
Abstract
In recent years, much progress has been made in pharmacotherapy for pediatric obsessive-compulsive disorder (OCD) and chronic tic disorders (CTDs). What were previously considered relatively intractable conditions now have an array of efficacious medicinal (and psychosocial) interventions available at clinicians' disposal, including selective serotonin reuptake inhibitors, atypical antipsychotics, and alpha-2 agonists. The purpose of this review is to discuss the evidence base for pharmacotherapy with pediatric OCD and CTDs with regard to efficacy, tolerability, and safety, and to put this evidence in the context of clinical management in integrated behavioral healthcare. While there is no single panacea for these disorders, there are a variety of medications that provide considerable relief for children with these disabling conditions.
Introduction
Obsessive-compulsive disorder (OCD) and chronic tic disorders (CTDs) can be highly impairing conditions which affect a wide range of youth. Multiple prevalence estimates for children and adolescents indicate that approximately 1%-2% of children experience OCD, 0.5%-1.0% experience Tourette Disorder, 1.0%-2.0% experience chronic tic disorders and approximately 5% experience transient tic disorders.1–7 Obsessive-compulsive disorder is characterized by unwanted intrusive cognitions that persist against the patient's wishes (obsessions) followed by repetitive behaviors intended to reduce associated distress (compulsions), which can be variably expressed.8–10 The content of obsessions often includes perceived contamination, uncertainty about completing an action (eg, checking locks), taboo thoughts (ie, sexual, religious, aggressive), and symmetry and ordering obsessions. Common compulsions include excessive hand washing, repetitive touching of objects, covert rituals (eg, counting, praying), reassurance seeking, unnecessary checking to ensure tasks have been completed, and ordering of objects in a certain configuration until they are perceived as “in order”. Tic disorders are characterized by both simple and complex tics, which are often manifest themselves through motor actions (eg, eye-blinking, shoulder shrugging, or detailed facial gestures) and verbal expressions (eg, groaning, cursing in public despite no intention of doing so). Tic disorders encompass chronic tic disorder (CTD), transient tic disorder (TTD), and Tourette Disorder (TD); CTDs (motor or verbal) are often grouped with TD in treatment trials and in conceptualization of pathology, whereas transient tic disorder has received less focus in clinical research. Thus, this review will address CTD and TD under the umbrella of CTDs. Obsessive-compulsive disorder and CTDs share similarities in phenotypes and neurobiology and are commonly comorbid: a modest amount of children with a principal diagnosis of OCD experience comorbid tics (20%-40%), while a higher percentage of youth with tics experience comorbid OCD (20%-60%).11–17 Comorbid tics are more frequent in younger OCD patients, and both disorder classes are more prevalent in younger boys. 18
Obsessive-compulsive disorder and CTDs interfere with the child's functioning in the school, interpersonal, emotional, and home domains.19–28 In clinical samples, over half of patients with both conditions have been observed to experience functional difficulty due to symptoms of both conditions,21, 24 with many patients having two or more problem areas in functioning. This is particularly problematic given that these conditions can occur during critical periods of social and academic development for youth, where interference from these conditions can lead to missing out on critical experiences which may affect optimal functioning in adulthood (eg, reduced access to social and academic opportunities can lead to difficulty in vocational and social functioning as adults due reduced experiences of age appropriate norms). For example, a child with OCD may have compulsions getting in the way of completing school assignments, or a child with vocal tics may have difficulty practicing reading aloud before the class or speaking to the teacher, and children with both conditions may experience distraction due to obsessions or premonitory urges that can interfere with concentration inside and outside of the classroom.
