
Abstract
Purpose:
The purpose of this study is to examine the clinical effects and results of lower-extremity surgery under ultrasound-guided nerve block; time required for nerve block, anesthesia onset time, duration of anesthesia, duration of analgesia, tolerable tourniquet time, visual analog scale (VAS) satisfaction score, and anesthetic-related complications.
Methods:
A total of 3312 cases (2597 patients) from January 2010 to April 2015 were analyzed retrospectively. A senior author performed ultrasound-guided nerve block of the lateral femoral cutaneous nerve (LFCN, 630 cases), femoral nerve (FN, 2503 cases), obturator nerve (ON, 366 cases), sciatic nerve (SN, 3271 cases), or posterior femoral cutaneous nerve (PFCN, 222 cases) depending on the type of surgery. Time required for nerve block, anesthesia onset time, duration of anesthesia, duration of analgesia, tolerable tourniquet time, VAS satisfaction score, and anesthetic-related complications were analyzed.
Results:
The mean times required were 1.1 min for SN block, 2.5 min for FN/SN block (1762 cases), and 4.8 min for FN/SN/LFCN/ON block. The mean anesthesia onset time was 48 min. The mean durations of anesthesia were 4.5 h for FN dermatome and 5.6 h for SN dermatome. The mean duration of analgesia was 11.5 h. The mean tolerable tourniquet times after were 35, 51, and 84 min after SN block, FN/SN block, and FN/SN/LFCN/ON block, respectively. The mean VAS satisfaction score was 9.3. There were no anesthetic-related complications, such as infection, hematoma, paralysis, or nerve irritation.
Conclusion:
Selective block of the LFCN, FN, ON, SN, and PFCN based on the locations of lesions and type of surgery showed favorable clinical results with high efficacy. Ultrasound-guided nerve block may be a good option for anesthesia and analgesia in lower-extremity surgery.
Introduction
The use of ultrasound (US) allows safe and rapid local anesthesia by providing real-time observation of anatomical structures of the soft tissues, enabling physicians to selectively block nerves that control motor and sensory function of the lower extremities, based on the locations of lesions and type of surgery. 1,2 This is a great advantage compared to blind nerve block or neurostimulator-guided nerve block. 1,3 –11 In addition, US-guided nerve block is not associated with complications that may occur due to spinal anesthesia, such as headache, hypotension, reduced bowel movement, urinary retention, lower back pain, nausea, vomiting, and respiratory problems. 10,12 –15 Furthermore, a high success rate of anesthesia can be achieved as it allows real-time monitoring of the needle and injected anesthetics as well as anatomical structures, thus reducing the amounts of local anesthetics used. However, general concerns still remain about nerve block with regard to its efficacy and complications related with the procedure.
We hypothesized that US-guided nerve block in lower-extremity surgery would produce good clinical results with few complications. In this study, we examined the effectiveness and complications of US-guided nerve block for orthopedic surgeries on the lower extremities by analyzing various clinical outcomes of 3312 cases. In particular, we assessed the affects of blocking different combinations of the lateral femoral cutaneous nerve (LFCN), femoral nerve (FN), obturator nerve (ON), sciatic nerve (SN), and posterior femoral cutaneous nerve (PFCN). The purpose of this study is to examine the clinical effects and results of lower-extremity surgery under ultrasound-guided nerve block; time required for nerve block, anesthesia onset time, duration of anesthesia, duration of analgesia, tolerable tourniquet time, visual analog scale (VAS) satisfaction score, and anesthetic-related complications.
Methods
Patients
We retrospectively assessed 3312 cases (2597 patients) who had undergone surgeries under US-guided nerve block between January 2010 and April 2015 in one institution, Chungnam national university hospital. One senior author performed local anesthesia to selectively block one or several of the nerves; LFCN, FN, ON, SN, and PFCN; mentioned above based on the type of surgery (Table 1).
Cases of ultrasound guided nerve block.

a F = femoral nerve. b b = block. c S = sciatic nerve. d L = lateral femoral cutaneous nerve. e O = obturator nerve. f P = posterior femoral cutaneous nerve.
A total of 2041 cases (2041 patients) underwent one surgery and 1271 cases (556 patients) underwent multiple surgeries ranging from two to eight. The study was approved by our institutional review board and written informed consent was obtained from all patients preoperatively before the nerve block. We excluded the patients with mental illness such as mental retardation, psychological disorder, etc.
