
Abstract
Both obturator and sciatic nerve block in combination with femoral nerve block (FNB) have been suggested to be useful in relieving pain after total knee arthroplasty (TKA), compared with FNB alone. We compared their efficacy in this retrospective study. For six consecutive months, patients undergoing unilateral TKA under general anesthesia with continuous FNB plus obturator nerve block (n = 8) or continuous FNB plus sciatic nerve block (n = 8) were investigated. Knee pain was assessed using visual analogue scale (VAS) on the day of surgery and on postoperative days one to three. In addition, we also investigated intraoperative and postoperative morphine consumption. VAS scores and total morphine consumption were not different between the two groups, although patients in the FNB plus sciatic nerve block group were administered less morphine during surgery. Sciatic nerve block with continuous FNB may be superior to obturator nerve block with continuous FNB for analgesia during surgery for TKA.
Introduction
Patients undergoing total knee arthroplasty (TKA) often experience severe postoperative pain. Effective postoperative pain control leads to earlier ambulation and physiotherapy,1–3 which can reduce the length of in-hospital stay and lower the risk of postoperative complications, such as thromboembolic events.
Femoral nerve block (FNB), intravenous opioid patient controlled analgesia (PCA) and epidural analgesia are common methods for pain relief following TKA. Among them, femoral nerve block has increased in popularity because of its superior pain control during mobilization, opioid sparing effects, and consistency with anticoagulatory therapy. 4 Furthermore FNB is an easy technique to master and has a low risk of complications. The emergence of ultrasound guidance for peripheral nerve block has also increased this trend.
Although FNB is a good way to reduce pain after TKA, FNB does not provide complete analgesia. Two kinds of peripheral nerve block have been suggested to improve analgesia following TKA in combination with FNB; obturator nerve block5,6 and sciatic nerve block.7–9 However, no investigations have directly compared these two methods of analgesia. Thus, the purpose of this retrospective study was to determine the analgesic efficacy of FNB plus obturator nerve block and FNB plus sciatic nerve block after TKA.
Methods
For six consecutive months, from September 2010 to February 2011, patients undergoing unilateral TKA under general anesthesia with continuous FNB plus obturator nerve block (CFNB + ONB group) or continuous FNB plus sciatic nerve block (CFNB + SNB group) were investigated based upon their medical records and charts. We obtained the comprehensive agreement of patients about deriving clinical data for a retrospective study. Patients who underwent TKA using other methods of anesthesia and analgesia were excluded. In order to compare the postoperative opioid consumption for each method of analgesia, patients who did not have the intravenous opioid PCA system were also excluded.
Patients undergoing TKA were intubated after the induction of general anesthesia with propofol (1–2 mg/kg), remifentanil (0.1–0.5 mcg/kg/min) and rocuronium (0.6–1 mg/kg). General anesthesia was maintained with sevoflurane (1%–1.5%) and remifentanil (0.1–0.5 mcg/kg/min). FNB and either obturator nerve block or sciatic nerve block were then performed in the supine position. The skin around the inguinal area was prepared and draped in a sterile fashion. FNB, obturator nerve block and sciatic nerve block were all guided by ultrasound (Vivid s6, GE Healthcare, Buckinghamshire, UK) without the use of nerve stimulation. A linear array 5- to 13-MHz ultrasound transducer was used for the FNB and obturator nerve block, and a convex array 1.5- to 4.5-MHz ultrasound transducer was used for the anterior approach of the sciatic nerve block. Both ultrasound transducers were enclosed in sterile sleeves and sterile gel was applied. Patients in the CFNB + ONB group received continuous FNB and obturator nerve block. Patients in the CFNB + SNB group received continuous FNB and sciatic nerve block.
FNB was performed with the transducer parallel to the inguinal crease to obtain a SAX (short-axis) view of the femoral nerve. An 18-gauge, 5-cm-long Tuohy needle (Contiplex Tuohy, B. Brown Melsungen AG, Germany) was inserted in-plane through the iliaca fascia to the surface of the femoral nerve. Twenty-25 mL of 0.5% ropivacaine was injected to create a perineural fluid space. A 20-gauge catheter was then inserted perpendicular to the femoral nerve 3–5 cm beyond the tip of the Tuohy needle. After completion of the surgery, the catheter was connected to an elastomeric infusion pump (Coopdech Balloonjector 300, Daiken Medical Corporation, Tokyo, Japan). The pump was filled with 0.2% ropivacaine, and its flow rate was 5 mL/hr (continuous FNB).
