
Abstract
The incidence of non-alcoholic fatty liver disease (NAFLD) is rising rapidly in parallel with obesity rates. The underlying pathogenesis of NAFLD remains an enigma but is largely influenced by individual lifestyle choices involving diet and exercise. Therefore, studies have highlighted the importance of calorie reduction and macronutrient composition (eg, carbohydrate and fat) in modifying disease outcomes. Micronutrients are also believed to play a role in disease progression. There are now an increasing number of studies linking vitamins with NAFLD, particularly vitamin E, and the supplementation of several different vitamins has been demonstrated as a promising therapeutic option in the treatment of NAFLD. This review provides a broad overview of the potential role of vitamins in NAFLD development and disease management.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is characterized by increased fat accumulation as triglycerides in the liver, 1 which can manifest as a wide spectrum of conditions: from hepatic steatosis to more severe steatohepatitis with fibrosis, cirrhosis, and potentially hepatocellular carcinoma. 2 Currently, NAFLD is the most common liver disease of the Western world, largely due to obesity induced by readily available high-energy food and sedentary lifestyle of the modern society. As a consequence, the incidence of NAFLD is rising drastically in tandem with the rising rates of obesity worldwide. Currently, the prevalence of NAFLD stands at 24.4% globally, 3 and it is found to be even higher in patients with a background of Type 2 diabetes mellitus (T2DM) and other metabolic syndrome features. 4 The mortality rate and the number of liver transplantations due to NAFLD are also on the rise, and non-alcoholic steatohepatitis (NASH) is now the second leading indication for liver transplantation in the US.5,6 To prevent further exacerbation of this serious condition, it is necessary to find more effective interventions. Recently, in a large cross-sectional study of patients with liver biopsies, Dongiovanni et al. 7 showed a protection from liver damage in those patients who are at risk of non-alcoholic steatohepatitis after a statin treatment. 7 Lifestyle modification, involving exercise and dietary adjustment with reduced calorific content, continues to be the core therapeutic approach for NAFLD. However, several studies have highlighted that perhaps a reduction in energy alone is not sufficient for the alleviation and prevention of NAFLD; the dietary compositions, both macronutrient and micronutrient, may also play a crucial role in the manifestation and development of NAFLD. For example, recent studies have highlighted the importance of dietary vitamin composition and liver fat accumulation. Vitamins are essential micronutrients in the maintenance of health, which cannot be synthesized sufficiently from other molecules alone. Currently, there are 13 known vitamins: four lipid soluble (A, D, E, and K) and nine water soluble (groups B and C). 8 Until now, most review articles have summarized studies of a specific micronutrient/vitamin on hepatic metabolism, whereas the aim of this article was to provide a broader overview of the role of vitamins in NAFLD development and management.
Pathogenesis of NAFLD
To understand whether and how vitamins play a role in the mechanism of NAFLD, it is necessary to know how NAFLD is manifested. The
Genetically, studies have further supported the importance of the genetic background on NAFLD development: genome-wide association studies have identified the patatin-like phospholipase domain-containing 3 (PNPLA3) and the transmembrane 6 superfamily member 2 (TM6SF2) as genes related to the susceptibility of NASH.7,13
In addition, recent studies have shown that the alteration of innate immunity has an influential role in NAFLD. This is consistent with the fact that liver is often considered a major immune organ and has a wide repertoire of immune cells: dendritic cells (DCs), Kupffer cells (KCs), natural killer (NK) cells, and natural killer T (NKT) cells. Hepatic stellate cells, known to be responsible for collagen production, also exhibit immune properties by presenting antigens. 14 Other studies have indicated the involvement of immune system in the etiology or progression of NAFLD. Both NAFLD patients and animal models showed an increased number, but impaired phagocytic function of KCs.15,16 NKT cell number was reported to be decreased in the animal models of NAFLD, accompanied by an increase in inflammatory cytokines. 17 Similar observations of NKT cells were also found in patients with NAFLD, suggesting a protective role of NKT cells in NAFLD. 18 Interestingly, there is a new hypothesis for the role of microbiota composition in NAFLD, based on the observation that patients with obesity have an altered ratio of Bacteroidetes to Firmicutes, intestinal bacteria concentration, and decreased richness of other gut bacteria. 19 It is believed that microbiota composition causes NAFLD either by increasing the endotoxin level or by affecting the integrity of the tight junctions in the gut. 20
Taken together, the underlying pathogenesis of NAFLD is complex, and it might involve the interaction between innate immunity and the individual's microbiota composition. It is possible that the alteration of this axis is related to vitamins as they are known to have an immune modulatory role. Furthermore, the disruption of the gut integrity might affect the absorption and processing of the vitamins.