This study retrospectively analyzed the data of each patient with the approval of the institute’s Research Ethics Review Committee (IRB No. 2015-07-004).
Preparation of US-guided nerve block
US-guided nerve block was performed in the US room using ACCUVIX V-20 and ACCUVIX XG US devices (Medison, Seoul, Korea) with a 5–13 MHz musculoskeletal US probe. Anesthesia was administered with the patient in the supine position in all cases (Figure 1).

A. Image showing the site of the ultrasound probe with the patient in the supine position for femoral nerve block. B. Image showing the patient’s position, ultrasound probe, and needle site for sciatic and posterior femoral cutaneous nerve block performed with the hip in 30°–45° flexion.
The anesthetics used were 1% lidocaine and 0.75% ropivacaine mixed at a 1:1 ratio. Preparation of nerve block was composed of 50 mL syringe and 23-gauge spinal needle, and intravenous extension line filled with the anesthetics. The mean volumes used for nerve block were 6 mL for LFCN, 16 mL for FN, 9 mL for ON, 18 mL for SN, and 6 mL for PFCN. The total of 6992 nerve blocks were conducted for the 3312 patients (Table 2).
Anesthetics dosage used for each nerve block.

a LFCN = lateral femoral cutaneous nerve. b FN = femoral nerve. c ON = obturator nerve. d SN = sciatic nerve. e PFCN = posterior femoral cutaneous nerve.
In patients who did not show contraindications for sedative administration (3179 cases, 96%), an average of 2.0 mg (range: 1.5–2.5 mg) benzodiazepine (Midazolam) was injected intramuscularly approximately 30–60 min before surgery as an anti-anxiolytics. In addition, an average of 2.4 mg (range: 2.0–3.0 mg) Midazolam was injected intravenously diluted in 100 mL normal saline for patients (1324 cases, 40%) who preferred to have more sedative effect during the surgery.
The state of the patients were monitored by measuring heart rate, oxygen saturation, and blood pressure after the nerve block in the US room, ward, and operating room by the nurse.
Clinical evaluation of US-guided nerve block
The following were evaluated. Match between type of surgery and nerve block. Time required for SN block (Sb), FN/SN block (FSb), FN/SN/LFCN block (FSLb), FN/SN/PFCN block (FSPb), FN/SN/LFCN/ON block (FSLOb). Anesthesia onset time, or the time until the patient did not feel pain upon application of pinprick stimulation to the anesthetized area. Duration of anesthesia, or the time between nerve block and when the patient started to feel pain in the pinprick test. Duration of analgesia, or the time between nerve block and when the patient started to feel pain voluntarily. Tolerable tourniquet time, or the time from application of the tourniquet until the patient felt pain due to tourniquet applications in patients who complained of tourniquet pain during surgery. The tolerable tourniquet time was measured in patients who had undergone surgery with the use of a tourniquet to the thigh after FSb and FSLOb and in patients who had undergone surgery after using an Esmarch bandage as a tourniquet to the lower leg after Sb. For patients who complained of tourniquet pain, the tourniquet was removed and the surgery was performed without it or with new application of an Esmarch bandage on the lower leg. Patient satisfaction with the anesthesia method was surveyed before discharge using a visual analog scale (VAS) (score 0–10). Preferences among general anesthesia, spinal anesthesia, and US-guided nerve block were investigated. Complications associated with anesthetics and sedatives.
An investigator not involved in any operative treatments retrospectively reviewed medical charts and interviewed time results related with the US-guided nerve block.
US-guided nerve block in the lower extremity
Before needle insertion, the skin lateral to the probe was disinfected with an alcohol swab. The in-plane approach was used for nerve block. While continuously injecting anesthetic, we made the anesthetics completely surround the nerve like ‘donut’ shape by precisely moving the tip of the spinal needle. Perineural vessels run with nerves and large vessels run adjacent to nerves such as ON, FN, and posterior tibial nerve. Therefore, to be certain that there is no vascular injury, we checked for it by pulling back the syringe at certain intervals (once per injection of every 2–4 mL) in all cases. The procedures of the US-guided 5 nerve blocks are well introduced in the youtube site (https://www.youtube.com/watch?v=yJO8k0AXZRs).