Obturator nerve block was performed using ultrasound guidance and injection of 8–10 mL of 0.75% ropivacaine. The transducer was placed in the inguinal crease to identify the femoral artery and vein. The transducer was then moved medially along the inguinal crease. After identification of the fascial planes of the pectineus and adductor muscles along the inguinal crease, half of the volume of ropivacaine was injected between the pectineus and adductor brevis muscles via the 20-gauge 8 cm-long Tuohy needle, and the other half was injected between the adductor brevis and adductor magnus muscles.
In performing sciatic nerve block, patients were placed in the supine position with the hip and knee on the operated side flexed and the leg rotated externally. The ultrasound transducer was first positioned approximately 8 cm distal to the inguinal crease. A clear transverse image of the hyperechoic sciatic nerve located posterior and medial to the lesser trochanter was then scanned by adjusting the position of the transducer. A short bevel 100-mm, 22-gauge echogenic nerve block needle (Plexufix, B. Braun Melsungen AG, Germany) was inserted in-plane with the transducer from anteromedial to posterolateral of the thigh. The perineural spread of the solution was achieved with 20–25 mL of 0.3% ropivacaine.
The surgery was started after completion of the FNB and either obturator or sciatic nerve block. Approximately 1 hour before the TKA was completed, 0.4–1.2 mg/kg morphine and 50 mg flurbiprofen were administered intravenously to attenuate postoperative pain. The dose of this single shot of intravenous morphine was determined at the discretion of the anesthesiologist in charge of the patient. After surgery, patients were provided with the intravenous PCA system (i-Fusor, Debiotech, Lausanne, Switzerland) set to deliver 0.016–0.02 mg/kg morphine (0.5 mg/ml) every 10 min, as needed. After the patients were transferred to the general ward, oral loxoprofen 60 mg was administered when they required adjunctive analgesics in addition to the intravenous morphine PCA system and continuous FNB.
After surgery, patients were moved from the operation room to the transfer room, and efficacy of FNB and sciatic nerve block was examined by pinprick test (18G). The pinprick test was conducted on the anterior aspect of the thigh and the medial aspect up to the medial malleolus below the knee (femoral nerve) and the dorsal aspect of the foot (sciatic nerve). It was not determined whether or not obturator nerve block was successful in the CFNB + ONB group. Knee pain was assessed at rest using visual analogue scale (VAS) scores ranging from 0 mm (no pain) to 100 mm (worst imaginable pain), at the same time as the pinprick test. VAS scores were also recorded on postoperative days 1 to 3 by the anesthesiologist in charge of the patient at the general ward. In addition, the following data were investigated: intraoperative and postoperative morphine consumption, the incidence of postoperative nausea and vomiting (PONV), and the maximum continuous passive motion (CPM) angle of the knee on postoperative days 7.
Data are expressed as the median (interquartile range) unless otherwise indicated. Continuous variables were compared with Wilcoxon rank sum test. Categorical variables were compared with Pearson's χ2 or Fisher's exact test. A P value <0.05 was considered to be statistically significant. All analyses were performed using JMP software (SAS, Cary NC).
Results
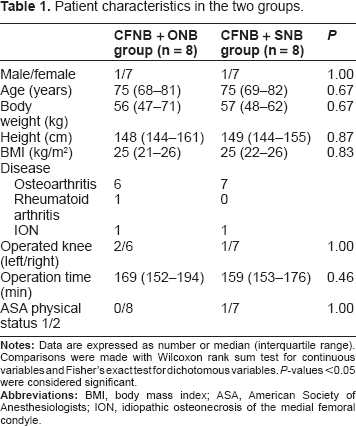
There were nine patients in the CFNB + ONB group and eleven patients in the CFNB + SNB group. Among them, one patient in the CFNB + ONB group and three patients in the CFNB + SNB group were excluded because the intravenous opioid PCA system was not used after surgery. Ultimately, eight patients in each group were included in the subsequent analyses. The baseline characteristics of patients were similar between both groups (Table 1).
