
Abstract
We report a 52-year-old female with end-stage osteoarthritis of the hip accompanied by acetabular dysplasia in whom quality of life (QOL) was improved by Kampo treatment. When she was 42 years old, she developed pain in the left hip joint, and early-stage OA of the hip was diagnosed by hip joint x-ray. Therefore, she took NSAIDs, and received conservative therapies such as diet and muscle training. However, pain in the hip joint increased and her activity of daily life (ADL) decreased at the age of 50, although she continued to receive the conservative therapies. At the age of 52, she consulted our department requesting Japanese Oriental (Kampo) Medicine. Kampo formulae; Keishikaryojutsubuto (12Tab/day: Kuracie Co. Ltd. Japan), and Boiougito (7.5 g/day: Kuracie Co. Ltd. Japan), were administered. Treatment for 3 months resulted in a decrease in the left hip joint pain using visual analogue scale (VAS) and improvement of her ADL. One year later, her joint symptoms have not increased, and both the Harris hip score and the clinical evaluation criteria of osteoarthritis of the hip have improved.
The course of this disease varies depending on the lifestyle of the patient, and Kampo formulations may offer safe, potent supplemental treatment.
Introduction
Osteoarthritis (OA) of the hip induces regressive changes in the hip joint cartilage and subsequent abnormality in the synovial membrane and articular capsule, leading to the impairment of joint function, and osseous changes also occur. The prevalence of this disease is not high, 1 but coxalgia and surrounding pain and limitation of the range of motion occur, and subsequently limit ADL with the progression of lesions.
OA of the hip is classified into primary and secondary cases based on the presence or absence of causes. Primary OA of the hip is defined as coxarthrosis with normal hip joint alignment and acetabular formation. 2 In Japan, primary cases account for only 0.65%, and many cases are secondary. 2 The cause of secondary OA of the hip in which lesions are localized in the hip joint includes congenital hip joint dislocation, acetabular dysplasia, necrosis of the femoral head, and Perthes's disease. When acetabular dysplasia remains in the growth period, it may become OA of the hip. 3 When the femoral head is impaired with the treatment of congenital hip joint dislocation, deformation of the femoral head and neck occurs. These are the most frequent causes of secondary OA of the hip.
The natural course of this disease is diverse and classified based on the severity of joint deformation into pre-, early, progressive, and end-stage coxarthrosis, but it does not necessarily progress with aging. The natural course is influenced by the lifestyle, and it has been reported that X-ray radiographic findings improved in some cases. 4 Conservative or surgical treatment is selected in the natural course, and the timing is dependent on individual cases. In Japan, Kampo has been clinically applied for rheumatic diseases for centuries. In this study, we applied Kampo for progressive to end-stage coxarthrosis in a female in her 50 s, and achieved improvement of the hip joint function and QOL. Herein, we report the case along with a literature review.
Case Report
We encountered a 52-year-old woman with end-stage OA of the hip accompanied by acetabular dysplasia in whom the quality of life (QOL) was improved by Kampo treatment.
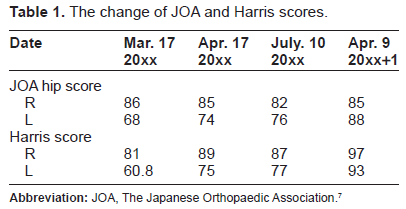
She had demonstrated acetabular dysplasia at birth, and dislocation of the hip was treated with a plaster cast. Although anterior coxarthropathy was noted by a general practitioner at the age of 31, she was observed without treatment, due to the absence of joint symptoms. At the age of 42, she developed pain in the left hip joint, and early-stage OA of the hip was diagnosed. Therefore, she took non-steroidal anti-inflammatory drugs (NSAIDs), and received conservative therapies such as diet and muscle training. However, pain in the hip joint increased and her ADL decreased at the age of 50. Nevertheless, she continued to receive conservative therapies, although her symptoms did not change. At the age of 52, she consulted our department requesting Japanese Oriental (Kampo) Medicine. There were no abnormalities on blood and biochemical analysis. Hip joint X-ray showed end-stage OA in the left hip joint (Fig. 1). We administered the Kampo formulae; Keishikaryojutsubuto (12Tab/day: Kracie Co. Ltd. Japan), and Boiougito (7.5 g/day: Kracie Co. Ltd. Japan), according to the traditional diagnostic system 5 . The arthralgia was evaluated by visual analogue scale (VAS). Treatment for 3 months resulted in a decrease in hip joint pain as well as improvement of her ADL. One year later, her joint symptoms have not increased, and both the Harris hip score 6 and the Japanese Orthopaedic Association (JOA) hip score 7 have improved (Table 1). Although Kampo treatment continued over one year without discontinuation, there were no adverse effects.

Hip joint X-ray. The image shows joint space narrowing, osteosclerosis and osteophyte formation in left hip joint, accompanied by the dysplastic hip.
The change of JOA and Harris scores.