Neurobiological research of OCD has focused on the orbitofrontal cortex (along with the amygdala) in a fear learning model. Although its etiology is multidetermined, OCD has a genetic component, with increased risk of familial transmissionand some observed genetic loci of interest that merit further investigation. 29 36 Additionally, alterations in glutamatergic functioning may also be associated with OCD. 37 Other research foci in the development of OCD haveimplicated fear learning, 38 operant theory, 39 cognitive theory, 40 and sensitivity to negative affect. 41
Tic disorders are associated with dysfunction of the prefrontal cortex and the basal ganglia along with the limbic system.42, 43 Androgens have been implicated in the childhood development of OCD and CTDs, with empirical support provided by the elevated morbidity rate of both conditions in early youth as well as the study of androgen roles in CTDs. Tic disorders also have a genetic basis, with increased risk observed in family members of probands who experience tics.44, 45 Research on genetic inheritance for both conditions indicate polygenetic influences with some overlap. 46 Environmental risks for OCD/CTDs have also been identified such as perinatal difficulties, 47 traumatic experiences,48, 49 and immune related risks.7, 50-54
A variety of orally administered pharmacotherapies have demonstrated efficacy for youth with OCD and CTDs, each with specific benefits and risks. The purpose of this review is to delineate medication options based on clinical research, with randomized clinical trial (RCT) evidence being weighted most highly followed by open trial evidence, with case reports and other uncontrolled research holding less influence. Controlled evidence is particularly pertinent for tic disorders, as tic severity may fluctuate over relatively brief periods of time.55–57 An appropriate control group is necessary to separate medication effect from a naturalistic course. Emphasis is placed on the efficacy, safety, tolerability, and relative place in evidence based support of these agents. Empirical work was included if the predominant focus of the research was on children; exceptions were made only in the case of lack of pediatric research for a particular agent, and such research with an adult focus has been specifically identified. While there is little evidence to indicate that OCD and CTDs present with substantial differences between children and adults that affect treatment decision making, the evidence base for pharmacotherapy is more robust for adults. The majority of medications indicated for children have also been shown efficacious with adults, and any substantial discrepancies are explicitly noted. Psychopharmacological research for OCD and CTDs is first addressed separately for each respective condition, with subsequent focus on issues in the clinical management of each condition both individually as well as in the context of comorbidity. While cognitive behavioral therapy (CBT) has also been established as efficacious for pediatric OCD and habit reversal training has strong support for treating childhood CTDs,58, 59 the focus of this review is on pharmacotherapy, and behavioral therapies are discussed only in the context of available treatment options in deciding on medication selection.
Pharmacotherapy Options for the Treatment of Pediatric OCD
Selective reuptake inhibitor (SRI) medications have received the majority of research with pediatric OCD, which encompass the selective serotonin reuptake inhibitors (SSRIs) and a specific tricyclic antidepressant (clomipramine), and over 1,000 patients are now available for comparison in meta-analysis. Meta-analysis of RCTs have indicated that these medications have a significant effect relative to placebo, with overall effect size estimates ranging from 0.46-0.48, and with clomipramine showing a significant advantage over SSRIs in efficacy relative to placebo.60, 61 However, head to head comparisons between clomipramine and SSRIs in a single trial are unavailable, and variables in study design and subject selection can influence effect sizes. Additionally, other factors (such as tolerability) have implications for treatment selection.
Evidence for the use of SRIs in pediatric OCD has been most conclusively demonstrated through RCTs,62– [72] which have demonstrated efficacy for clomipramine, sertraline, fluoxetine, fluvoxamine and paroxetine (with pooled RCT effect sizes for each medication observed to be 0.85, 0.47, 0.51, 0.31, and 0.44, respectively).61 With regard to prescriptive use for children, the United States Food and Drug Administration (FDA) has provided approval for pediatric OCD treatment for clomipramine (ages 10 and above), sertraline (ges 6 and above), fluoxetine (ages 7 and above), and fluvoxamine (ages 8 and above). For each of these medications, dosing titration using the lowest recommended dose with incremental increases every 2-4 weeks based on efficacy and tolerability is recommended. Frequent visits at treatment initiation are also recommended, followed by less frequent monitoring after the medication regimen is stabilized.73
Selective Serotonin Reuptake Inhibitors (SSRIs)
Among FDA approved SSRIs for pediatric OCD, no significant efficacy differences have been observed,60, 61 and no direct comparisons have been made in the context of a single trial. Thus, choice of agent usage is relegated to preferred half-life, observed patient response, and idiographic tolerability of an individual agent, as the SSRIs do differ from one another in pharmacodynamics and drug interactions. In pediatric OCD trials, more commonly reported side effects of SSRIs include abdominal discomfort, decreased appetite, sleep interference in the form of either insomnia or somnolence, and fatigue.67, 68, 74, 75 While these side effects are not commonly prohibitive, significant patient dropout (22%) attributable to side effects has been observed in pediatric OCD trials. 61
