same metrics have not been examined for the revised measure. 101
Important Related Factors
Several additional factors are important when assessing OCD. First, assessment of OCD-related functional impairment is crucial in determining if an individual meets diagnostic criteria. Moreover, impairment is considered a key treatment target, along with perceived distress, and an important component of treatment response.103,104 Second, assessing family accommodation in OCD is important as it is prevalent and associated with treatment outcome.105-107 Family accommodation is a relatively broad construct that can manifest as a family member facilitating the completion of a ritual, assisting with avoidance of a feared event, or any myriad activity carried out in response to a patient's obsessive–compulsive symptoms.108-110 High levels of family accommodation prohibit patients with OCD from fully engaging in exposure-based psychotherapy, as accommodating behaviors serve a similar function to compulsions (ie, relieving distress associated with obsessions). 111 Last, limited insight has been documented across samples of adults and youth with OCD.112-114 Limited insight into obsessive–compulsive symptoms is associated with worse clinical prognosis and attenuated treatment response to exposure-based psychotherapy.112-114
Impairment
Clinician-rated and self-report measures of adult and youth OCD impairment, family accommodation, and insight.

A more specific and commonly used measure of OCD-related impairment is the Child Obsessive–Compulsive Impact Scale – Revised (COIS-R). 120 The COIS-R is a revision of the original COIS and is available in parallel parent- and child-report versions, assessing impairment due to OCD across multiple functional domains (see Table 4). 121 The parent and child versions of the COIS-R exhibit good to excellent internal consistency and acceptable to good test–retest reliability across subscales. The parent-report version has demonstrated sensitivity as a predictor of treatment response, while the child-report version is sensitive to treatment response for both cognitive-behavior therapy and medication.122-124
Family Accommodation
Meta-analytic findings support the notion that interventions targeting family accommodation are associated with larger improvements in patient functioning, warranting the assessment and tracking of this construct. 125 There are four measures to assess for the presence and level of family accommodation in youth and adults. The Family Accommodation Scale for Obsessive–Compulsive Disorder (FAS) is a clinician-administered semi-structured interview that is similar in format to the Y-BOCS (see Table 4).108,109 This scale shows strong internal consistency and interrater reliability. 109
For adult patients with OCD, a self-report version of family accommodation also exists, called the Family Accommodation Scale – Patient Version (FAS-PV) (see Table 4). 126 The FAS-PV total score shows good internal consistency and test–retest reliability. Additionally, the FAS-PV total score exhibits fair convergent validity with other measures of family accommodation and good to fair discriminant validity with measures of anxiety, impulsivity, and depression (see Table 4). 126
Similarly, there is also the option for the adult patient's family member to complete accommodation ratings through completion of the Family Accommodation Scale – Self-Report (FAS-SR) (see Table 4). 127 The FAS-SR total score shows excellent internal consistency, but test–retest reliability has not been examined. Additionally, the FAS-SR shows good convergent validity with clinician-rated family accommodation and fair convergent validity with measures of global functioning and relative distress.
Meanwhile, for youth, there exists the Family Accommodation Scale – Parent Report (FAS-PR) (see Table 4).128,129 The FAS-PR total score demonstrates excellent internal consistency, fair convergent validity with other measures of OCD symptom severity and impairment, and good discriminant validity from measures of trauma-related symptom severity. 128 Additionally, the FAS-PR has been shown to be sensitive to treatment.124,130
Insight
A certain level of insight is inherent in making an OCD diagnosis in adults. OCD is believed to be ego dystonic, meaning that an individual is able to acknowledge that his/her thoughts and behaviors are excessive and absurd, despite the individual's continued engagement in them. 5 Research suggests, however, that not all adults with OCD are able to identify their obsessions and compulsive behaviors as irrational, which can result in poor treatment outcomes.131-133 In children, insight is not required to make a diagnosis, however, youth with poor insight similarly tend to experience worse treatment response. 134 Moreover, lack of insight can make it particularly difficult for both adult and youth patients to accurately report the extent of their symptoms and associated impairment.
