
Abstract
We present three rheumatoid arthritis (RA) patients successfully treated with traditional herbal medicine (THM: Kampo). The treatment with THM resulted in a decrease in RA disease activity such as DAS28, as well as in the serum levels of anti-cyclic citrullinated peptide antibodies (anti-CCP) in 3 cases.
These observations suggest that disease progression may be retarded in patients who respond to THM since anti-CCP is important for the prediction of disease severity and radiographic joint damage. Additionally, serial mesurements of anti-CCP titers may be a useful indicator in assessing this kind of treatment efficacy.
Introduction
RA is a polyarticular chronic inflammatory disease characterized by cartilage destruction and bone erosion. Disease modifying anti-rheumatic drugs (DMARDs) may retard disease progression. Recently, specific treatments, infliximab or etanercept, have targeted relevant proinflammatory cytokines, such as tumor necrosis factor alpha (TNF-α). In Japan, traditional herbal medicines (THM: Kampo) have also been used as adjunctive agents for RA treatment. 1 Although the clinical effects of THM have been shown by several investigators,2,3 it is still not obvious whether THM supresses the progression of joint damage.
An assay for anti-cyclic citrullinated peptide antibodies (anti-CCP) has been developed in recent years, although the diagnosis of rheumatoid arthritis (RA) depends primarily on clinical manefestations supported by several serological findings such as rheumatoid factor (RF). Anti-CCP is useful in the preclinical and early diagnosis of RA, and is also important for the prediction of disease severity and radiographic joint damage.4,5
In this report, we described three patients with RA who were successfully treated with THM and demonstrated a decrease in serum levels of anti-CCP, and reviewed the literature on changes in anti-CCP in response to various medications for RA.
Case Report
Case 1
In 2003, a 61-year-old female developed pain, swelling and stiffness of the bilateral wrist joints and was diagnosed as having RA at a local hospital. She was treated with bucillamine: 100 mg/day, and her condition remained in remission for approximately one year. In 2004, she developed polyarthralgia again and was additionally treated with methotrexate (MTX) and salazosulphapyridine (SASP), while SASP was discontinued due to eczema. However, polyarthralgia persisted, and the patient discontinued administration of MTX and bucillamine by herself in August 2006. Thereafter, she consulted our hospital with a request for herbal medicine in September 2006. At the first medical examination, she had severe polyarthralgia. There were no significant findings on physical examination of the neck, chest and abdomen. Laboratory data were as follow: hemoglobin (Hb): 9.9 g/dl, erythrocyte sedimentation rate (ESR): 114 mm/hour, C-reactive protein (CRP): 13.2 mg/dl, rheumatoid factor (RF): 242 IU/ml, Matrix metalloproteinase-3 (MMP-3): 1839.5 ng/ml, Antinuclear antibody (ANA): negative. Hepatic, renal and thyroid function was normal. Keishinieppiitto-ka-ryojutsubu (KER; decoction: Uchida Co. Ltd Tokyo Japan) was prescribed per mouth daily without the DMARDs treatment according to the diagnosis by THM under informed consent. After 3 months, treatment with KER alone resulted in improvement of her symptoms, as well as a decrease in the serum levels of a series of serological markers (Fig. 1). This patient was categorized as showing a good response (5.21 to 2.90) according to DAS28; CRP(3) method (DAS28). Furthermore, her serum level of anti-CCP also decreased (Fig. 1).

Clinical course (Case 1: a 61-year-old, female). The treatment with traditional herbal medicine resulted in good response according to DAS28, as well as the considerable decrease in serum level of aCCPab titer.
Case 2
In 2002, 68-year old female developed pain at the bilateral metacarpopharangeal (MCP) joint and wrist joints. She consulted a local hospital and was diagnosed as having RA. She was treated with sodium aurothiomalate (GST) 10 mg;im/month and actarit 300 mg/day. Although her condition remained in remission during approximately three years, she developed the arthralgia at the bilateral wrists and shoulders. Therefore, she consulted our hospital with a request for herbal medicine in July 2006. At the first medical examination, she demonstrated mild deformity in the bilateral MCP and wrist joints. There were no significant findings on physical examination of the neck, chest and abdomen. Laboratory data were as follow: Hb: 12.1 g/dl, ESR: 66 mm/hour, CRP: 3.5 mg/dl, RF: 119 IU/ml, Antinuclear antibody (ANA): negative. Hepatic, renal and thyroid function was normal. The administration of actarit was continued, but treatment with GST was stopped. In addition, KER was prescribed per mouth daily as an adjunctive with actrait. Three months later, joint symptoms improved, and the serum levels of serological markers, as well as anti-CCP have considerably decreased (Fig. 2). This patient was also categorized as showing a good response (4.95 to 2.60) according to DAS28.