The FDA Black Box warning for suicidality for SSRIs has addressed concern regarding the administration of SSRI medications,76, 77 which was based on a compilation analysis of data from RCTs in children with depression and anxiety disorders as well as on lay testimony of perceived risks. The risk for suicidal behaviors are theorized to occur in the context of behavioral activation, 78 a phenomenon which can involve agitation, hostility, restlessness, impulsivity emotional lability, and insomnia. These symptoms are most often seen 1-9 days after a dose change,78, 79 where younger children may be at higher risk from activation syndrome (with particular focus placed on mood and irritability).77, 80 When considering SSRI suicide risk by diagnosis, Bridge et al found no statistically significant increase in risk of suicidal thinking or behavior when considering pediatric OCD SSRI trials, 81 where they found an increased risk difference between SSRIs and placebo to be 0.5 and a number needed to harm of 200. Nevertheless, while such risk may have been higher in trials for depression relative to those for OCD, 81 providers must carefully monitor for increased suicidal ideation when administering SSRIs to children with OCD, especially considering the high comorbidity rate with depression,82–[84] which sometimes may go undetected given the difficulties in diagnosing pediatric internalizing disorders. 85 Managing activation can be accomplished by titrating and adjusting doses slowly, using the minimum therapeutic dose, and/or changing to a different medication. 75 Additionally, practice parameters recommend the use of CBT alone in mild and moderate severity cases, and together with a SSRI in more severe cases. 72 The combination approach should be considered given its efficacy and tolerability with the additional benefit of reduced suicidal symptoms reported in those receiving CBT + SSRI versus those receiving only SSRI treatment. 86
Clomipramine
Clomipramine was the first antidepressant to demonstrate efficacy in RCTs for pediatric OCD and is FDA approved in treating youth with OCD ages 10 and older.67, 68, 71 It has demonstrated relatively stronger effects in reducing obsessive-compulsive symptoms than the SSRIs, with an estimated effect size of 0.85 relative to placebo. 61 Clomipramine is a tricyclic antidepressant which exerts effects on serotonin and norepinephrine, which may partially account for its increased efficacy relative to the selective agents. 60 When using clomipramine, a baseline electrocardiogram (EKG) is indicated to observe for cardiac arrhythmia, and further EKG monitoring along with blood level monitoring of medication levels is indicated. Other side effects associated with clomipramine include dry mouth, somnolence, dizziness, fatigue, tremor, weight gain, and constipation.67, 68 Thus, while clomipramine has the strongest demonstrated efficacy among medications for pediatric OCD, it is often not indicated as a first-line agent due to its side effects, with particular concern given to its relationship with cardiac arrhythmia.60, 87, 88
Other Agents
Atypical antipsychotics have drawn the majority of attention among other agents in treatment for OCD, with particular attention given to their role in augmenting non-or partial-response to SRIs. Some data support this practice among adults; one recent meta-analysis suggests such use to be considered after 12 weeks of incomplete response to two adequate trials of SRI therapy. 89 However, despite its frequent use in youth, no methodologically rigorous data exist regarding antipsychotic augmentation of SRI therapy in youth with OCD beyond case reports.90, 91 Additionally, there are concerning metabolic and cardiac effects associated with antipsychotic use among youth. 92 Given the lack of RCT data and the risks of associated adverse effects, this option should only be considered after failure of appropriate CBT (of sufficient duration by a professional with expertise) and when symptoms are severely impairing functioning. Further evidence beyond uncontrolled reports is required to justify its use in youngsters with OCD. 93
A new direction in augmenting agents involves the glutamate modulators memantine and riluzole, which have had open trial support for treatment resistant OCD in youth,94–[96] with promising results. While preliminary, these medications provide an alternative to the traditional serotonin hypothesis in pharmacotherapy for pediatric OCD. Other glutamate modulators such as n-acetylcysteine and glycine have been theorized to be of pharmaceutical use, but no evidence currently exists to support their efficacy in pediatric OCD. 97
Pharmacotherapy Options for the Treatment of Pediatric Chronic Tic Disorders
The two major classes of medication that have been indicated as efficacious with pediatric chronic tic disorders are dopamine antagonists (typical and atypical), and alpha-2 agonists. While no meta-analytic estimates exist with regard to the efficacy of these agents, the effect sizes of antipsychotics relative to placebo are larger than those for alpha-2 agonists.98–103 Given the unique pharmacodynamic and pharmacokinetic characteristics of these medications, treatment choice is guided by weighing risks of adverse effect profile versus expectancy of treatment response.