Insight of adult patients can be assessed using the Brown Assessment of Beliefs Scale (BABS), a semi-structured clinician-administered rating scale (see Table 4). 135 The BABS total score exhibits good internal consistency, excellent interrater reliability, and good test-retest reliability. Additionally, the measure shows good convergent validity with other measures of delusional thinking and unawareness of mental disorders, as well as good to fair discriminant validity from symptom severity scales (see Table 4). 135
Additionally, the Y-BOCS and Y-BOCS-II each contain one item assessing insight. In youth with OCD, insight can be measured using one item from the CY-BOCS, which assesses insight on a five-point scale based on clinical judgment (0 = excellent insight, 1 = good insight, 2 = mild insight, 3 = poor insight, and 4 = completely lacks insight).
Discussion
This paper reviewed common evidence-based assessment tools in the service of assisting clinicians in developing an evidence-based assessment that addresses their specific goals. In line with the pragmatic framework, the following recommendations have been tailored to assessment goal and setting.
Screening Assessment
Brief self-reports are ideal tools to preliminarily identify symptoms and quantify severity in a time-limited setting. Self-report measures are cost effective, require minimal training to administer and interpret, and have the advantage of removing potential interviewer bias. 136 However, the items can be difficult for some patients to understand and may be better suited for adult patient populations. Accordingly, the OCI-R is a brief self-report measure that possesses reliability, validity, and diagnostic sensitivity, with a total score of 21 corresponding to an OCD diagnosis. Similarly, the DOCS is another brief measure that captures dimensional aspects of OCD and possesses excellent psychometric properties including diagnostic sensitivity, with a total score of 18–20 corresponding to an OCD diagnosis. While there has been no evaluation of diagnostic sensitivity for any youth self-report measure, the OCI-CV and C-FOCI may serve as acceptable screening tools to identify symptoms in youth.
Differential Diagnosis Assessment
Structured and/or semi-structured interviews can assist in determining an OCD diagnosis, especially when significant comorbidity is present. Thus, a clinician may select a developmentally appropriate diagnostic interview to rule out differential comorbid conditions. Additionally, this interview can be supplemented with clinician-rated and self-report scales with strong discriminant validity. The Y-BOCS-II/CY-BOCS shows good discriminant validity from worry and impulsivity, and the FOCI/C-FOCI shows fair discriminant validity from anxiety. As many of the OCD measures do not discriminate well from depression, it may be worthwhile to supplement the use of these OCD rating scales with a well-validated measure of depression severity (eg, Beck Depression Inventory-II for adults, or Child Depression Inventory-II for youth.137-139
Initial Assessment
During an initial assessment, the use of psychometrically valid clinician-rated measures for quantifying symptom severity is recommended. Clinician ratings integrate reports from multiple informants (ie, patient and collaterals), synthesize clinician observations and judgments, and are particularly helpful when assessing individuals with limited insight. 134 Clinician judgment also plays an important role considering recent changes in OCD diagnostic criteria put forth in the DSM-5. Although hoarding disorder is recognized as a distinct psychiatric disorder in the DSM-5, 25%–30% of individuals with OCD report compulsive hoarding and many well-validated assessment measures still probe for such symptoms.140-142 When an individual scores high primarily on hoarding symptoms/severity, it should be taken into consideration in the overall clinical picture, particularly since such symptoms are associated with worse treatment outcome.143-146 Clinicians may wish to also consider exploring a hoarding disorder diagnosis.
The Y-BOCS/Y-BOCS-II/CY-BOCS represent the gold standard in clinician-administered assessment tools for OCD severity. When conducting an evaluation, it is also important to integrate measures of the patient's impairment, level of family accommodation, and insight. For adults, the SDS is a brief measure that captures global impairment. While the clinician-administered FAS is preferred, the FAS-PV and/or FAS-SR are also acceptable measures. In terms of insight, the BABS is a relatively brief clinician-administered measure capable of determining a patient's insight. Meanwhile for youth, the COIS-R is a psychometrically valid measure that captures OCD-specific impairment. Additionally, it can be administered with the FAS-PR to capture family accommodation, with insight being rated using the single item on the CY-BOCS. As each of these factors can contribute to inflated or diminished quantifications of symptom severity, they should be accounted for by the clinician in case conceptualization.
