
Abstract
Objective
To describe a patient with erhythema and edema after Radix Astragali was added to a kampo formula.
Case summary
A 21-year-old male, who was diagnosed as having atopic dermatitis in 1989, demonstrated systemic dry eruptions and consulted our department for treatment with traditional herbal medicine (THM) in 2004. The oral administration of herbal medicine resulted in decreased symptoms as well as a reduction in the serum IgE level. In August 2007, he complained of sweating on the neck and we added Radix Astragali to the previous formula. About 18 hours after he ingested the new formula including Radix Astragali, erhythema appeared with swelling of the bilateral hands and feet. Administration of the formula was discontinued and about 48 hours later, his symptoms had almost disappeared. Astragaloside, which is the main ingredient of Radix Astragali, was negative on lymphocyte transforming test (LTT) and we could not determine the ingredient that induced erhythema.
Conclusion
We consider that the Radix Astragali induced acute erhythema with swelling based on the clinical course. Acute edematous erythema due to THM is very rare and we discuss allergic reactions to traditional herbs and review the litrature.
Keywords
Introduction
Radix astragali, OgiR is prepared from the root of Astragalus membranaceus Bunge or A. mongholicus Bunge, and is one of the representative herbs used in the field of traditional herbal medicine (THM: called Kampo in Japan). The main components consist of flavonoids such as formononetin, 3‘-hydroxyformononetin, l-canavanin and saponins such as astragaloside, sayasaponin. This herb is usually used in the form of decoctions having a tonic-effect. It has been reported that this drug has pharmacological actions such as immunomodulatory effects, anti-inflammatory effects and anti-allergic effects.1,2
This paper describes a rare case of a patient with atopic dermatitis (AD) demonstrating edematous erythema thought to be caused by adding Radix astragali to a kampo formula.
Case Report
The patient consulted our hospital in April 2004 at 21 years of age, with systemic dry eruptions associated with AD.
In 1989, he developed systemic eruption with itching and was diagnosed as having AD at a local hospital. He was treated with ointment containing steroids and his condition periodically became somewhat better or worse. However, his symptoms gradually worsened recently and the use of ointment containing steroids was discontinued. Thereafter, he consulted our hospital with a request for herbal medicine in 2004. At the first medical examination in April 2004, he had severe dry eruptions on the neck, chest, bilateral upper and lower extremities, especially, eczema with lichen on the neck. His laboratory data were as follow: White blood cell: 7400/mm3, eosinophil: 14.9%, immunoglobulin (Ig)-E: 15012.6 mg/dl, C-reactive protein (CRP): 0.1 mg/dl, lactate dehydrogenase (LDH): 226IU/l. Hepatic, renal and thyroid function was normal. Kagen-ichiin-sen (KIS; decoction: Uchida Co. Ltd Tokyo Japan; Table 1) was prescribed per mouth daily, based on the traditional diagnostic system. 3 Briefly, the indications for KIS are eczema and pruritis with dry skin and dotty or diffuse pigmentation. The oral intake of KIS resulted in a decrease in symptoms as well as a reduction of the serum IgE level (3863.7 mg/dl) on Feb. 2007.
Herbs composed of Kagenichiin-sen.
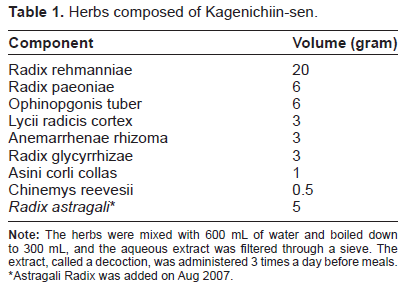
Astragali Radix was added on Aug 2007.