Typical Antipsychotics
Typical antipsychotics were the first medications to display efficacy in controlled research for pediatric tic disorders, and thus have the broadest evidence base. The only medication with FDA approval for pediatric CTDs is pimozide (ages 12 and older). Haloperidol has a long history in the treatment of CTDs, with evidence stretching back 50 years. 104 While RCTs have demonstrated the efficacy of haloperidol in adults, 105 controlled evidence in youth is lacking; one crossover trial failed to find efficacy relative to placebo on the primary outcome measure, 106 though secondary outcome measures of global functioning detected overall improvement. Side effects that are frequently reported include extrapyramidal symptoms, sedation/drowsiness, weight gain, and increased prolactin secretion. Dosage reduction can be used to manage these side effects. Side effects from typical antipsychotics that can be serious include tardive dyskinesia and neuroleptic malignant syndrome. For CTDs, much lower doses are used than those used for psychotic disorders. For this reason and perhaps because of neurobiological differences, those with CTDs appear to have low risk for tardive dyskinesia. Estimates of the risk of tardive dyskinesia in children and adolescents treated for TD range from 1%-4.8%. 107 110 However, the risk of such effects increases with greater treatment duration and dosage, may persist after treatment discontinuation.111, 112
Pimozide, which is a less powerful antagonist of norepinephrine than haloperidol, has been employed in treatment for pediatric CTDs. Its efficacy has been established in RCTs,106, 113 with fewer adverse effects than haloperidol. However, it still presents with a substantial side effect profile including weight gain, akathisia, acute dystonia, QTc prolongation, tardive dyskinesia, and extrapyramidal effects. 114 Given its QTc effects, electrocardiograms at baseline, during titration, and at regular intervals throughout treatment are indicated. Additionally, interactions with antidepressant medications (which are commonly employed with OCD, such as fluvoxamine) have been observed, which presents substantial concern when working with comorbid conditions.
Fluphenazine, which has antagonistic properties for both D1 and D2 receptors, is better tolerated than haloperidol with regard to sedation and extrapyramidal effects while showing similar efficacy to haloperidol in adults.115, 116 However, controlled data in youth are lacking. Despite its relatively more desirable side effect profile, fluphenazine still presents the risks of traditional neuroleptic adverse effects including akathisia, tardive dyskinesia, and extrapyramidal effects.
Atypical Antipsychotics (Second Generation Antipsychotics)
The more recently introduced atypical antipsychotics have now garnered a substantial evidence base with regard to efficacy for pediatric CTDs. The major advantage of atypical antipsychotics is the reduced risk of tardive dyskinesia and extrapyramidal symptoms associated with classic neuroleptics. However, there are concerns about the safety and tolerability of these medications, especially with regard to increased levels of prolactin (with the exceptions of aripiprazole, quetiapine, and clozapine), sedation, and metabolic effects which can lead to elevated glucose levels, increased appetite, and weight gain. 117
The medication with the most research evidence in treatment for CTDs is risperidone, with efficacy demonstrated through four RCTs (effect sizes = 0.55-10).98, 118–120 However, risperidone has been associated with weight gain, increased prolactin levels, and sedation/fatigue as common side effects. 121 Nevertheless, the tolerability of risperidone has been considered preferable to that of traditional neuroleptics such as haloperidol. 103
Ziprasidone has 5HT-2 and D2 antagonistic properties along with norepinephrine and 5HT reuptake inhibition. It has RCT evidence to demonstrate efficacy relative to placebo (effect size = 0.76), 100 but merits EKG monitoring due to effects on QTc.92, 122, 123 Additionally, mild sedation has been observed. 100 Thus, while it has been demonstrated as efficacious, particular concern with regard to its effect on cardiac conduction raises caution when considering its use. Additionally, while mild sedation has been observed. 100 It is perhaps the atypical antipsychotic with the lowest weight gain profile.
Olanzapine has displayed efficacy in children with CTDs in several open trials124–126 and one small crossover trial. 127 However, it has increased risk from weight gain and metabolic effects relative to other atypical antipsychotics.121, 124, 128 Thus, given its other associated side effects such as sedation and increased prolactin levels, consideration for its use in CTDs should be made in the context of other available medicinal and behavioral treatment options.
Aripiprazole is a D2 regulator (partial agonist/antagonist), addressing hyperdopaminergic conditons in the limbic system and hypodopaminergic condition in the frontal and prefrontal cortices. 129 Multiple open trials have indicated improvement in CTD symptoms,130–133 but controlled evidence in children is currently lacking, although RCTs are underway. Sedation, nausea, headache, agitation, and insomnia have been observed as side effects; some weight gain has been observed, but to a lesser degree than other comparable agents.121, 134
Quetiapine has empirical support from one open label trial, 135 but lacks RCT evidence to support its use. It is a weaker D2 antagonist than comparable medications, and thus its theoretical efficacy for CTDs is questioned. Abdominal discomfort, gastrointestinal upset, somnolence, and weight gain have been observed as common side effects.
Given the observed side effects of atypical antipsychotics, careful observation of adverse effects is recommended. With regard to metabolic effects, the American Diabetes Association has published monitoring guidelines for these agents. 136 While these criteria have not been empirically validated, they provide a starting point in evaluating metabolic side effects with patients. Correll 92 has recommended detailed monitoring schedules that include testing for glucose, lipids, and liver function at three months after treatment initiation and then every six months thereafter, and to evaluate for sedation and weight gain at each visit. Additionally, symptoms of elevated prolactin can include menstrual interruption in females and breast tenderness in males and females, and merit further inquiry upon observation. Proactive management of such effects is recommended including adjusting dosing, changing medications, and monitoring of lifestyle habits (eg, appropriate diet and exercise).
