
Abstract
This comprehensive review includes large-scale pan-India surveys and regional studies. Every aspect of smokeless tobacco, including variations in social, economic, demographic, gender, and education stratifiers, is presented. This evidence-based presentation thereby provides insight not only to assess the burden but can serve as a base, leading to the development and encouragement of research in closing the existing gaps in knowledge. It can also provide a track to formulate tobacco control strategies as well as to reinforce and potentially guide tobacco control policy aimed at addressing the tailored needs in the Indian context. The recommendations expand the tobacco control spectrum and are the first of their kind in the literature to focus on cessation programs as a paramedical subject to draw the attention of not only policymakers but also to integrate medical and dental educational institutions, health care professionals, and tobacco users to synergistically develop successful tobacco control measures.
Introduction
Literature is replete with data that smokeless tobacco (SLT) is the primary etiological factor causing significant morbidity and mortality. 1 Moreover, 30% of the world's population is covered by at least one effective tobacco control measure; 2 even so, tobacco-associated diseases are burgeoning. India is the second highest consumer of tobacco, 3 and despite having adopted and developed tobacco control policies, has one of the highest rates of tobacco-related morbidity and mortality in the world. Illiteracy, poverty, and tobacco use form a vicious cycle, leading to the increase in the number of disease cases. This triad is exacerbated by the failure of tobacco control measures to target specific tobacco habits that are influenced by regional and cultural behaviors and that consequentially burden the handicapped health care system. There are a myriad forms of tobacco consumed, yet tobacco control measures focus primarily upon cigarette smoking and less attention is provided to SLT at all levels of cessation measures. Ironically, however, SLT is the second most common form of tobacco used in India. In this review, an effort has been made to elaborate on regional practices, target groups, and associated mortality in India using data from both large-scale surveys and small research studies. This narrative review is a comprehensive presentation of epidemiological data on SLT use in India, and based on the available information, the gaps in knowledge are discussed; moreover, this review is compiled to be a guide in identifying the lacunae in existing policy measures and includes appropriate recommendations targeted toward decreasing the SLT-associated public health burden.
Terminology
SLT refers to a form of tobacco that is not required to be ignited for use. It is available in various forms, both raw and processed, and is used orally and nasally. Nasal use of tobacco called snuff, although still practiced, is somewhat obsolete and lacks many scientific studies. 4 The term “smokeless tobacco” describes tobacco consumed orally (oral tobacco that can be chewed is mostly described as chewing tobacco), as a quid, sucked, and/or used as a dental and gingival applicant. In this review, smokeless tobacco is abbreviated as “SLT”.
Oral cancer refers to a group of neoplasms affecting any region of the oral cavity, pharyngeal regions, and salivary glands. This term is used interchangeably with oral squamous carcinoma and represents the most frequent of all oral neoplasms. It is estimated that more than 90% of all oral neoplasms are oral squamous cell carcinomas. 5 In this review, the term oral cancer refers to squamous cell carcinoma.
Methodology
This is a narrative review, accomplished by systematic search of the literature digitally. We have reviewed research papers, systematic reviews, and scientific reports about the incidence and prevalence, as well as trends, in SLT use among Indian men, women, youth, children, and other categorizations. Data regarding age, gender, educational status, socioeconomic factors, regional variations, health effects, and tobacco control in India related to SLT use were extracted from multiple surveys. During this process, confounding factors such as smoking and alcohol were avoided to prevent either minimization or exaggeration of facts about SLT. The search terms and sentences used were smokeless tobacco use in India, forms of smokeless tobacco, and smokeless tobacco use under each category–-men, women, school children, teenagers, and pregnant women. Cross-references from primary articles were also searched. In addition, data were derived from related Web sites–-Global Adult Tobacco Survey (GATS) 2010 and the Ministry of Health and Family Welfare, Government of India. Also included are reports from conferences, meetings, and conference presentations.
This review includes data pertaining to the Indian context; however, to compare the variation in toxicity and potential reduced health risks, studies from high-income countries are also included, especially from North America and Europe.