Several studies have highlighted the role of vitamin A in the pathogenesis of NAFLD. It has been demonstrated that retinoic acid effectively reduced adiposity in the liver and enhanced hepatic fat catabolism.
24
Furthermore, an
Vitamin B12 plays an important role in DNA synthesis and repair. 34 In humans, vitamin B12 exists in two forms: methyl cobalamin and 5‘-deoxyadenosylcobalamine. It is a cofactor for the mitochondrial enzyme, namely methyl malonyl CoA mutase, which is known to regulate the rate of long-chain fatty acyl-CoA transfer into the mitochondria, thereby influencing lipid metabolic pathways. 34 One prevailing theory of NAFLD is the change of mitochondrial environment, which leads to the overproduction of ROS. 35 Liver is an important storage site of vitamin B12, which has been linked to acute hepatitis, cirrhosis, and hepatocellular carcinoma. Studies have demonstrated the generation effect of B12 deficiency on the lipid metabolism in animal models. 36 It has been reported that low vitamin B12 in maternal diet induced higher rates of adiposity and T2DM in the offspring, which was accompanied by a change in hepatic gene expression involved in lipid metabolism pathways. Furthermore, the reconstitution of B12 to the offspring was able to normalize the alterations.36,37 In a study by Koplay et al, it was also observed that low serum B12 in patients with NAFLD was related to an elevated serum alanine aminotransferase (ALT) concentration. 38 In addition, vitamin B12 restriction in weaning female rats increased the body fat mass percentage, decreased fat-free mass, and impaired offspring capacity to secrete insulin. 39 Furthermore, offspring born to mothers with B12 deficiency had the dysregulation of pathways involved in fatty acid metabolism, amino acid metabolism, and glycolysis. The mechanism is believed to be due to the alterations of PPARγ and PPARα hepatic expression. It was further shown that the enzymes involved in β-oxidation were downregulated, affecting the lipolysis process. 39 Similarly, another study showed that offspring subjected to maternal vitamin B12 deficiency increased the plasma total cholesterol, and offspring born to dams fed B12 supplemented diet had standard plasma total cholesterol levels. 37 However, the protective role of vitamin B12 in NAFLD could be controversial. One human study attempted to examine the relationship between serum level of vitamin B12 and NAFLD. The patients with NAFLD were matched with control subjects; however, no difference was observed between the two groups. 40 This disparity could be due to the limited number of subjects in the study, which only involved 30 patients with NAFLD, and the results are based on one center alone.
Vitamin D might also modulate the hepatic status via the immune pathway. Calcitriol is synthesized by both innate and adaptive immune cells.
47
The landmark PIVENS study, a random controlled trial involving 247 adults with NAFLD, showed that vitamin E treatment comparing with pioglitazone and placebo over two years improved liver histology, reduced steatosis and inflammation, and decreased liver transaminases.59,60 Similar results were observed from pediatric populations. In children, Vos et al reported that the insufficiency in vitamin E consumption is related to higher grade of hepatic steatosis. 61 Similarly, Nobili et al studied in children with NAFLD receiving vitamin E treatment led to an improvement in transaminases and liver histology. 62 In a pediatric population of NAFLD diagnosed by biopsy, there was no significant improvement in ALT from daily 800 IU vitamin E after 96 weeks, although there was an improvement in hepatocellular ballooning score and NAS. 63 A possible explanation is that the treatment period was not sufficiently long enough to have an impact on the ALT level. In a separate random controlled trial involving 44 overweight/obese children aged 14–17 years, supplement with α-tocopherol and ascorbic acid was randomly given to the participants daily for four months. It was observed that the liver transaminases were moderately improved in the treatment group in comparison with the controls, further suggesting that vitamin E may have a beneficial role in NAFLD. 64 However, there is yet any study on the effect of vitamin E on children with biopsy-proven NAFLD.