Alpha-2 Agonists
The alpha-2 agonists clonidine and guanfacine have demonstrated efficacy in treating pediatric CTDs. While observed effect sizes in treating CTDs have been lower than those for antipsychotics, the major benefits of the alpha-2 agonists relative to antipsychotics is their reduced side effect profile (which does not include metabolic interference or extrapyramidal symptoms) and their efficacy for comorbid ADHD. 137
Clonidine has demonstrated efficacy in RCTs for CTDs (effect sizes = 0.26-0.57),101, 118, 138 with fewer side effects than neuroleptic and atypical antipsychotic medication. Common side effects reported with clonidine use include sedation, irritability, headaches, and dry mouth. However, given its short half-life, withdrawal symptoms such as temporary increases in blood pressure and heart rate have been reported.139, 140 Thus, blood pressure and pulse should be monitored at baseline and during titration, with some recommendations for baseline and follow up ECGs. 141
Guanfacine is more highly selective for the alpha-2-adrenergic receptors, which is hypothesized to be the reason for its improved side effect profile relative to clonidine (with particular regard to sedation). It also has a longer half-life than clonidine, reducing the risk of withdrawal effects and permitting for more convenient dosing (which can be limited to twice per day). Efficacy of treatment for CTDs has been demonstrated for guanfacine through RCTs (effect sizes = 0.67-0.84), with one including comorbid ADHD. 102 Although one study did not detect improvement over placebo, 142 it was limited by a small sample size, short duration, and a floor effect due to mild baseline tic severity.
Other Agents
The efficacy of the anticonvulsant topiramate was recently supported through an RCT by Jankovic et al. (ES = 1.01), 99 and has further support from retrospective chart reviews. 143 Like the alpha-2 agonists, topiramate has the advantage of no risk of extrapyramidal side effects or weight gain relative to typical or atypical antipsychotics. Common observed side effects include somnolence, weight loss, and cognitive slowing. The anticonvulsant levetiracetam has shown open-label evidence for improving tics;144, 145 however, two small randomized crossover trials did not detect a tic-reducing effect.101, 146 Commonly reported side effects include somnolence, headache, dizziness, and asthenia. Significant agitation has also been associated with levetiracetam use and suicidal ideation has been observed in 1% of patients,147, 148 which merits close monitoring for psychiatric adverse events during administration. 149
Mecamylamine is a nicotine receptor agonist which has conflicting research support, where a retrospective case report series indicated some efficacy, 150 but it did not demonstrate superiority to placebo in a well-designed RCT. 151 Nicotine (via gum or transdermal patch) as an augmentation strategy with haloperidol has been investigated, with open trial evidence showing minor effects for CTDs, 152 but an RCT did not support its efficacy. 151 Baclofen is an agent that interacts with GABA to inhibit the release of various neurotransmitters (including glutamate), which has support in a large open label trial, 153 and a small RCT indicated significant difference from placebo on the CGI-Severity, 154 but only near-significance on the Yale Global Tic Severity Scale (YGTSS).155, 156 For very localized tics, botulinum toxin has been studied, with some evidence from open trials.157, 158 In an RCT, botulinum toxin reduced number of tics per minute as recorded on videotape, but patients did not report perceived benefit. 159 Additionally, although botulinum toxin may display some effectiveness in addressing a very localized tic (eg, facial grimacing), it does not address the underlying psychopathology as tics may simply be reassigned to different body parts, 159 and thus it should not be considered a common treatment for a wide variety of tics.
Other agents that interact with the dopaminergic system include metoclopramide, tetrabenazene, tiapride, sulpriride, and pergolide. Metaclopromide is a D2 antagonist which has traditionally been used for gastroesophageal reflux disease and as an anti-nausea agent, with side effects that can include sedation, increased appetite, and increased levels of prolactin, along with a risk of tardive dyskinesia and extrapyramidal symptoms. 160 Though it has a limited evidence base for CTDs, in a small RCT it demonstrated efficacy compared to placebo (effect size = 0.95). 161 Tetrabenazine is a dopamine agonist that intercedes in dopamine reuptake, which has case series and open trial support.162–164 Side effects include sedation, depression, nausea, insomnia, akathisia, and parkinsonism, and insomnia. Tiapride is a benzamide that has some support through an RCT to improve tics compared to placebo, 165 with hyperprolactinemia, somnolence, and weight gain as side effects of note. Sulpiride is similar to tiapride, and has some support through retrospective studies to improve tics in adults. 166 The most common side effects reported were sedation and depression, although tardive dyskinesia was reported in a case report. 167 Both sulpiride and tiapride are available in Europe but not in the United States. Pergolide interferes with dopamine release and has been investigated for use in Parkinson's disease. While efficacy compared to placebo has been reported,168, 169 pergolide has been associated with cardiac valve pathology in treatment for Parkinson's disease and has been withdrawn from the United States market.170, 171
Choosing among Pharmacotherapy Options for Pediatric OCD and CTDs
Clinical Management of Pediatric Obsessive Compulsive Disorder
Controlled Evidence for Pharmacotherapy Options in the Treatment of Pediatric OCD.