Results
SLT use in India
Oral tobacco is used worldwide. 6 Almost one-fifth of the world's tobacco is consumed as SLT. 7 India is the second highest consumer of tobacco in the world,3,8 and SLT is the dominant form of tobacco used in India: 25.9% of adults use SLT, including 32.9% of males and 18.4% of females.9,10 In some populations, SLT is used by more than 60%. 3 Gender is an important indicator of the form of tobacco consumed. 11
Unlike smoking, smokeless forms of tobacco are consumed by men, women, children, teenagers, and medical and dental students.3,12,13 Most concerning is that street children in India are enticed by the SLT sachets and begin use by as early as 5–10 years of age, and initiation of tobacco use begins by chewing SLT. 14 This leads to early addiction, with approximately 20 million children between 10 years and 14 years of age addicted to tobacco. 14 It is also very common among the scheduled castes. 15 Moreover, children actually are sometimes encouraged to use SLT by parents. 16
Some people, known as polyusers, consume multiple forms of SLT tobacco; these individuals consume, on average, 50% more tobacco than monousers; polyusers are an understudied population. 17 In addition, there is another group of users called dual users, who both smoke and consume SLT; their expenditure on tobacco use is extensive compared to single-form users. 18 Initiation is also associated with psychological and physiological factors, such as tension, indigestion, and constipation. 18
SLT forms
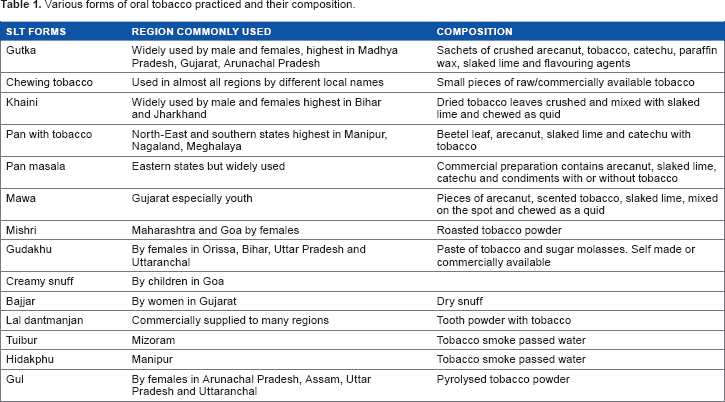
SLT is consumed globally. Unlike in many other countries, in India, tobacco is used in a multitude of forms based on regional practices that are culturally diverse, driven by lifestyle behaviors and unique consumption patterns. The methods of tobacco use include chewing, sucking, and applying/rubbing on gingiva and teeth. 4 This highly addictive substance is used orally in raw/traditional and/or processed forms (Table 1). Gutka, sada, khaini, and beetel quid are chewed either alone or in combination with other products. These are custom prepared by consumers or by pan vendors, in addition to being available prepacked. Pan is a preparation made with beetel leaves, areca nut, and slaked lime with or without tobacco. 4 Pan can be used raw or in combination with commercial preparations such as zarda and kiwam. Various other names for chewing tobacco are manipuri tobacco, mawa, chutki and Tamol, kaddipudi, Guindi, kadapam, and pattiwala.12,15,19 Dentrifices or dental hygiene products such as mishri, gul, bajjar, gudhaku, creamy snuff, and lal dantmanjan are applied on gingiva and teeth.
Various forms of oral tobacco practiced and their composition.
Trends in SLT use
The number of SLT consumers is 163.7 million, and there are 42.3 million dual users.20,21 In India, SLT consumption continues to grow by 2%–3% per annum. 22 Trends in tobacco use are assessed by repeated cross-sectional surveys (National Sample Surveys) carried out across the nation; this allows assessment of type and volume of consumption over a given period of time. However, in these surveys, consumption information is focused on households rather than on individuals, and this presents the possibility of respondent bias. The GATS India report provides information on individual consumption, but as it was conducted only once in India, trends on usage and volume consumed cannot be determined. 23 The male–female gap is less evident in SLT use and is equally high among middle-aged and elderly males and females. 24
The GATS India 2009–2010 survey monitored tobacco use and reported that the most popular form of tobacco among males and females is khaini. 25 Another common form of SLT use that is prevalent throughout India is the chewing of betel quid, a combination of betel leaf, areca nut, and slaked lime with tobacco. Mishri is applied to the gums using a finger, and the habit is generally begun as a dentifrice.