Patient characteristics in the two groups.
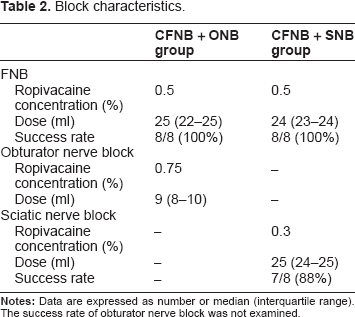
The clinical features of the peripheral nerve blocks performed in both groups are presented in Table 2. The success rate of FNB, assessed by pinprick test after surgery, was 100% in both groups. The success rate of sciatic nerve block, assessed in the same manner, was 88% in the CFNB + SNB group. Transient motor blockade of the sciatic nerve was seen in 2 patients (25%) in the CFNB + SNB group, both of which lasted at least until the next morning after surgery. No complications of peripheral nerve blocks were observed in either group.
Block characteristics.
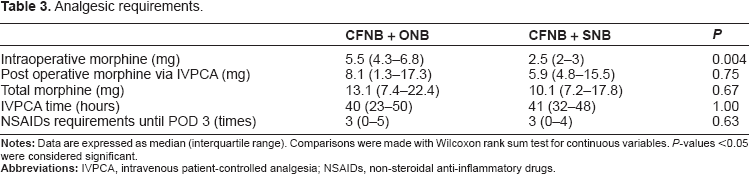
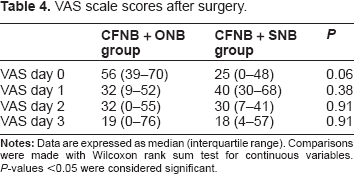
The amount of morphine administered during surgery was significantly lower in the CFNB + SNB group compared with the CFNB + ONB group (Table 3). Nevertheless, there were no significant differences in VAS scores just before transfer to the general ward; rather, patients in the CFNB + SNB group tended to suffer from less pain (Table 4). This trend disappeared by the next day and the VAS scores were similar in both groups on postoperative days one to three. Total morphine consumption was also similar in both groups. The incidence of PONV was 38% (three patients) in the CFNB + ONB group and 25% (two patients) in the CFNB + SNB group. The maximum CPM angle of the knee (median, interquartile range) on postoperative days 7 was 88 (81–98) degrees in the CFNB + ONB group and 93 (81–95) degrees in the CFNB + SNB group.
Analgesic requirements.
VAS scale scores after surgery.
Discussion
All four major nerves around the hip are associated with innervation of knee sensation: the femoral, the lateral femoral cutaneous, the obturator and the sciatic nerves. 10 The femoral nerve supplies the skin over the anterior surface of the thigh, quadriceps muscles and the knee joint. The lateral femoral cutaneous nerve supplies the anterolateral and lateral aspect up to the middle of the thigh. It also provides one branch to the patella. The obturator nerve innervates the adductor muscles and the skin over the medial aspect of the thigh. It also sends an articular branch to the knee. The sciatic nerve innervates the posterior part of the thigh and all areas below the knee joint except the medical aspect up to the medial malleolus. Since the superior analgesic efficacy of FNB after TKA has been widely recognized, the addition of another peripheral nerve block to FNB has received increasing interest for attenuating postoperative pain.
In this study we focused on the addition of obturator nerve and sciatic nerve blockade to continuous FNB. We found no differences in the VAS scores immediately after surgery with significantly smaller amount of intraoperative morphine in the CFNB + SNB group. However, although the difference was not significant, patients in the CFNB + SNB group appeared to suffer from less pain just after surgery, as assessed by VAS scores. This indicates that the sciatic nerve plays a more important role than the obturator nerve as a supplier of knee sensation. However, total morphine consumption and VAS scores were similar in both groups on postoperative days 1 to 3. In performing the sciatic nerve block, we used ropivacaine 0.3%, which was a relatively low concentration. This was because we intended to avoid motor blockade of the sciatic nerve to allow us to confirm the absence of severe sciatic nerve injury as a complication of TKA just after completion of the surgery. Thus the duration of the sciatic nerve block could be too short to make a significant difference in the total morphine consumption compared with the CFNB + ONB group.