Clinical Management of Pediatric Chronic Tic Disorders
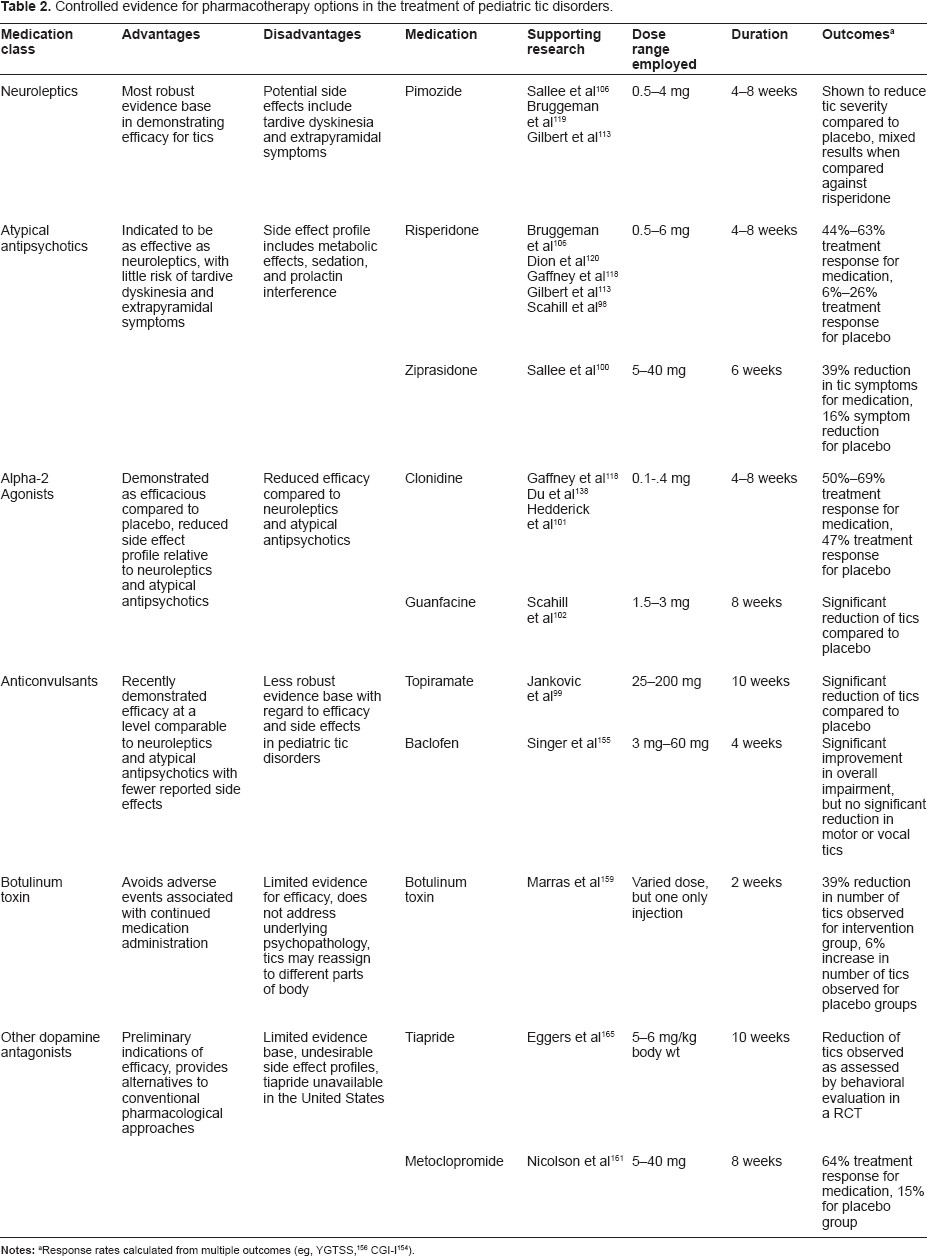
Controlled Evidence for Pharmacotherapy Options in the Treatment of Pediatric Tic Disorders.