SLT use among youth in India
Age is a crucial factor determining the form of tobacco used. 18 There has been a progressive decline in the age of initiation of tobacco use. Increased use of tobacco among the young is an emerging trend. 26 Younger children are more susceptible than older ones. 27 SLT is the common form of tobacco used by youth; however, its prevalence decreases with increase in age. 18 Commercially available chewing tobacco products such as zarda, gutka, khaini, and mishri are very popular among Indian teenagers and young adults, 28 and gutka is the chewable form that is most commonly used. Socioenvironmental determinants, peer pressure, easy availability, and curiosity have been cited as reasons for initiation among the younger age groups.8,29 Children exposed to Western culture have shown increased risk of tobacco use compared to those exposed only to Indian culture. 30 The behaviors and attitudes of adolescents are also influenced by Bollywood stars.31,32
SLT use among females in India
Increased consumption of SLT by females has been cited as being due to ease of availability and lower cost, as well as social acceptability. 18 Husbands are a crucial influence in enabling women to use SLT. 17 Moreover, women consume SLT even during pregnancy despite knowledge of health risks to the fetus, 3 and there is no difference in consumption patterns between pregnant and nonpregnant women. 17
Studies reporting the prevalence of tobacco use among young and middle-aged females may be an underrepresentation. This can be due to underreporting in the context of societal taboos, especially when individuals are responding in the presence of other members of their family or when the information is provided by the oldest member of the family who may be unaware of their habit or disinclined to admit to their use.
SLT use among school children
A study from the town of Midnapore, West Bengal, India, found that the age of initiation among boys was less than 10 years 33 or even earlier, 19 and this was in the form of SLT. 33 Prevalence of chewing among boys was reported as 48.5%, with 18% applying tobacco orally. Gutka has been the most popular. Exposure to tobacco advertisements has been strongly correlated with tobacco use in children. 27 Adolescents attending school and who were exposed to tobacco promotion activities in Bollywood movies as well as tobacco-branded merchandise were more receptive to tobacco advertising and were two times more likely to have tried tobacco products. Studies have also documented that SLT is advertised by printing their pack shots and brand names on kites that children fly throughout India.31,32 Educational programs for school children have been sponsored by giant tobacco companies. A study from Karnataka has shown that SLT is used by 5.9% of boys and 1.4% among girls aged 13–15 years. The ascending order of prevalence of tobacco use by children, by region, is as follows: rural (3.4%), metropolitan (6.8%), and transitional towns (8.2%). 26 This parallels the exposure to tobacco advertisements. Among this age group, children perceive that tobacco-consuming boys are attractive (69.5%) and have more friends (72.3%). Despite the perception of harm, tobacco use is seen in 4.9% of the children younger than 13–15 years. There is a major lacuna in support from educational institutions for tobacco control, apart from a failure in implementation of legislation and lack of surveillance. 34
Tobacco use among health care students
There is increased use of SLT among medical and dental students despite vast knowledge of its impact on health.12,35 This may be due to onset of nicotine dependence even before students learned about the relationship between SLT and disease. As they are considered role models by patients and their advice on cessation is highly reinforcing, these are important groups to be targeted for future patient care in tobacco control.
Socioeconomic risk factors
Tobacco is used by all socioeconomic groups and the volume of SLT use has increased across all of the socioeconomic groups in the past decade. Income, education, caste, gender, age, and region of residence are risk stratifiers22,36,37 and barriers to penetration of tobacco control policies. SLT is more common among the poorest; the lower the income, the greater is the use of SLT across most of the states.18,37 Exceptions include Andhra Pradesh, Arunachal Pradesh, Kerala, Meghalaya, Mizoram, Nagaland, Sikkim, and Uttarakhand. In Nagaland, however, the rich consume SLT more than the poor. 37 Overall in India, consumption is 3.1 times higher among the poor compared to the rich. 38 Gutka and khaini are the common SLT products available for less than half a rupee. 39 Age appears to be an important indicator of the form of tobacco used; SLT is very common among the young, whereas smoking is more common among the older age groups. 8
SLT use is very common among urban slum dwellers who are a high-risk group for development of tobacco-related diseases. This disease burden is exacerbated by poor health status and inadequate health care.
The prevalence of SLT use is higher among females than among males. 8 Men in urban areas use twice as much as their counterparts in rural areas and women in urban slums use more than women in rural areas. 39 Overall, SLT is very common in urban areas, especially in urban slums, much more than in rural areas. Peer pressure and easy availability are common reasons for initiation of tobacco use.