Lateral femoral cutaneous nerve block (LFCb)
The LFCN on the superficial layer of the tendon sheath of the sartorius muscle mostly crosses the anterior superior iliac spine (ASIS) from the region medial to 1–2 cm from the ASIS toward the inferolateral direction. In most cases, it can be observed only on close examination by repetitively moving the probe from the proximal to the distal direction. A long, thin, slightly arched thread-like structure extending from the proximal medial region to the distal lateral region on the superficial region of the sartorius muscular fascia can be observed. While monitoring the nerve with the probe, the needle was inserted through the skin 2–3 cm lateral from the probe and the anesthetics were injected around the nerve (Figure 2).
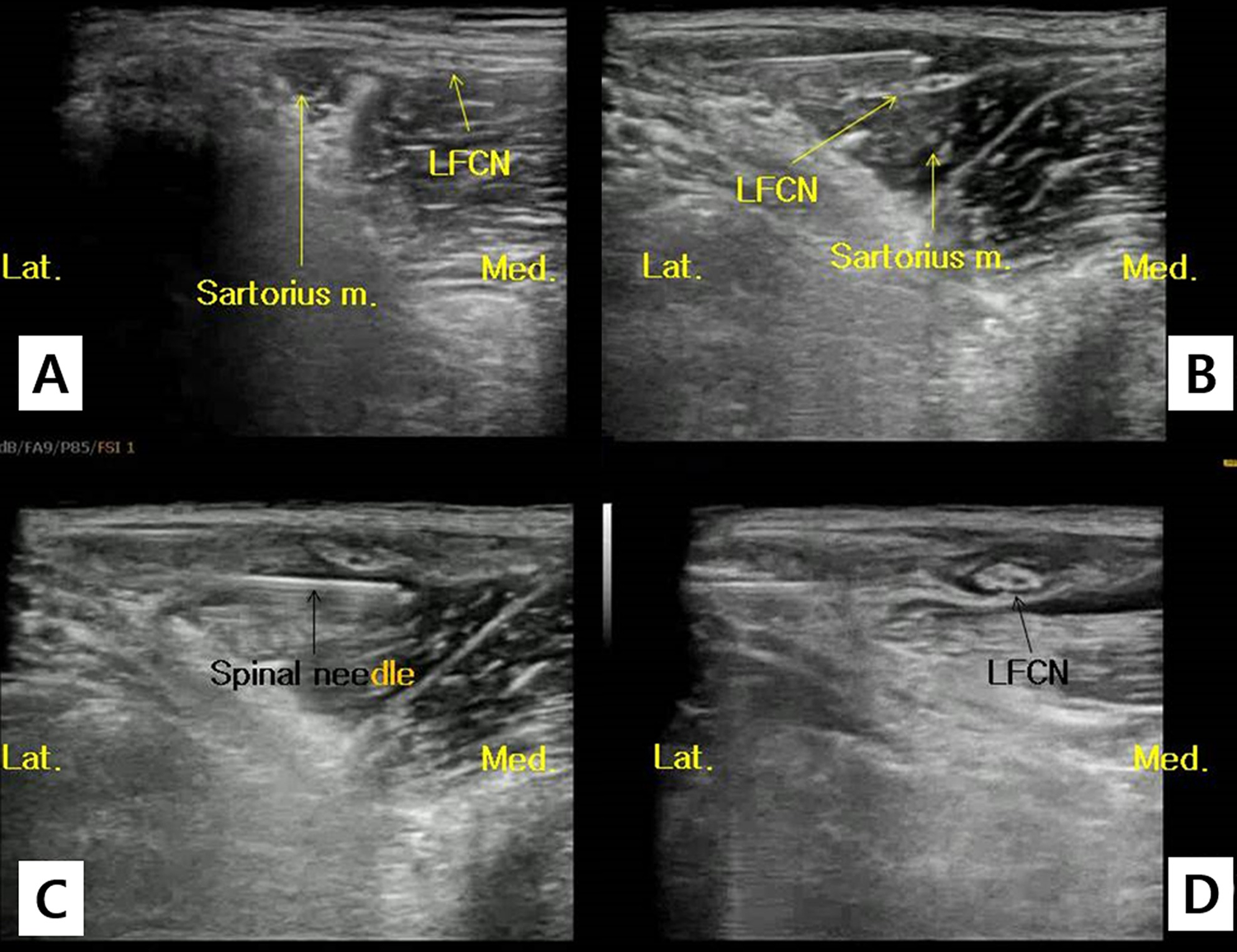
A. Ultrasound image showing the lateral femoral cutaneous nerve (LFCN) superficial to the deep fascia of the sartorius muscle. B and C. Images showing the injection of anesthetics near the LFCN under ultrasound guidance. D. The LFCN surrounded by anesthetic after nerve block.