For youth with CTDs, tics generally run a waxing and waning course, with many youth experiencing remission of tics by age 18.55, 89 The majority of remaining youth will continue to exhibit tics, albeit with reduced severity compared to those experienced in childhood and adolescence, and a minority will continue to experience sustained tic symptoms. Given these observations, the option of no treatment or behavioral therapy should be considered in the context of presenting severity versus the side effects of the medication employed, with particular consideration given to habit reversal training (HRT). The central components of HRT involve creating awareness of premonitory urges in context and then implementing incompatible competing behaviors, such as contracting the muscle opposite of the tic. For example, a child may learn to identify that he has an eye-blinking tic when sitting in class, become able to identify it each time it happens, and then invoke a response where he consciously uses his eye muscles to hold his eyes open when feeling such an urge. Habit reversal training was the central component of the multi-site RCT for the Comprehensive Intervention for Tics (CBIT), along with functional analysis and relaxation training. In this large (N = 126), multi-site RCT, the CBIT intervention displayed an effect size of 0.68 relative to the control arm, with a reduction in tic severity comparable to contemporary medicinal interventions. 58 Additionally, at 6 month follow up 87% of treatment responders contacted experienced continued benefit from the CBIT intervention. However, most patients were on medications during the trial and a head to head comparison of therapy to medication, similar to the Pediatric OCD Treatment Study (POTS) 72 is needed. While CBIT is a promising intervention, it may not be appropriate for younger children and those with limited insight/motivation, and outcomes may be affected by certain comorbidities that would impact self-monitoring (eg, ADHD).
Clinical Management of Common Comorbid Conditions
Comorbid conditions in children present complexity in the context of therapeutic management for clinicians. Unfortunately, comorbidity is the rule rather than the exception in the clinical presentation of children with OCD and CTDs, and may be associated with attenuated response and remission rates.180–183 It has also been observed that with CTDs, more impairment may be caused by the comorbid conditions than the tics themselves. 180 In the context of pharmacotherapy, the presence of CTDs in children may substantially attenuate response to SSRIs for children with OCD, where one study found a 75% response rate for children with OCD only in comparison to a 53% rate for those children with OCD who also present with tics, 62 and another found non-significance relative to placebo in post-hoc analyses for sertraline monotherapy in children with OCD and comorbid tics. 182 Moreover, this comorbidity has been associated with a greater OCD relapse rate following paroxetine treatment. 62 Further complicating matters is the fact that OCD is often comorbid with CTDs and depression,82–84 and CTDs are frequently comorbid with OCD and ADHD. 184 Given the high comorbidity rate found between OCD and CTDs (as well as with other conditions), clinicians often are faced with multiple decisions in treatment planning for these comorbid conditions. In general, the state of current psychopharmacological practice when presented with comorbidity for children with OCD and tics is to use the agent that is appropriate for each condition if pharmacotherapy is needed, while considering the possible negative or positive effects that the agent may have on comorbid conditions.179, 185, 186
The situation is simplified in pharmacotherapy for OCD, where SSRIs can affect both OCD and depression/anxiety, and while they have not been observed to help with CTDs, they have not been associated with worsening of comorbid tics. On the other hand, with regard to comorbid ADHD and CTDs, while there is some evidence that stimulants may exacerbate tics and anxiety in children with CTDs,187, 188 a meta-analysis by Bloch et al indicates that this effect may be dependent on the specific agent and dosing, 189 and one multisite RCT found roughly equal tic increases when using methylphenidate, clonidine, or placebo. 190 Although the issue of stimulants and CTDs presents with some contrasting evidence, using clonidine or guanfacine to address comorbid CTDs and ADHD simultaneously is a consideration when choosing among pharmacotherapy options for these conditions. Additionally, there is some evidence that risperidone and aripiprazole may have positive effects on anxiety symptoms,185, 186, 191 which is hypothesized to be a consequence of their action on 5HT receptors, and is a further consideration when treating comorbid CTDs and OCD.
