
Abstract
Purpose
Depression is frequently observed in people with diabetes. The purpose of this study is to develop a tool for individuals with diabetes and depression to communicate their comorbid conditions to health-care providers.
Method
We searched the Internet to review patient-held medical records (PHRs) of patients with diabetes and examine current levels of integration of diabetes and depression care in Japan.
Results
Eight sets of PHRs were found for people with diabetes. All PHRs included clinical follow-up of diabetes and multidisciplinary clinical pathways for diabetes care. No PHRs included depression monitoring and/or treatment. In terms of an integrated PHR for a patient comorbid with diabetes and depression, necessary components include hopes/preferences, educational information on diabetes complications and treatment, medical history, stress and coping, resources, and monitoring diabetes and depression.
Conclusion
A new PHR may be suitable for comorbid patients with diabetes and depression.
Introduction
There are bidirectional pathways between diabetes and depression,1–7 and meta-analyses of longitudinal studies show that people with diabetes are 1.3 times more likely to be depressed than people without diabetes 5 and that people with depression are 1.6 times more likely to have diabetes than people without depression. 3 Comorbid depression in patients with diabetes worsens blood glucose levels, 8 elevates initiation of dialysis,9,10 and increases use of emergency care and costs, 11 and mortality.12–15 Medication adherence rates also decrease when people with diabetes have depression. 16
Patient-held medical records (PHRs) were primarily developed as a copy of the medical record for patients to keep and take to health appointments, to help manage health-care tasks and communication, 17 and to improve the continuity and quality of care. 18 In Japan, Japan Association for Diabetes Education and Care (JADEC) developed diabetes handbook in 1982. The handbook was revised as Diabetes Communication Handbook in 2010 to enhance continuity of care between primary care physicians and diabetologists. 19 The Japanese Society of Ophthalmic Diabetology developed an eye notebook for people with diabetes to enhance communication between internal medicine and ophthalmology in 2002. 20 In 2008, the Japan government recommended that each prefecture develop PHRs for cancer, stroke, acute myocardial infarction, and diabetes as a care pathway in the community. 21 In 2013, mental disorders were added as the fifth priority diseases for Japanese national medical services.
However, PHRs for diabetes and depression are independently developed, and there is no collaboration or integration of care for the two diseases. In addition, there are no publications on PHRs for patients with mental disorders except dementia. 22 Therefore, we reviewed the current PHRs for patients with diabetes and developed a PHR for patients with comorbid diabetes and depression. The purpose of this study is to develop a tool for individuals with diabetes and depression to communicate their comorbid conditions to health-care providers.
Methods
Procedure
The study protocol was designed in collaboration with the National Hospital Organization Kyoto Medical Center (NHO-KMC), National Centre of Global Medicine (NCGM), and National Centre of Neurology and Psychiatry (NCNP). NHO-KMC, a national general hospital located in the south part of Kyoto city, has been a World Health Organization Diabetes Collaborating Center since 1988. NCGM and NCNP are government-funded national institutes with hospitals responsible for promoting the development and use of PHRs (through local government and health-care organizations) for patients with diabetes and mental disorders, respectively. The Diabetes and Metabolism Information Center in the NCGM has been providing information on diabetes care to patients and clinical staff and PHRs for diabetes to local governments and medical associations since 2008. The Diabetes and Metabolism Information Center Website provides links to local PHRs for people with diabetes (http://ncgm-dm.jp/center/hashin_ipan.html). Twelve PHRs are available through the Website.
Components of the PHRs
We reviewed existing PHRs for diabetes and mental health care in Japan. In this study, members of the NCGM and NCNP reviewed all PHRs available through the Diabetes Information Center, to classify the contents (including depression care) of the PHRs. The inclusion criteria for the study were as follows: (1) PHRs of patients with diabetes in the community available through the Internet and (2) PHRs designed to share information across professionals, direct care staff, and local government staff.