In August 2007, he complained of sweating on the neck and we added Radix Astragali to KIS, since the indication for Radix Astragali is eruptive eczema with sweat. 3 However, about 18 hours after he ingested the full day's dose (twice a day) including Radix Astragali, erhythema with swelling of the bilateral hands and feet appeared (Fig. 1A). There was no swelling of the superficial lymph nodes. Although the eosinophil count and serum LDH level did not change, the serum CRP level increased slightly (0.3 mg/dl). Anti-nuclear antibody was negative, and there were no apparent monoclonal gammopathies. Administration of the altered formula was discontinued and 2 days later, his symptoms had almost disappeared (Fig. 1B) and the serum CRP level was <0.1 mg/dl. Thereafter, he continued intake of the original KIS formula and his condition stablized.
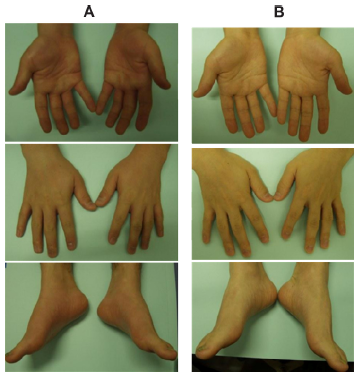
A) Eighteen hours after administration of Radix Astragali. Edematous erythema with a sensation of heat at the hands and feet. Upper panel: the palm, Middle panel: the back of hands, Lower panel: feet. B) Forty-eight hours after discontinuation of Radix Astragali intake. Edematous erythema had almost disappeared.
Analysis by Ltt Using Herbal ingredient
The patient refused oral provocation with a low concentration of Radix Astragali. Therefore, lymphocyte transformation test (LTT) was performed with his consent. LTT for THM is unreliable because of the likelihood of a false positive results. 4 Thus, LTT for the main ingredient of Radix astragali was utilized, and as a result astragaloside was negative on LTT (Table 2). This assessment was approved under the comprehensive agreement provided by Gunma University Hospital.
The results of lymphocyte transformation test for herbal ingredients.

Stimulation Index: astragaloside or saikosaponin/no treatment;
Saikosaponin was utilized as negative control among herbal ingredient
PHA, phytohemagglutinin.
Discussion
THM, which is covered by national health insurance in Japan, is generally used in the field of primary health care, and is also administered as an alternative remedy for chronic diseases such as AD. Although it is considered that THM is generally a safe drug, some adverse effects are known. Drug eruption is an occasional adverse effect in THM and several cases have been reported.5–11 Recently reported cases of drug eruptions due to THM are summarized in Table 3. Discontinuation of each drug resulted in the improvement of drug eruptions in all cases. Two cases of drug eruption induced by Radix Astragali have been reported, one patient (No. 7) showed lichenoid planus 3 weeks after the start of Radix Astragali intake. In contrast, another patient (No. 2) showed edematous erythema with fever and oliguria that appeared 24 hours after taking medicines containing Radix Astragali. Although physicians consider that drug eruption due to THM is generally mild, it should be understood that a few patient may show acute edematous erythema such as erythroderma. Generally, erythema with a heat sensation in erythroderma spreads over the whole body within 12–48 hours. The present case also showed edematous erythema 18 hours after the drug-intake, but erythema involved the hands and feet. It is unclear whether the present patient would have developed an acute erythroderma if the administration of Radix astragali had continued.
List of recently reported cases of drug eruptions due to THM. *
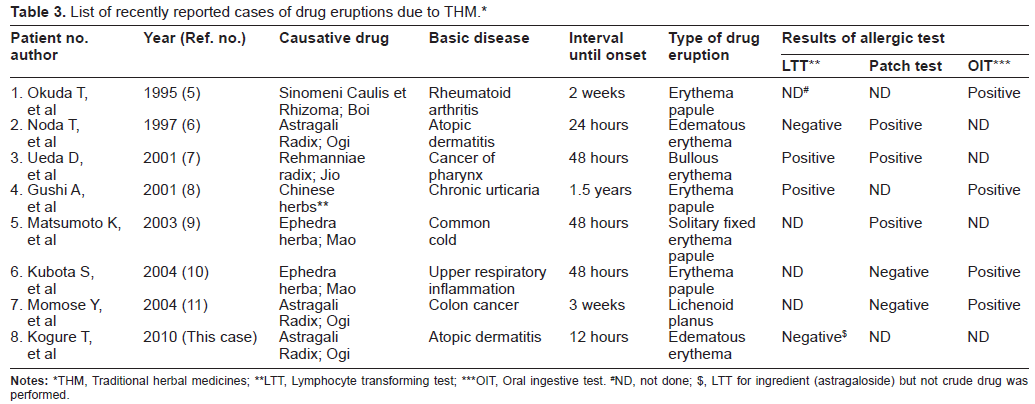
THM, Traditional herbal medicines;
LTT, Lymphocyte transforming test;
OIT, Oral ingestive test.