Clinical course (Case 2: a 68-years old, female).
Case 3
A 57-year old female developed a low fever, and bilateral wrist joint pain in June 2006. She consulted a local hospital and was diagnosed as having RA since RF was positive. Prednisolone (PSL) 10 mg/day and methotrexate (MTX) 6 mg/w were initiated in July and symptoms improved. However, when the PSL dosage was reduced, the condition worsened again. Thereafter, she consulted our hospital with a request for herbal medicine in October 2006. At the first medical examination, she had severe polyarthralgia in the bilateral MCP and wrists, knees, and right shoulder joints. There were no significant findings on physical examination of the neck, chest and abdomen. Laboratory data were as follows: Hb: 9.5 g/dl, ESR: 124 mm/hour, CRP: 6.5 mg/dl, RF: 185 IU/ml, Antinuclear antibody (ANA): negative. Hepatic, renal and thyroid function was normal. We reduced PSL dosage from 10 mg/day to 5 mg/day, and continued the administration of MTX. Additionaly, we prescribed KER. After 2 months her symptoms decreased, and 6 months later, the serum levels of a series of serological markers containing anti-CCP was decreased (Fig. 3). PSL dosage was reduced 3 mg/day at August 2007. This patient was also categorized as showing a good response (5.37 to 2.30) according to DAS28.
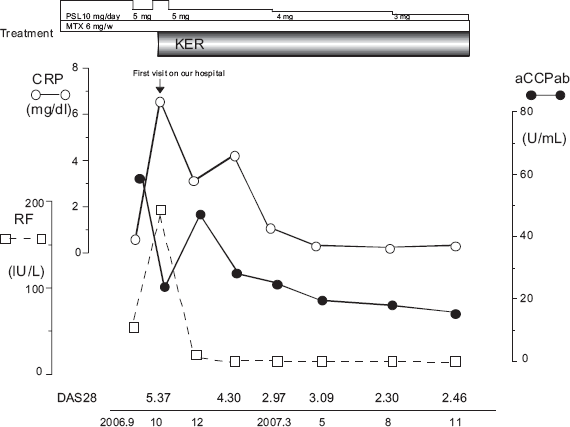
Clinical course (Case 3: a 57-years old, female).
Discussion
THM (Kampo), which is covered by national health insurance in Japan, is often used in the field of primary care, and also applied as the alternative remedy for serious diseases such as RA. In RA, clinical effects of THM were reported by several investigators and its immunomodulatory effects were demonstrated in several mouse models of arthritis.1–3 The components of KER, which is crude drug, are shown in Table 1. This is commonly prescribed kampo formula and we have demonstrated that KER treatment decreased the serum level of RF, as well as disease activity using self-control trial. 6 However, it remains unclear whether THM supresses the progression of joint damage because randomized controlled trials (RCT) have not been carried out. In this regard, we monitored the change in serum levels of anti-CCP, which can be a prognostic marker of erosive damage.
The herb composed of Keishiniepppiittoka-ryojutsubu (KER).

Twelve herbs were mixed with 600 ml of water and boiled down to 300 ml, then the aqueous extract was filtered through a sieve. The extract (300 ml/day), called a decoction, was administered 3 times a day before meals. The preparation of the decoction was performed by each patient under the guidance of a pharmacist.
Recently, the clinical significance of the serial determination of anti-CCP has been discussed. Meyer et al. has reported that serially determined anti-CCP during the three years of follow-up is more useful than the baseline determination for predicting radiographic progression in patints with RA. 7 We have also demonstrated that RA patients in whom the serum level of anti-CCP did not decrease demonstrated severe progression of joint damage while mild progression of the erosive lesion was observed in RA patients with a decrease in anti-CCP. 4 Responders to THM presented in this report showed serum levels of anti-CCP decreased in parallel to other serological markers including RF, permitting the speculation that treatment with THM suppressed the progression of joint damage.
Effects on the serum level of anti-CCP are variable with each drug. It has been reported that MTX did not influence on the production of anti-CCP. 8 Although MTX was administered a month before the start of THM in case 3, it is considered that the decrease in serum level of anti-CCP was attributed to the treatment with KER. According to TNF-α blocking agents (infliximab or etanercept), several diverse results in patients showing clinical improvement have been reported. First anti-CCP titer is unchanged by anti-TNF-α treatment,9,10 second its treatment results in a decrease in anti-CCP titers, 11 and third anti-CCP decreases at 6–7 months but returns to the baseline. 12 The difference among these reports can not be explained although many investigators have highlighted the significant variations in anti-CCP titers among patients treated with anti-TNF-alpha drugs. Additionally, the prognosis for joint damage remains obscure in the patients, whose anti-CCP titer was not decreased by anti-TNF-α drugs treatment. In the present report, 3 patients, responders to THM, showed a decrease in the serum level of anti-CCP, suggesting that THM may be a useful agent for the treatment of RA as an adjunct to DMARDs or anti-TNF-α drugs, since several studies demonstrated that the decrease in the serum level of anti-CCP predicts an absence of radiographic progression.4,7 However, this suggestion would be limited to responders, but not non-responders to THM.
Treatment with THM resulted in a decrease in the serum level of anti-CCP, as well as RF. Rycke et al 9 has described that RF and anti-CCP antibodies are two, independent antibody systems in RA. Therefore, treatment with THM may act on both pathways in THM responders. The mechanisms whereby THM could lead to a decrease in the generation of autoantibodies such as anti-CCP and RF are not understood, and the explanation of this phenomenon remains unclear. However, it has been shown that THM can downregulate the several inflamatory cytokines and mediators,2,3,13,14 and these immunomodulatory effects may account for a reduction in autoantibody generation.
In conclusion, three patients with RA were successfully treated with Traditional Herbal Medicine (THM) and demonstrated a decrease in their serum levels of anti-CCP and RF. These mesurements may be a useful adjunct in assessing the efficacy of this kind of treatment.
Disclosure
The author reports no conflicts of interest.
Footnotes
Acknowledgments
This study was supported by a Grant-in-Aid for Scientific Research from the Japan Society for the Promotion of Science.