Illiteracy is a major risk factor associated with both increased tobacco consumption and poly-SLT users. A 50% increase in consumption of tobacco is seen among poly-SLT users compared with mono users. 17 Among the various caste groups, the scheduled tribes show the highest prevalence of chewing tobacco and pan masala, with lower levels of use observed among other backward classes and forward castes. 40 Tobacco use is so well accepted socially among Indian communities that in some marriage celebrations, kiosks are provided that vend SLT for free. Thus, despite awareness of adverse effects, religious prohibitions, and societal taboos, use of SLT continues at a high level.
Geographic variation
The significance of geographic variation needs to be considered in relation to SLT. Though SLT is used throughout India, there are substantial variations in prevalence between states, ranging from 1.6% in Jammu and Kashmir to 59.4% in Mizoram. 37 Chewing tobacco is more common in central, western (except Goa), and northeastern states (Assam, Arunachal Pradesh, Manipur, Meghalaya, Mizoram, Nagaland, and Tripura) compared to other states.19,22 A study from a community-based setting in Delhi found that the prevalence of smoking and SLT use was the same. 18
A study in Mumbai indicated that 56% of women chewed tobacco; of these, 30% used mishri, 32% chewed pan with tobacco, 17% used gul, and 11% initiated SLT as a tobacco dentifrice (SLT is used as a tobacco dentifrice by many children and adults). 17 Gutka is consumed by more than 50% of SLT users. In Gujarat, SLT use was more prevalent among men than among women. Mawa is more popular among youth in Gujarat. 4 SLT use is more common among people aged 25–44 years in Gujarat and Andhra Pradesh. In Andhra Pradesh, the prevalence of SLT use is equal among women and men. 41 The prevalence of tobacco use in Punjab is the lowest, which could be related to the large population of Sikhs (58% of the population), as Sikhism prohibits the use of tobacco. 40 However, a study in Delhi found that Sikhs actually were higher consumers of and spent more money on tobacco. 18
Reasons for increased usage
SLT products account for approximately one-fourth (27%) of the tobacco consumed in India. 42 Reasons for the increased use of SLT in India include extensive antismoking campaigns and increased awareness of the harms of cigarette smoking. Additionally, smoking by women and children is a taboo in most Indian societies 43 and SLT hides tobacco use from bystanders given that it does not require combustion and avoids secondhand smoke. In addition, it is easily available and affordable for all age groups. 44 At least one member in each household has been reported to use SLT. 42 These factors, combined with marketing strategies claiming that SLT is safe, have made these products even more popular and widely used, especially among college students and highly educated people. Low cost and ease of availability have led to use by people of all socioeconomic strata. Easy assimilation of SLT into the culture despite social and religious disapproval has been facilitated by the medicinal properties thought to be associated with it–-that it improves oral health and relieves bowel or abdominal problems. 17 Unrestricted access to tobacco products from stores (irrespective of purchaser age), parental influences, perceived attraction from the opposite gender, and increased exposure to gutka advertisements are all risk factors in facilitating initiation of tobacco use. 19 SLT is so widely available that most residents can obtain it within 10–30 meters of their houses; residential proximity also results in sharing of tobacco practices. 3 Moreover, at work sites, the warnings specifically mention “smoke free” or “no smoking” but do not address the issue of SLT. SLT users have reported that their work premises had no prohibition on tobacco use. 45
Attitude and behavior of SLT users
Users view SLT as a feature of community life in urban slums and use it continuously in spite of it being harmful. 3 A common myth among people who consume SLT is that it causes less harm than smoking and is actually good for their health.6,17 However, there also is recognition of its harmful effects. Parents may spend money on SLT and yet not spend money on sending their children to school. 3
Users commonly feel that gutka refreshes them after hard work. Shared use helps in developing companionship, reduces stress, and suppresses hunger, in addition to being an energy booster during work. 17 People indulge in tobacco use after meals, while resting, and when in a happy mood. 18
SLT users express higher intention to quit when considering personal health and family and are also more receptive to cessation programs, but the quit rates are low. 46
Carcinogenicity of Indian SLT products
SLT is consumed globally; it is called snus in Nordic countries and North America, chimó in Venezuela, nass in Uzbekistan and Kyrgyzstan, tambook in Sudan, and snuff in Nigeria, Ghana, and South Africa. 47 Assessment of toxicity levels in these products shows considerable diversity.