Treatment Monitoring
Use of outcome monitoring and feedback is a recommended practice throughout the field of behavioral health.147-149 Such strategies have been shown to enhance clinical decision-making, as well as to improve a clinician's ability to detect worsening of symptoms and optimize treatment.150-154 Further, relaying treatment progress to a client in a standardized way can result in statistically and clinically meaningful changes in treatment outcome and engagement.155,156 When selecting tools for this purpose, it is important to prioritize symptom severity and impairment measures that have established treatment sensitivity and also evaluate factors that can attenuate treatment outcomes (eg, accommodation and insight). While the Y-BOCS/Y-BOCS-II/CY-BOCS have demonstrated treatment sensitivity across multiple studies and are preferred, they can be time consuming to regularly readminister to monitor therapeutic response. Thus, self-report measures like the FOCI and DOCS, which have demonstrated treatment sensitivity, are recommended. Even though the treatment sensitivity of the SDS has yet to be evaluated with OCD patients, it is also recommended here, given the importance of tracking functional changes over treatment. As family accommodation and poor insight can impede evidence-based treatments for OCD, these factors should be monitored regularly to ensure that they are not contributing to a patient's diminished therapeutic response. Thus for adults, the FAS-PV (and/or FAS-SR) and BABS are recommended. Meanwhile for youth, the OCI-CV and C-FOCI, along with the COIS-R, should be used to assess symptom severity and function impairment, respectively. Additionally, the FAS-PR and insight item from the CY-BOCS would be appropriate to monitor family accommodation and insight among youth.
Conclusion
When designing an assessment battery, the clinician should develop the most parsimonious assessment battery to minimize deterioration of patient responses. Time burden certainly can interfere with the feasibility of implementing an assessment battery in a clinical setting, and thus, researchers are urged to continue to develop brief, psychometrically sound measures. Concurrently, when reviewing data gathered from the assessment, a clinician should apply judgment in interpreting the data from multiple measures and weighing information across informants. Indeed, clinicians may consider the influence of parental psychopathology on reporting accuracy of child symptoms, as evidence suggest an association between parental psychopathology and greater reported severity of their child's symptoms compared to youth report. 157
In summary, an evidence-based assessment is the cornerstone of evidence-based treatment. This paper reviewed commonly used OCD measures to enhance clinicians' abilities to evaluate, differentiate, and monitor OCD symptom severity and impairment in youth and adults. Findings highlighted several psychometrically validated clinician-rated, patient-rated, parent-rated, and child-rated measures to assess OCD symptom severity and impairment (see Appendix A for information on how to access and/or request assessment tools reviewed). Based on individualized assessment goals and empirical support, this paper provided recommendations to complete an evidence-based assessment in youth and adults with OCD.
Disclaimer
The views expressed within this article represent those of the authors, were not influenced by any funding source, and are not intended to represent the position of NIMH or other funding sources.
Author Contributions
Wrote the first draft of the manuscript: AMR, JFM. Contributed to the writing of the manuscript: AMR, JFM, RLB, JP. Agree with manuscript results and conclusions: AMR, JFM, RLB, JP. Jointly developed the structure and arguments for the paper: AMR, JFM, RLB, JP. Made critical revisions and approved final version: AMR, JFM, RLB, JP. All authors reviewed and approved of the final manuscript.
Footnotes
Appendix A
To obtain the Y-BOCS, Y-BOCS-II, or FOCI/C-FOCI for use in clinical practice, please visit the following website for further details of terms and agreements: http://www.mountsinai.org/patient-care/service-areas/psychiatry/areas-of-care/obsessive-compulsive-disorder/rating-scales The CY-BOCS can be accessed through the following link: https://iocdf.org/wp-content/uploads/2016/04/05-CYBOCS-complete.pdf The DOCS can be accessed at no cost for clinical or research use through the following link: https://www.unc.edu/~jonabram/DOCS_download.html
Note: Readers interested in specific measures not listed above should contact the authors to request permission to obtain the measure.