Several studies have also highlighted the drawbacks of vitamin E. One study has shown that the daily administration of vitamin E increased the risk of developing prostate cancer in healthy men. 65 There are also contentious studies linking high-dose vitamin E supplementation with increased mortality. 66 Therefore, the effectiveness and safety of using vitamin E as a form of treatment require further study.
Literature on the role of vitamin K in the NAFLD is very limited; so far there is little evidence that vitamin K is involved in lipid metabolism. One study has reported the storage of vitamin K in the adipocytes, and there appeared to be a positive relationship between adult obesity and vitamin K concentration in the adipocytes. 69 However, studies are lacking in how and whether this micronutrient has a role in NAFLD at all.
Conclusion
Although this review is focused on the effect and possible mechanisms of action on NAFLD by each different vitamins, it is also important to highlight that there can be interactions between different vitamins, as well as between vitamins and micro/macronutrients intake. For example, it has been recently demonstrated that supplementation with vitamin A can compensate vitamin D deficiency. 70 Furthermore, other studies focused on cancer have also shown the relation between these two vitamins, 71 and it has been also described that the high levels of vitamin A can antagonize the effects of vitamin D. 72 On the other hand, the interaction between vitamins and micronutrients intake can affect obesity-associated features such as disturbances in lipid profile, inflammatory status, and insulin resistance, all of the key factors in the development of NAFLD. 73 Therefore, vitamins and micronutrient mixes have been also described as potential tools against the development of diet-induced NAFLD. 11
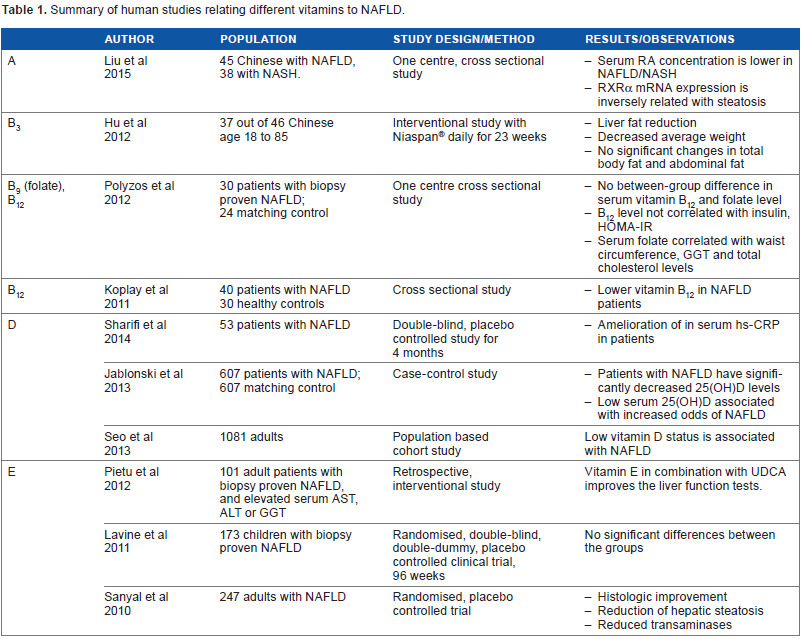
In conclusion, NAFLD is a complex chronic liver condition, with a strong association with obesity, and multiple factors influencing its pathogenesis. The underlying mechanism involves the modification and interaction of innate immunity and microbiota composition, among other factors. Although the role of dietary macronutrients in NAFLD pathogenesis is now better characterized, micronutrients such as vitamins may also play a key role. The current evidence appears to suggest a positive role of vitamins A, B3, B12, D, and E as therapeutic targets (Table 1), but some of them may also be linked with several adverse outcomes. Further, well-designed studies are therefore required to better define the potential role of these micronutrients in the development and treatment of NAFLD.
Summary of human studies relating different vitamins to NAFLD.
Author Contributions
Wrote the first draft of the manuscript: JL, PC. Contributed to the writing of the manuscript: JL, PC, VN, JO. Agree with manuscript results and conclusions: JL, PC, VN, JO. Jointly developed the structure and arguments for the paper: JL, PC, VN, JO. Made critical revisions and approved final version: JL, PC, JO. All authors reviewed and approved of the final manuscript.