A study of the chemistry of SLT products in India demonstrates high levels of tobacco-specific nitrosamines (TSNAs) and tobacco alkaloids. The tobacco species used for SLT has higher TSNAs than the smoked form.12,28 TSNAs and tobacco alkaloids are strong indicators of the role of SLT in the etiology of cancer. 48 Indian SLT products have high levels of TSNAs, and the greatest amounts are in khaini and zarda. 28 Carcinogenic contents are also present in lal dantmanjans and other dental hygiene products such as Dentobac. The level of the TSNA N′-nitrosonornicotine alone is as high as 76.9 μg/g, whereas the total amount of TSNAs in SLT products marketed in Europe and the USA is less than 10 μg/g. 28 Comparison of the chemical analytes in SLT samples from India in a recent study has revealed that TSNAs and other carcinogens have remained the same as had been found previously. 28 Thus, despite documentation of the direct association of TSNAs with cancer, no efforts have been made to reduce their levels in the newer tobacco products. This is not the case with higher-income countries, eg, Sweden has shown significant reduction in the levels of TSNAs from 1983 to 2002; moreover, moist snuff marketed in Norway, South Africa, Sweden, the USA, and other countries has considerably lower levels of carcinogens. 49
Health effects of SLT
Broader diversity in the toxicity levels of SLT is a deterrent to establishing global risks to human health. 47 The SLT-attributable global disease burden is very high, 85% being due to use in Southeast Asia. 47 In India, the tobacco-caused disease burden is high, 45 and specifically accounts for 74% of the global disease burden. 47 Increased tobacco use has important implications for chronic disease burden as well as for premature death. The lack of effective tobacco control interventions as a primary measure in health care systems leads to the continued increases in disease burden. There are direct and indirect adverse health effects, and the consequences are dose responsive, increasing with the amount of SLT use. SLT when used chronically induces nicotine addiction, 48 oral pigmentation, dental caries, gingival recession, oral mucosal lesions–-tobacco pouch keratosis and potentially malignant lesions–-leukoplakia, erythroplakia, lichenoid reaction, and submucous fibrosis. 50 Tobacco use is a major factor in the etiology of cancer–-oral, 51 pharyngeal, esophageal, and gastric–-and has an important contributory role in cardiovascular diseases, peripheral vascular disease, hypertension, peptic ulcers, and perinatal health, including premature delivery, low birth weight and birth length, as well as fetal morbidity and mortality.6,50,52
Oral lesions
The frequency of consumption and the duration over which SLT is held in the mouth are important risk factors for developing oral lesions. As SLT is predominantly consumed orally, these lesions are very evident.
Oral potentially malignant disorders. SLT-associated oral potentially malignant disorders (OPMDs) include premalignant lesions and conditions; these are leukoplakia, erythroplakia, and submucous fibrosis. India has a high rate of these premalignant lesions. 53 Overall, the prevalence of premalignant lesions in India is 2.5%–8.4%. 53
Leukoplakia is the most common lesion, with a prevalence rate of 0.2%–5.2%. 54 A study from Bangalore has recorded leukoplakia to be prevalent in 14% of the study group, and the malignant transformation rate has been reported to be 0.13%–5.2%. 55 The next most common oral lesion is submucous fibrosis. This is mainly caused by areca nut; as most tobacco users consume commercial preparations that often consist of compounds of areca nut and tobacco, these cannot be isolated. Submucous fibrosis has a malignant rate of 7.6%.
Oral cancer in India
Tobacco quid chewing increases oral cancer risk sixfold. 56 Due to the use of SLT, India has the highest number of oral cancer cases in the world;40,57 30% of all cancers in India are of the oral cancer type,13,58 and in some states, incidence is as high as 10.8 per 100,000. 28 Approximately half of the oral cancer burden is due to SLT; 59 17% of cancers in men and 20% of cancers in women are oral. 60 Crude incidence projections indicate that oral cancer will continue to increase. 58 Despite the role of SLT in the etiology of oral cancer, cessation of SLT use has not received as much attention as cessation of smoking tobacco and, in fact, SLT is promoted as a substitute for smoking tobacco. 61 However, one study failed to find an association between SLT and oral cancer. 62 Studies from Europe and the Americas do not substantiate any association between SLT and oral cancer.47,50 This also is true for esophageal cancer in the USA. 47
Cardiovascular diseases
Though the role of SLT in cancer is well known, its role in cardiovascular diseases is less well understood. 63 India is expected to experience a greater number of cardiovascular deaths than any other country over the next decade. 64
Tobacco control interventions could decrease the death toll by 25%, greater than the reduction achieved by pharmacological strategies. 64
Tuberculosis
Increased frequency of spitting in public places while using SLT poses the threat of transmitting communicable diseases, including tuberculosis (TB). 65 As most TB patients are also tobacco users and quitting tobacco use is synergistic with treatment outcomes, having tobacco cessation clinics at directly observed treatment, short – course (DOTS) centers would have a dual beneficial effect.