Femoral nerve block (Fb)
Only the inguinal region on the affected side of the patient in the supine position was exposed (Figure 1A). Anatomical structures were checked by locating the US probe in the distal region of the inguinal ligament and the anterior region of the femoral triangle. The structures were checked in the order of the femoral vein, femoral artery, and FN from the medial to the lateral direction. The FN is located in the deep iliopsoas fascia and was observed as a long oval or comma-shaped structure by slightly moving the probe proximally and distally. While monitoring the nerve with the probe, the needle was inserted through the skin 2–3 cm lateral from the probe and the anesthetics were injected around the nerve (Figure 3).

A. Femoral triangle showing the femoral nerve (FN), femoral artery, and femoral vein. B. The right FN surrounded by anesthetic after nerve block.
Obturator nerve block (Ob)
A unique method was used whereby the ON was blocked by moving the need to the ON while performing Fb, called single-needle femoro-obturator nerve block (FOb). First, the anatomical structures were observed by locating the US probe parallel to the inguinal ligament while inserting the needle for Fb. Then, after performing Fb, the superior ramus and symphysis pubis were observed by moving the probe medially. The pectineus muscle was observed in the superficial region of the distal superior ramus when the probe was moved slowly to the distal region, and the adductor longus, adductor brevis, and adductor magnus muscles were observed in sequence from the medial superficial region to the deep region. As the ON is thin and located in the deep region, it is difficult to observe. Therefore, Ob was performed by identifying the obturator artery that runs together with the ON by color Doppler US and injecting the anesthetics around the artery (Figure 4). The anterior branch of the ON and obturator artery was observed in the region where the pectineus, adductor longus, and adductor brevis meet, whereas the posterior branch of the ON and obturator artery were observed in the region where the adductor brevis, adductor magnus, and pectineus meet. After finding the needle tip with the probe under conditions where Fb has already been done, the needle can reach the obturator artery and ON if it is proceeded to the inferior region and medial region of the femoral artery and vein.
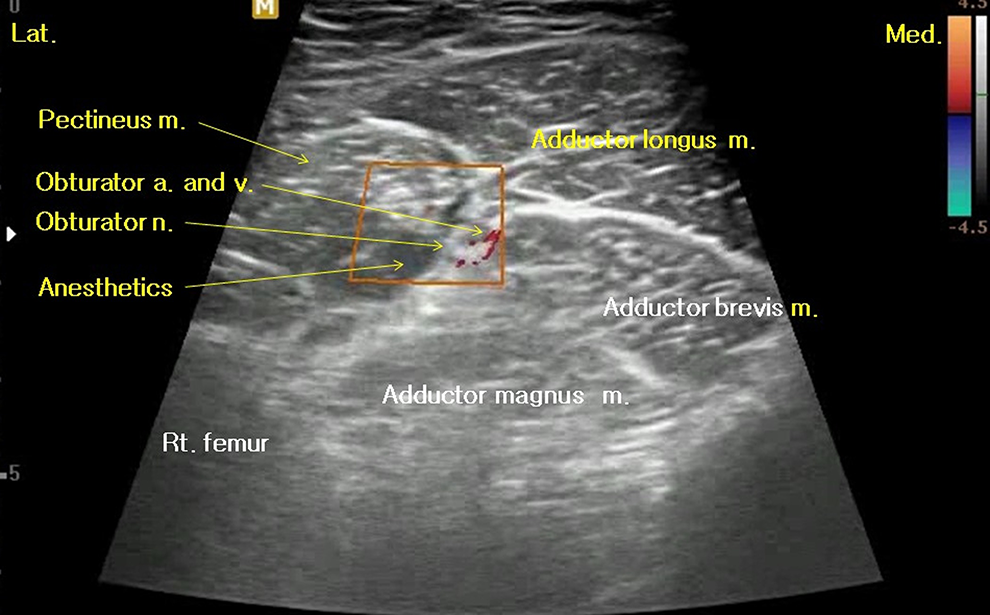
The obturator nerve (ON) and artery were surrounded by the pectineus, adductor longus, adductor brevis, and adductor magnus muscles just distal to the superior ramus of the pelvis. After identifying the obturator artery via color Doppler ultrasonography, ON block can be performed easily under ultrasound guidance.