We examined each record and created a table of elements. Six elements were categorized based on previous research22–24 on PHRs, as follows: (1) self-management support and patient education,22,23 (2) clinical follow-up,22,24 (3) linkage between physicians, 22 (4) linkage with team care staff, (5) linkage with mental health specialists, and (6) linkage to a notebook by the JADEC. 19
Development of PHR
Based on the examination of the previous PHRs, we developed a new PHR for patients with diabetes for integrating depression care into diabetes care for research and clinical purposes. Working members (NS-A, HI, TA, and HY) of this research proposed essential components in the medical record and discussed prioritizing importance of each element, classifying the elements, and rearranging categories. Easy structure for implementation in clinical practice and patient-centered perspective is key for the process. We only included a depression monitoring section because of feasibility to use in diabetes practice. Several clinical experts outside of the research team reviewed the proposed PHR, but not by patients. The PHR was distributed to patients with diabetes and will be revised based on patient feedback in the next phase of the research.
Ethical considerations
The study was approved by the Institutional Review Boards of the National Center of Neurology and Psychiatry (NCNP) as a part of a follow-up study of patients with comorbid physical and mental illness. Participants gave their written informed consent to participate in the research which was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Of the 12 PHRs that were available on the Internet, 8 sets of PHRs for people with diabetes met our inclusion criteria. The prefectures and organizations that developed the PHRs were the following: Chiba (Chiba Prefecture), Fukui (Fukui Prefecture Panel for Prevention and Treatment of Diabetes), Hyogo (Kobe City Hospital Organization Kobe City Medical Center West Hospital), Ishikawa (Minami-kaga Public Health and Welfare Center), Okayama (Okayama Prefecture), Shimane (Hamada Public Health Center), Tokyo (Itabashi Medical Association), and Toyama (Shinkawa Public Health Center).
The contents of each PHR are presented in Table 1. The length of these PHRs ranged between 1 and 36 pages. Five sets of PHRs had sections on self-management support and patient education. Two sets of PHRs had sections on medication adherence (Ishikawa and Toyama). All of the PHRs had a clinical follow-up section on nephropathy, neuropathy, and retinopathy and a section with linkages to dentists and ophthalmologists. There were no PHRs that had a section on depression monitoring. Linkages to nephrology and orthopedics were included in two PHRs (Fukui and Okayama) and one PHR (Ishikawa), respectively.
Regarding multidisciplinary team staff, linkages with dietitians and pharmacists were observed in five PHRs. Three PHRs had a section on certified diabetes educators (CDEs). In Okayama Prefecture, CDEs documented their services on an independent sheet. Three PHRs were linked with the JADEC tool. No PHRs included depression monitoring and/or treatment. There were no PHRs that showed the follow-up period, the number of patients who used each PHR, and history of revisions of each PHR.
Based on our search review, we reached a consensus regarding the important components of PHRs. Table 1 (right column) shows an outline of an ideal PHR with seven sections, including the following: introduction, education (diabetes, treatment, stress coping), medical history (outline, recent reports), monitoring (laboratory test, others), service linkage and communication tools, cost, and others.
PHRs for patients with diabetes. *
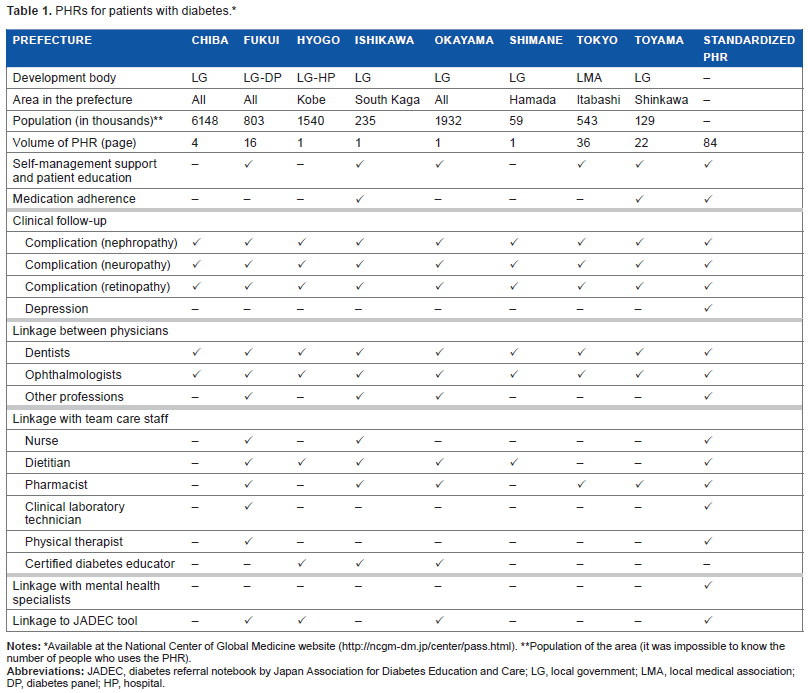
Available at the national Center of Global Medicine website (http://ncgm-dm.jp/center/pass.html).