Mortality
Increases in the prevalence of SLT use in India have resulted in an increased disease and mortality in the country.1,65 India accounts for one-sixth of tobacco-related illnesses worldwide, and tobacco-related deaths are approximately one million annually. Furthermore, tobacco-related deaths are expected to increase exponentially from 1.4% in 1990 to 13.3% in 2020.31,32 The World Health Organization (WHO) predicts that India will witness the fastest rise in deaths attributable to tobacco in the first 2 decades of the 21st century; most worrisome is the fact that due to increasing tobacco addiction among the youth, much of the rise in tobacco-related mortality will occur in the most productive years of life. 18 To date, tobacco-attributable mortality has been calculated as that generally attributable to cigarette smoking. However, tobacco in all forms adversely affects health, and thus estimates of disease and death from cigarette smoking alone is an underrepresentation of the harm. 66 Although 75% of the Indian population lives in rural areas, cancer-specific mortality rates are assessed from 24 urban cancer registries. 67 A greater number of deaths in India occurs at home without medical intervention and goes unrecorded. The Million Death Study, which is currently in process, has excellent potential to identify the specific causes of death in the Indian population. 67 Moreover, there is an overlap of tobacco use, even among SLT users. Areca nut by itself is carcinogenic; some individuals are dual users; therefore, there is difficulty in obtaining data on mortality from SLT alone. Pan also is carcinogenic; 68 so, mortality specifically related to SLT use in combination with pan is difficult to assess. However, available studies indicate widespread variation in mortality rates among Indian states. In both genders, SLT users suffer a 20% greater risk of death than do nonusers. 4
A study from Mumbai found that the age-adjusted relative risk for men (1096 deaths) was 1.22 and for women (1575 deaths) 1.35. 69 For women, the mortality rates among SLT users were higher in all age groups except the lowest age group (35–39 years). Among men, except in the age range 55–65 years, mortality rates were higher among SLT users. It is therefore highly likely that SLT use causes higher overall mortality.
Rates of tobacco related cancer deaths among men in Assam and other northeastern states were greater than the national rates of death from all cancers. 67 This is consistent with data in this review that SLT use is also higher in these states.
The relative risk of death from SLT use in rural India is 15% for men and 30% for women. 4
Legislation
Multiple attempts at legislation have failed to effectively control or regulate SLT use in India, 65 perhaps due to inadequate implementation. Even the core WHO Framework Convention on Tobacco Control (FCTC) provisions have been poorly implemented, despite India's ratification of the FCTC in 2005. 64 Tobacco control laws prohibit direct, as well as indirect, advertisements of tobacco products and ban sale of tobacco products to minors. However, in a study, one-third of users between 13 years and 15 years of age have reported easy and relatively unrestricted access to tobacco from commercial outlets. 26 Sale of tobacco products is banned within 100 m of educational institutions, but there are a number of outlets in school neighborhoods. Additionally, pan shops and general stores that contribute 90% of SLT outlets are within 100 m of schools.3,26 Tobacco-using medical students have reported that there is no law prohibiting tobacco use on campuses. There is surrogate advertising of tobacco products under the guise of non-tobacco-containing pan masala. 70 Point-of-sale advertisements have mushroomed after the implementation of the 2004 Tobacco Control Legislation. 71 Moreover, shopkeepers are paid for display of tobacco products by the manufacturer or distributor of these products. 71 Policymakers should work toward fuller and faster implementation of the core FCTC provisions to boost their efforts to reduce tobacco-related deaths. To date, tobacco control policies have failed to significantly reduce tobacco consumption. Meaningful reductions in tobacco use are especially challenging given that tobacco consumption is so deeply entrenched.