Conclusion
The goal of this review has been to discuss the current state of research on pharmacotherapy for pediatric OCD and CTDs, to provide an overview for clinical practice, and to demarcate current limitations in the literature to identify future research directions. While gains have been made in developing effective and safe/tolerable pharmacotherapy options for pediatric OCD and CTDs, much progress remains to be made. While pharmacotherapy is associated with generally positive treatment response, no current medication consistently achieves the more stringent criterion of symptom remission. Even with CBT for pediatric OCD (the most efficacious intervention reviewed), a significant proportion of children remain symptomatic following treatment.72, 192 With regard to pediatric OCD, moving beyond the serotonin hypothesis into other domains such as ascertaining the role of glutamate may provide fertile ground for efficacy gains. For CTDs, identifying and evaluating safe and effective alternatives to neuroleptics and atypical antipsychotics are indicated, with the use of alpha-2 agonists and topiramate as a starting point. Across disorders, identifying moderators and mediators of response and side effects is of critical importance to facilitate treatment individualization. Identifying which populations respond better to a certain medicine or which patient groups are less likely to experience side effects from a particular agent could assist in improved idiographic care.
With regard to contemporary agents, more comparative work between medications in a randomized fashion could allow for direct comparisons of efficacy and adverse event rates. Many medications have demonstrated efficacy relative to placebo, and for a new medication to be of incremental value, it must be more efficacious or have better safety/tolerability than currently available agents, which is a hypothesis that may be best tested in a RCT with medications compared against one another. The evidence base is robust enough to move beyond the “nil hypothesis” 193 that pharmacotherapy is better than no intervention at all, and to make further progress, the benchmark in many cases may be efficacious contemporary agents.
One further consideration is that that these medications are not prescribed in a vacuum, but are administered in the context of integrated behavioral healthcare. Careful weighing of the benefits and risks relative to the degree of impairment is of foremost importance when employing medications is needed, with particular regard given to available behavioral interventions. Moreover, given side effects of some agents, establishing a therapeutic relationship is of substantial consequence in promoting adherence to the intervention and comfort in reporting adverse events, and can also serve to empower a patient's decision making in treatment and provide a source of support to the patient in the face of functional interference. Such a relationship, often defined as the “therapeutic alliance”, has been indicated for further exploration with pediatric psychopharmacology, 194 and explains a portion of outcome variance in pharmacotherapy for adult depression as well as a variety of pediatric psychotherapies. It is also important to consider the family role with these conditions,195, 196 with a particular focus on how the family may interact with the child's symptom presentation. For example, a family may overly accommodate a child's OCD symptoms or be overly critical of a child's CTD symptoms, which can serve to worsen symptoms. In the presence of heterogeneity among family reactions to the pathology, clinicians can foster a supportive but disciplined approach towards implementing the chosen intervention.
Compared to only 25 years ago, a marked increase in pharmacotherapy interventions have become available for children with OCD and CTDs to intervene for these debilitating conditions. This has provided an array of efficacious interventions for youth with markedly reduced side effect profiles, although much progress still remains to be made. Given this expansion of treatment options, the major decisions in clinical pharmacotherapy come down to a balance of efficacy and adverse effects in the context of functional impairment and available psychosocial interventions. Managing these variables in the context of the evidence base for each approach will foster improved child outcomes.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and not under consideration by any other publication and has not been published elsewhere. The authors confirm that they have permission to reproduce any copyrighted material.
Mr. De Nadai and Mr. McGuire report no financial relationships with commercial interests. Dr. Storch has received grant funding from the All Children's Hospital Research Foundation, the Centers for Disease Control and Prevention, the International OCD Foundation, Janssen Pharmaceuticals, the National Alliance for Research on Schizophrenia and Affective Disorders, the National Institute of Mental Health, the National Institute of Child Health and Human Development, the Australian Rotary Health Research Fund, Transcept Pharmaceuticals, Biovail Technologies, and the Tourette Syndrome Association. Dr. Storch has received consultancy fees from Prophase Inc. and Otsuka Pharmaceuticals, receives textbook honoraria from Lawrence Erlbaum and Springer publishers, has been an educational consultant for Rogers Memorial Hospital, and receives research support from the All Children's Hospital Guild Endowed Chair and the University of South Florida. Dr. Lewin has received research support from the International OCD Foundation, the National Alliance for Research on Schizophrenia and Affective Disorders, and Otsuka Pharmaceuticals. Dr. Lewin has received consultancy fees from Prophase Inc. and Otsuka Pharmaceuticals. Dr. Murphy has received research support from the National Institute of Mental Health, the National Institute of Child Health and Human Development, Forest Laboratories, Janssen Pharmaceuticals, Endo, the International OCD Foundation, Transcept Pharmaceuticals, Biovail Technologies, the Tourette Syndrome Association, the All Children's Hospital Research Foundation, the Centers for Disease Control, and the National Alliance for Research on Schizophrenia and Affective Disorders. Dr. Murphy is on the Medical Advisory Board for Tourette Syndrome Association. She receives textbook honorarium from Lawrence Erlbaum.