Sciatic nerve block (Sb)
Sb was performed with the hip in 30°–45° flexion (Figure 1B). The anatomical locations of the popliteal artery, popliteal vein, tibial nerve, and peroneal nerve were checked by situating the probe at the popliteal fossa. The location for anesthetic injection was determined after observing the tibial nerve and the peroneal nerve in combination with the SN by slowly moving the probe to the proximal region of the thigh. The needle was inserted in the 20°–30° anteromedial direction to the skin at the level between the iliotibial band and the biceps femoris. We finely adjusted the direction of the needle to ensure its location in the anterior or posterior region of the epineurium of the SN (Figure 5).
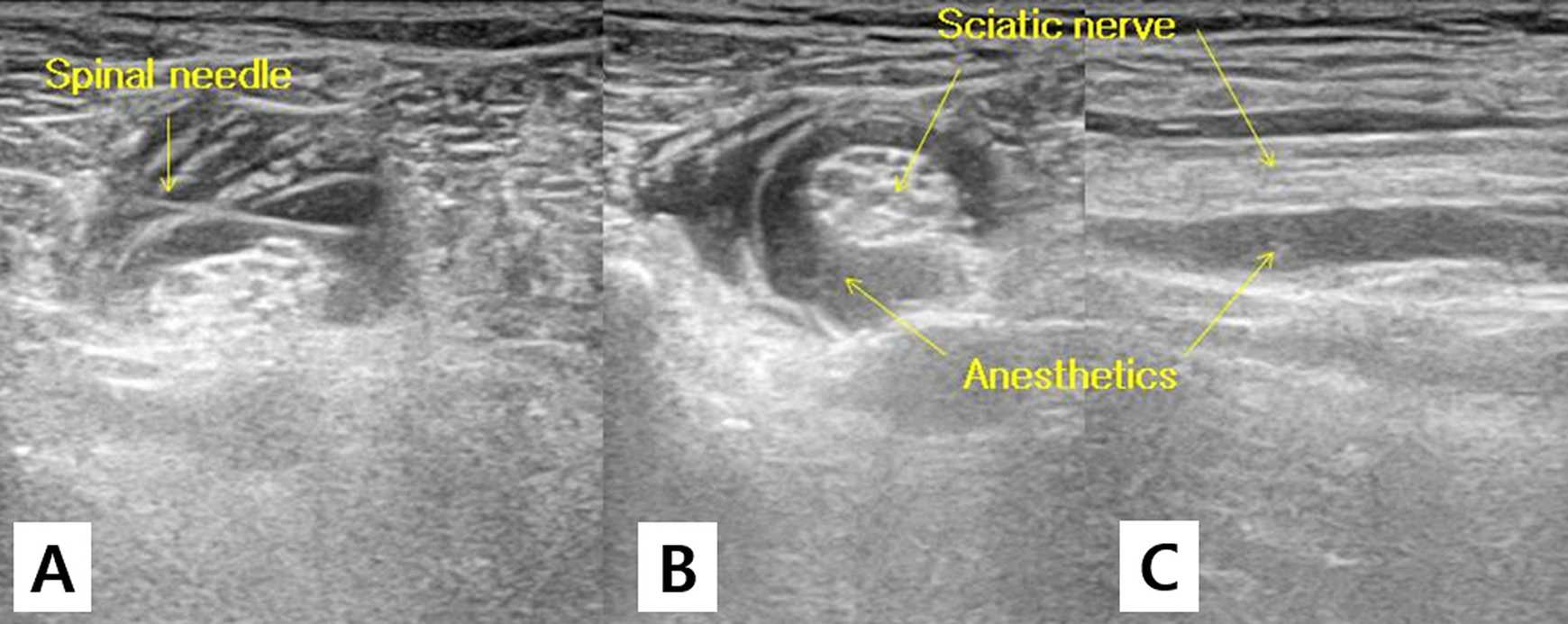
A. The anesthetic needle was advanced to the sciatic nerve (SN). B and C. The SN completely surrounded by anesthetic as seen in axial and sagittal images.