Discussion
Osteoarthritis of the hip begins with degeneration or wear of the joint cartilage, and various articular changes progress. It is considered that degeneration and wear of cartilage occur when mechanical loads, such as labor, exercise, and trauma, are added to background factors, such as race, gender, aging, obesity, and heredity. The metabolic disorder of chondrocytes occurs and cartilage destruction progresses, which induces inflammation of the synovial membrane and causes swelling of the joint and bone destruction. It progresses from pre-coxarthrosis → early stage → progressive stage → end stage in the general natural course, and various clinical symptoms appear in each disease stage.
There is ‘primary’ and ‘secondary’ osteoarthritis of the hip, as described above, and the presented case involved acetabular dysplasia-associated secondary coxarthrosis. In Japan, most patients with this disease are female, as was this patient. In treatment, conservative treatment is prioritized, such as instruction in daily living and physical and drug therapies, but some physicians consider that surgery in the early stage is desirable, even though symptoms are mild, when progression is apparently predicted. Various surgical methods have been proposed corresponding to the condition and stage of acetabular dysplasia and coxarthrosis (various osteotomy procedures, shelf operation, and total hip replacement).
The patient showed end-stage coxarthrosis on X-ray radiography, and felt pain not only while going up and down stairs but also when walking, limiting ADL. However, pain was rapidly alleviated after the initiation of Kampo treatment (Keishikaryojutsubuto and Boiougito) and ADL improved. Methods to judge therapeutic effects on osteoarthritis of the hip are roughly divided into comprehensive health scales8,9 widely covering physical functions through mental health and disease-specific scales specialized for specific diseases including coxarthrosis. Of the latter, the Harris hip score 6 is the most internationally common criteria. It is comprised of pain (44 points), function (47 points), deformation (4 points), and range of motion (5 points). Pain is divided into 6 categories, and function is comprised of the walking ability (33 points) including claudication, support for walking, walking distance, and daily living activities (14 points) including going up and down stairs, wearing shoes and socks, sitting, and the use of public transportation. The clinical evaluation criteria of osteoarthritis of the hip most commonly used in Japan are the hip joint function assessment criteria established by the Japanese Orthopedic Association (JOA hip score). 7 The current JOA hip score was prepared in 1995 based on the old JOA hip score established in 1971, and it is comprised of the following 4 items: pain (40 points), range of motion (20 points), walking ability (20 points), and daily living activities (20 points). Categories proposed by Charnley, such as unilateral, bilateral, and multiple joint developments, were adopted. The maximum score of the range of motion is 20 points, accounting for a large proportion of the overall score, compared to that in the Harris hip score. In this patient, the JOA and Harris hip scores improved over the about one-year course, and so we consider that the objective effect of Kampo treatment was exhibited.
In Japan, Kampo drugs are covered by national health insurance and clinically applied for various diseases. Arthralgia has been treated with Kampo for centuries, and many Kampo formulations are administered for osteoarthritis, 10 rheumatoid arthritis, 11 and psoriatic arthritis. 12 This kind of remedy is often used with several joints such as a knee joint 13 in addition to hip joint caused by some pathogenesis such as degeneration, metabolism or inflammation. Although there has been no report on administrations of Boiogito and Keishikaryojutsubuto for osteoarthritis of the hip, an effect on osteoarthritis of the knee comparable to that of NSAIDs and synergistic effect with NSAIDs have been reported. 14
The mechanism of the effect of Kampo on osteoarthritis has not been clarified. Pathologically, cracks and erosion occur in the cartilage surface in excessively loaded regions, loosing joint cartilage, in osteoarthritis of the hip. In the deep layer of joint cartilage, blood vessels invade calcified cartilage, and subchondral bone comes to exhibit a bone effect. On the other hand, osteophytes are formed in non-loaded regions. For rheumatoid arthritis, an immunomodulatory effect of Kampo has been shown, 15 and the inhibition of bone destruction in some cases has been reported. 16 The inhibition of bone turnover in osteoarthritis is assumed.
Additionally, there is another problem in this kind of treatment. Namely, Kampo Medicine has the important feature that differ from Western Medicine; the diagnostic system in Kampo medicine is different from that in Western medicine. Therefore, it is surely thought that Kampo diagnosis may not be easy for readers to understand. When we treat RA patients with Kampo Medicine, it is necessary to make a Kampo diagnosis as well as a diagnosis by Western medicine. This issue makes it difficult to perform controlled clinical trials. In this case, we selected the keishikaryojutsubuto and boiogito according to the traditional diagnosis system. The target group for keishikaryojutsubuto and boiogito is follows: easy fatigability, coldness, obesity, sweating with swollen joints.5,17
Furthermore, Kampo formulae are generally composed of several herbal components, but not purified chemical compound. Therefore it is considered that these remedies are safe. However, pseudoaldosteronism by licorice root is well known to be an adverse effects of herbal medicine, and there are also allergic effects, such as skin eruptions and liver injury, that can be induced by crude drugs.18–20
In summary, we reported a patient with end-stage osteoarthritis of the hip accompanied by acetabular dysplasia in whom the QOL was improved by Kampo treatment. Although the clinical use of this remedy should be with careful deliberation due to the absence of evidence, the course of this disease varies depending on the lifestyle among patients and Kampo formulations may offer safe, potent supplemental treatment. The clinical course of a present patient may open the way to the achievement of randomized controlled trials and the further basic analysis of this remedy in the future.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.