Population of the area (it was impossible to know the number of people who uses the PHR).
Discussion
Our results show that eight types of PHRs exist for patients with diabetes in Japan. All PHRs had a section on clinical follow-up and linkage with dentists and ophthalmologists. Linkages with primary physicians and nonphysician interdisciplinary team members varied by PHR. No PHRs integrated diabetes and depression care.
All PHRs had components following up of complications and linking diabetes care and other medical care, such as dentists and ophthalmologists. Diabetes complications worsen prognosis and are an important target in clinical diabetes care, along with glycemic control. Continuous monitoring of diabetes complications, referrals to appropriate secondary care if necessary, and communication among physicians are key to improving patient outcomes. Finally, some PHRs recommend using JADEC's care pathway with each PHR.
Unfortunately, no sections of the PHRs included depression or mental health care in this study. Depression is related to poor adherence to medication and an unhealthy lifestyle and results in a poor prognosis.8–16 Monitoring depression and using a linkage tool to mental health professionals in one section in local PHRs may help to improve outcomes.
It is worth noticing that CDEs are becoming important in Japan, and there were three sets of PHRs that have space for CDEs. Certified diabetes educator of Japan is a qualification awarded by the Japanese Certification Board for Diabetes Educators, to a nurse, dietitian, pharmacist, clinical laboratory technician, or physical therapist possessing wide specialist knowledge of diabetes, since 2000.25,26 In addition, CDEs who play an active role in local areas are called local certified diabetes educators. Local certified diabetes educators are trained in a manner corresponding to the conditions of an individual local area. Thus, it may be worth training CDEs to monitor depression and coordinate depression care with mental health specialists using the developed PHR.
The present study has several limitations. First, our research group examined easily accessed PHRs of patients with diabetes through the National Diabetes and Metabolism Information Center in the NCGM. Since other such records do exist (eg, in the Totuka area in Kanagawa and Kumamoto), our results did not cover all the records of patients with diabetes in Japan. Second, most of the PHRs were at the stage of distribution to residents of each community. Although we showed case examples, further research is necessary to assess the effectiveness of PHRs in the care of patients with diabetes and depression in the community. There were no information available that showed the follow-up period, the number of patients who used each PHR, and history of revisions of each PHR.
It is important to know the coverage rate per population in each PHR. Revision of PHRs is necessary based on further results and discussion with diabetes staff. For example, more information on depression is needed. Despite these limitations, our results highlight the challenges faced when developing PHRs for people with diabetes and depression in the community.
Conclusions
Results of this study showed that the existing patient-held record is not suitable for patients with diabetes and depression. We demonstrated a new patient-held record specific to those with comorbid diabetes and depression.
Author Contributions
Agree with manuscript results and conclusions: NSA, HI, TA, HY, KK, DN, KN, and MN. Jointly developed the structure and arguments for the paper: NSA, HI, TA, HY, KK, DN, KN, and MN. Made critical revisions and approved final version: NSA, HI, TA, HY, KK, DN, KN, and MN. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
This study was supported by the Health and Labour Sciences Research Grant for Comprehensive Research on Disability Health and Welfare from the Japanese Ministry of Health, Labour, and Welfare. We thank Dr. Miyako Kishimoto and Dr. Ritsuko Yamamoto-Honda of the National Center for Global Health and Medicine for providing valuable comments and information. The authors declare that there is no conflict of interests regarding the publication of this paper.