Posterior femoral cutaneous nerve block (PFCb)
Careful observation is required to detect the PFCN due to its small size. In general, it is observed at the boundary between the lateral hamstring muscle and the medial hamstring muscle. Hence, for PFCb, we first performed Sb and then pulled the needle partially back, changed its direction toward the skin of the posterior thigh, and the pushed it toward the PFCN (Figure 6).
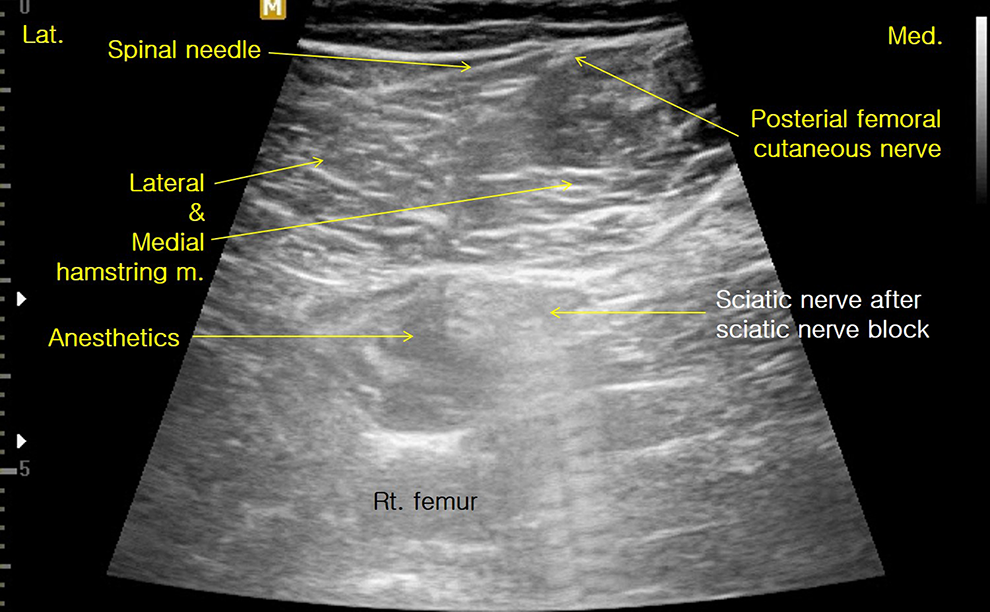
Posterior femoral cutaneous nerve (PFCN) block can be performed using single-needle approach after sciatic nerve block. PFCN always passes a superficial fascia between the medial and lateral hamstring muscle.
Results
FSb was performed in 1762 cases (53%), Sb was performed in 765 cases (23%), FSLOb was performed in 317 cases (%), FSLb was performed in 183 cases (5.5%), and FSPb was performed in 107 cases (3.2%) (Table 3). The times required for nerve block are shown in Table 4. The mean anesthesia onset time was 48 min (range: 20–100 min) for Fb and Sb. The mean duration of anesthesia was 4.5 h (range: 4–6 h) for Fb and 5.6 h (range: 5–7 h) for the Sb. The mean duration of analgesia was 11.5 h for Fb and Sb (range: 6–30 h).
Match between type of surgery and blocked nerve.

a F = femoral nerve block. b S = sciatic nerve block. c L = lateral femoral cutaneous nerve block. d O = obturator nerve block. e P = posterior femoral cutaneous nerve block.
The time required for ultrasound guided nerve block.

a F = femoral nerve. b S = sciatic nerve. c b = block. d L = lateral femoral cutaneous nerve. e O = obturator nerve.
Regarding the tolerable tourniquet time, in cases in which surgeries were conducted on the foot, ankle, or lower leg under FSb, a pneumatic tourniquet with a pressure of 250 mmHg was applied at the distal femur for an average of 51 min (range: 0–90 min). In cases in which surgeries were conducted around the knee joint and in the distal femur under FSLOb, it was applied at the mid-shaft region of the femur for an average of 74 min (range: 50–120 min). An Esmarch bandage was used on the lower leg in surgeries for the foot and ankle under Sb. The Esmarch bandage was applied for an average of 35 min (range: 0–50 min) (Table 5).
Tolerable tourniquet time.

a S = sciatic nerve. b b = block. c F = femoral nerve. d L = lateral femoral cutaneous nerve. e O = obturator nerve.
Regarding patient satisfaction, the mean VAS satisfaction score was 9.3 points (range: 5–10 points), and 3149 cases (95%) indicated that if they had to have a reoperation they would chose the same anesthetic method they had for their surgery (Table 1). All patients who had surgeries more than once (556 individuals) had reoperations under US-guided nerve block.