ND, not done;
LTT for ingredient (astragaloside) but not crude drug was performed.
Incidentally, in this case it was nesessary to rule out hereditary/acquired angioedema in the differential diagnoses. Unfortunately, we failed to measure the complements (eg, Serum C1q/C3/C4) and C1 esterase inhibitor. Therefore, we are not able to diagnose the allergic edematous erythema more precisely. However, we regarded the clinical manifestation of the present patient as allergic edematous erythema because of the improvement following discontinuation of drug, absence of monoclonal gammanopathy and absence of any classification for autoimmune diseases.
Although Radix astragali have several bioactivities such as immunomodulatory and the vasodilative effects,1,2 there was a limited quantity of the components of Radix astragali in the decoction. Therefore, edematous erythema is probably induced by an allergic response to Radix astragali. Generally, it is difficult to confirm that a traditional herb must be the causative drug in an allergic reaction. LTT for THM is unreliable because of the likelihood of false positive results. 4 Therefore, we performed LTT using only the main component of Radix astragali. However, the causative ingredient could not be confirmed. There are two possibilities for these results: one is the likelihood of a causative components other than astragaloside and another is that plural components (crude drug) may be associated with the allergic reaction.
In fact, it is considered that interstitial pneumonia induced by Shosaikoto is probably an allergic reaction for the crude drug: shosaikoto. 12 To certify the causative drug in the field of dermatology, patch test using crude drug has became prevalant. Evaluating previous reports, the patch test was carried out in 5 cases (No. 2, 3, 5, 6, 7 in Table 2). Three cases (No. 2, 3, 5) showed positive results and the causative drug was determined. In contrast, 2 patients (No. 6, 7) had negative results, but interestingly, these patients agreed to an oral ingestion challenge test and showed positive results. Therefore, we consider that assessment of the clinical course must be important when prescribing crude drugs such as traditional herbs.
Another important question is whether a high serum level of IgE may have been associated with the occurrence of allergic edematous erythema in this patient. There is no report demonstrating that drug allergy occurs more often in patients with AD in comparison with healthy subjects. Based on several investigations, 13 14 it is generally considered that a high serum level of IgE in AD patients is a result, not a cause. However, it is known that a high serum IgE condition increases IgE-mediated type I hypersensitivity reaction through Fc ε receptorl (Fc ε RI) on mast cells. 15 Possibly, edematous erythema having occurred in this patient was caused by an IgE-mediated allergic mechanism. Therefore, it is possible that edematous erythema might have been induced by Radix astragali due to the high serum levels of IgE in this patient. However, we could not identify a causative component using LTT Since LTT examines lymphocyte (non-IgE)-mediated allergic reactions, LTT might fail to show the positive result.
Herein, we presented a case of an atopic dermatitis with acute edematous erythema caused by Radix astragali. While the causative component could not be determined by LTT, it is estimated that the edematous erythema must have been caused by Radix astragali based on the clinical course of this patient. In eruptions caused by crude drugs, the causative agent should be determined from a comprehensive perspective. 5
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material. Written consent was obtained from the patient or relative for publication of this study.
Footnotes
Acknowledgments
This study was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science.