The analgesic efficacy of sciatic nerve block after TKA is controversial. Allen et al found no analgesic difference after FNB versus FNB and single shot sciatic nerve block. 11 They used 30 mL of 0.25% bupivacaine with 1:400,000 epinephrine for sciatic nerve block. Conversely, others have reported the benefit of adding continuous sciatic nerve block to continuous FNB after TKA.7–9,12 Dang et al 9 found lower VAS scores and decreased morphine consumption in the continuous femoral and sciatic nerve block group. They argued that sciatic-related pain would last 36 hours after surgery, thus the effect of a single injection of sciatic nerve block would rarely be persistent throughout this period. These studies suggest the superior effects of continuous injection as a method of sciatic nerve block. We agree that continuous sciatic nerve block should be considered at least when a low concentration of local anesthetic is used for sciatic nerve block in addition to FNB for analgesia after TKA.
Obturator nerve block has been reported to have an opioid sparing effect after TKA when added to single shot FNB 5 or single shot FNB plus sciatic nerve block. 6 In our study, the addition of obturator nerve block to continuous FNB is likely to have a minor effect compared with sciatic nerve block. Obturator nerve block may be effective but is less effective compared with sciatic nerve block for analgesia after TKA. However, obturator nerve block could be worthwhile especially in the case of patients who are at high risk for sciatic nerve injury as a complication of TKA and thus, are reluctant to undergo sciatic nerve block. Sciatic nerve injury occurs with an incidence of 0.3%–1.8% after TKA. 13 It occurs primarily with correction of combined fixed valgus and flexion deformities, which are common in patients with rheumatoid arthritis. Some people have cautioned that sciatic nerve block could increase the risk of sciatic nerve injury after TKA or delay its diagnosis. 14
Winnie et al 15 described femoral ‘3-in-1 nerve block’ for blockade of the femoral, obturator, and lateral femoral cutaneous nerve. However, several studies have demonstrated that this approach does not consistently block the obturator nerve.16–18 The lack of appropriate assessment of the obturator nerve block by motor testing might contribute to the misconception of femoral ‘3-in-1 nerve block’, as there is no cutaneous contribution of the obturator nerve in many cases.19,20 In our study, we did not examine whether or not obturator nerve block was successful, since sensory testing assessed by the expected cutaneous distribution is potentially confusing and motor testing is fairly complicated. If motor testing is needed as an accurate method to assess the consequence of obturator nerve block, the strength of adduction must be measured with a mercury sphygmomanomemeter, as described by Lang et al 18 Meanwhile, when evaluated by pinprick test, the success rates of FNB and the anterior approach of sciatic nerve block were 100% and 88%, respectively. Although we used only ultrasound guidance without nerve stimulation, these data were comparable with previous studies, 21 which suggests the high quality of peripheral nerve block in both groups in this study. Thus we believe that the success rate of obturator nerve block in this study was high.
The question can be asked which extent effective continuous FNB alone is. Wang et al 22 reported that total morphine consumption within 48 hours after TKA was 17.6 ± 48 mg (mean ± SD) using continuous FNB and intravenous morphine PCA system as postoperative analgesia. Their protocol of continuous FNB and intravenous morphine PCA system were similar as that in our study.
This study has some limitations. First of all, this study was designed in a retrospective manner and might have a strong selection bias. Second, we did not assess whether or not the obturator nerve block was successful, as noted above. Nevertheless, this study is worthwhile, since there has been no randomized controlled trial to directly compare these two methods of analgesia.
In conclusion, sciatic nerve block is likely to be superior to obturator nerve block when added to continuous FNB for analgesia after TKA on the day of the surgery. However, the similar VAS scores in both groups on postoperative days one to three, along with similar morphine consumption, suggest the need for continuous sciatic nerve block with continuous FNB.
Disclosure
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.