There were no cases of infection or hematoma at the needle insertion site, and no complications including nerve palsy or nerve stimulation associated with the use of anesthetics or spinal needles. No clinically significant side effects were observed in patients (3179 cases, 96%) who had intramuscular injection of Midazolam. However, among those who received it intravenously (1342 cases, 40%), seven (0.5%) experienced paradoxical excitation, a significant side effect of Midazolam. This disappeared within 3 min after intravenous injection of the Midazolam antagonist Flumazenil (Flunil®; Bukaung Co., Ltd., Seoul, Korea).
Discussion
The data presented here supported our hypothesis that US-guided nerve block in lower-extremity surgery can produce good clinical results with few complications.
Improvements in the accuracy and success rate of anesthesia have decreased the amounts of local anesthetics used, which has in turn made it possible to conduct numerous types of nerve block simultaneously. 1,5 –7,9,16 Among 3312 cases in the present study, there were no cases of switching to general anesthesia or spinal anesthesia due to incomplete nerve block, and significant vascular damage or nerve damage was not observed. In addition, no clinically significant side effects related with morbidity and mortality were observed.
US-guided nerve block showed several advantages in this study. It required only a short time for procedure and provided pain control after surgery for more than 10 h (average, 11.5 h, maximum > 19 h). In the case of FSb, which was the most common block performed in this study, the mean time for the procedure was 2.5 min (range: 2–6 min). We assumed that the high degree of satisfaction result might be due to the long duration of analgesia. In the authors’ other study, additional solitary injection of diluted local anesthetics for Fb or Sb under US guidance allowed extension of postoperative analgesic duration, providing more effective pain control compared to other analgesic drugs. 17,18 Also immediate preparation of nerve block and surgery is another great advantage. In the authors’ previous study, emergency external fixation with US-guided nerve block in patients with severe lower extremity trauma can be implemented in less time, regardless of the preoperative preparation, which is a requirement for general anesthesia. 19
The types of nerve block used for anesthesia in the lower extremity differ according to the location of the tourniquet, tourniquet time, and surgical site. In this study, most surgeries were performed with additional LFCb and Ob for FSb when the tourniquet time was 50 min or longer or when surgeries were performed in the knee joint and the distal femur. 20 In the previous study of our team, arthroscopic knee surgery, such as meniscal repair or meniscectomy, synovectomy, and other procedures, was safely and effectively performed under US-guided nerve block. 