Advertisement at the point of sale
This requires special attention as the provision for point-of-sale advertisements has distorted India's comprehensive Tobacco Control Act 71 and has served as a method to attract and recruit new users as well as retain current users. There is a causal relationship between tobacco marketing and adolescent tobacco use; students exposed to tobacco advertisements in more than four places are 1.5 times more likely to progress to tobacco usage than unexposed students.31,32 There is a ban on direct advertising of tobacco products in the media or on billboards since May 1, 2004; nevertheless, colorful sachets are displayed abundantly at the point of sale. These colorful hanging sachets are highly appealing and are placed near candies and at a reachable height for children. 71 Points of sale unique to India include pan shops on roadsides and adjacent to or as part of most restaurants (as Indians have the habit of consuming pan and giving priority to tobacco consumption after meals). In general stores SLT is displayed outside along with snacks, houshold groceries. Similarly in tea shops and milk booths. SLT is sold on both community access roads and on main highways. 3 Promotional offers entice shop owners and purchasers with extra packets free with bulk purchases. These offers motivate shopkeepers to attract more users; moreover, selling of tobacco requires no licencing. 3 Children also sell SLT products as a form of income generation. 3
Conclusion
The history and cultural roots of SLT present a difficult set of challenges to India's tobacco control measures.30,72 Moreover, tobacco consumption is expected to continue to increase among both adolescents and adults. 30 Illness due to tobacco use and poverty form a vicious cycle, and continued tobacco use in all sections of society creates a crescendo of disease burden and impedes economic development. The progressive decline in the age of initiation of tobacco use is a matter of significant concern and underscores the need for immediate tobacco control measures. 18 In some countries, supporting SLT use may be considered a harm reduction strategy. 73 Thus, some public health experts in Western countries advocate the use of SLT as a means of tobacco control, specifically as an alternative to cigarette smoking.73,74 However, such an approach is not appropriate for India given the huge health burden of SLT and the fact that the carcinogens present in SLT consumed in India are greater than in those consumed in Europe and North America.
Nationwide multicentric epidemiological research is needed for targeted SLT cessation strategies. Indian SLT users are more receptive to quitting tobacco than are smokers, 46 with a success rate highest among the elderly (who are, ironically, less likely to receive cessation services). 36 The government should tap into this attitude to bring about increased cessation activities, because quitting at any age is beneficial. 46 Currently, there are only 19 tobacco cessation clinics in the entire country, and for these clinics to support 275 million tobacco users is clearly not possible. 75
Gender-sensitive individual- and community-specific interventions can reduce the prevalence and negative effects of tobacco use. 15
Tobacco control policies in India have focused on health awareness and behavior change, but population-level interventions–-such as increased taxation and taxing of SLT on a par with smoking tobacco–-have not been adequately considered. 76 India should take lessons from Bhutan, where the production of tobacco and the manufacture of tobacco products have been completely banned since 2005, if there is serious political will to extinguish tobacco and decrease the disease burden in this country.
Although the harmful effects of SLT are evident, epidemiological and demographic studies of adult mortality at subnational levels in India remain scarce. Further reliable evidence of the levels, variation, and trends in adult mortality in India's districts can promote adoption of evidence-based policies. 77
Recommendations
Based on the available data, the following actions are recommended, envisaging reduction in tobacco use in the near future.
Studies are needed that focus exclusively on populations of women surveyed away from their residence, such as workplaces and colleges, to prevent underreporting.
Surveillance of implementation and enforcement of existing policies should be conducted periodically, especially tobacco sales and purchases by children.
Ban point-of-sale advertisements.
Tobacco cessation should be included as a primary health care service. Tailored quitting programs that are culturally oriented should be developed to increase the effective penetration of tobacco control policies.
Tobacco control programs and cessation services should be made a paramedical subject to entice and engage more health care professionals.
It should be mandatory to screen and counsel women as part of maternity examinations and to follow up in order to prevent fetal morbidity and mortality associated with maternal tobacco use.
Educational institutions must be mandated to actively participate in creating awareness of the ill effects of tobacco consumption, in addition to conducting surveillance to prevent new recruits and to encourage current users to quit. Such initiatives will continue to be a sustainable source for prevention of early initiation.
Footnotes
Author Contributions
Wrote the first draft of the manuscript: PM. Contributed to the writing of the manuscript: PM and HAL. Agree with manuscript results and conclusions: PM and HAL. Jointly developed the structure and arguments for the paper: PM and HAL. Made critical revisions and approved final version: PM and HAL. All authors reviewed and approved of the final manuscript: PM and HAL.