20 We concluded that the choice of anesthesia does not influence the recovery 6 months after knee arthroscopy, but US-guided regional nerve block is more effective than spinal anesthesia and general anesthesia for postoperative pain control without general complications after the procedure. However, FSb alone was sufficient when the tourniquet time was shorter than 50 min and surgeries were performed on the foot, ankle, and proximal tibia. The selection and indications of nerve block according to type of surgery are shown in Table 6.
Selective nerve block for lower extremity surgery.
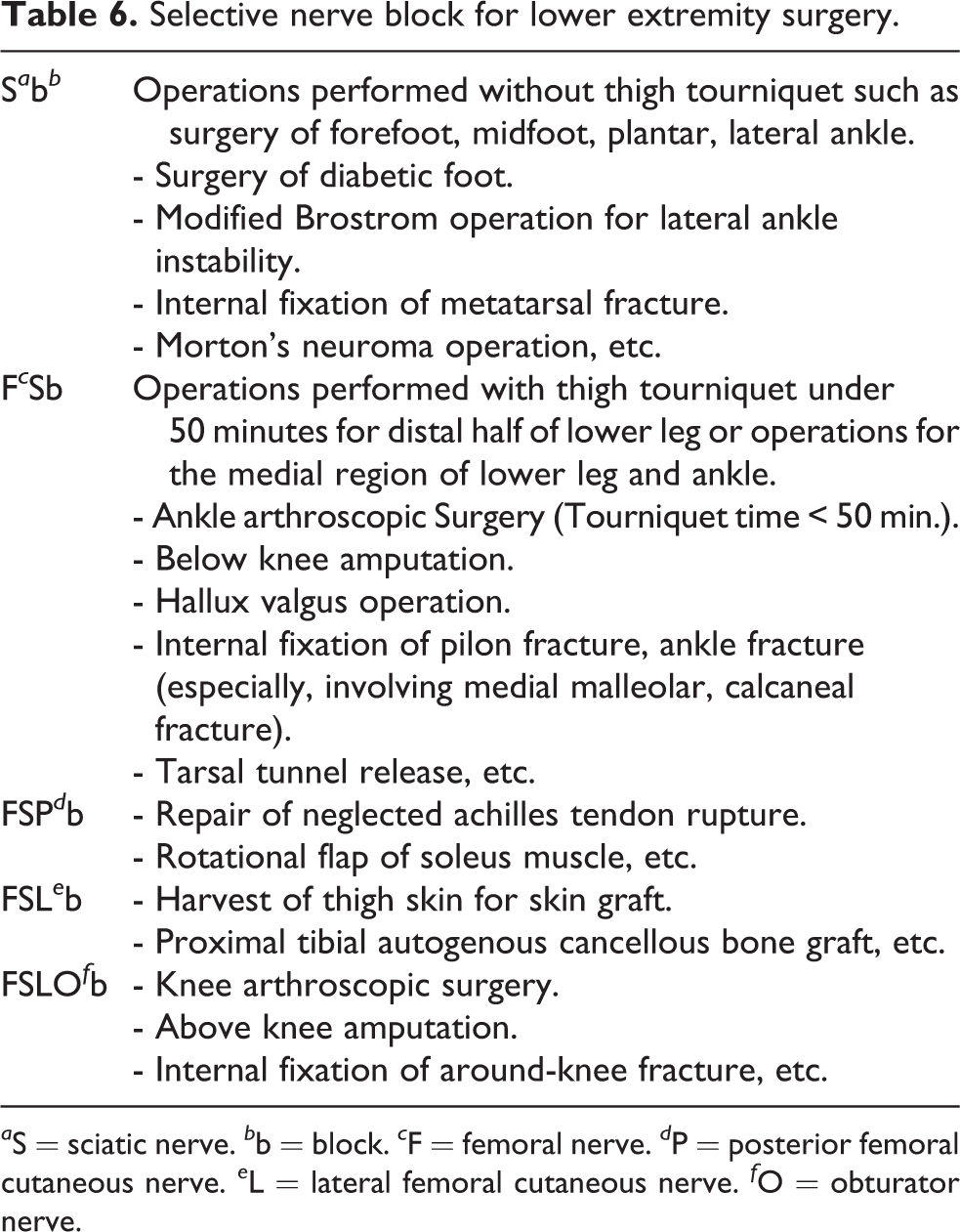
a S = sciatic nerve. b b = block. c F = femoral nerve. d P = posterior femoral cutaneous nerve. e L = lateral femoral cutaneous nerve. f O = obturator nerve.
Pearce et al. reported that coagulopathy, local infection, hematoma, peripheral neuropathy, and distorted anatomy at the site for local nerve block are contraindications for block. 21 However, we do not consider the last as contraindications, as the use of US allows direct observation of anatomical structures without causing nerve damage. We propose that neurosis, psychosis, dementia, and some types of mental retardation, which are difficult to control using sedatives, should be included as contraindications for nerve block. That is, the method of anesthesia must be chosen carefully in patients requiring deep sedation or sleep during surgery, as hyperpnea has been observed in some neurosis and psychosis patients after administration of anesthetics or sedatives. And we performed US-guided nerve block on patients taking anti-coagulants without stopping medications, there was no anesthetic-related complications such as hematoma, etc.
The limitations of our study included its retrospective nature and the short-term follow-up data. Prospective and long-term follow-up studies of US-guided nerve block for the lower extremity surgery are required. Also, only some cases of the study were compared with general anesthesia and spinal anesthesia as reported in our previous studies. 19,20 A comparison study among our regional anesthesia technique, general anesthesia, and spinal anesthesia of large group are required. Another limitation is that US-guided nerve block was performed by single proceduralist.
In summary, regional anesthesia through ultrasound-guided nerve block for the lower extremity is a safe procedure that can be performed rapidly. Selective block of the lateral femoral cutaneous nerve, femoral nerve, obturator nerve, sciatic nerve, and posterior femoral cutaneous nerve based on the locations of lesions and type of surgery showed favorable clinical results with high efficacy. Ultrasound-guided nerve block may be a good option for anesthesia and analgesia in lower-extremity surgery.
Footnotes
Authors’ note
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.