
Abstract
Aim
This study was designed to determine if there is a relationship between celiac disease (CD) and the presence of gastrointestinal disease (GI) disease in children with autism.
Subjects and Methods
One hundred twenty-two children were tested for IgG and IgA anti-transglutaminase autoantibodies (55 autistic children with GI disease, 28 non autistic children with no GI disease, 30 autistic children with no GI disease, and 9 non autistic children with GI Disease). We also compared the presence/level of these autoantibodies to presence of anti-neutrophil cytoplasmic antibodies (ANCA) and level of Alpha-1 Antitrypsin (AAT).
Results
We did not find a significant difference in the level of anti-transglutaminase IgG or IgA in autistic children with GI disease compared to controls. However, we found a significant relationship between the presence of ANCA and low-level IgG anti-transglutaminase IgG in children with autism and GI disease.
Discussion
Although there appears to be no relationship between these celiac disease markers and the presence of GI disease in autistic children, these results suggest a possible association between sub diagnostic levels of anti-transglutaminase IgG and the presence of ANCA, and therefore, supports the hypothesis that there is a generalized autoimmune dysfunction in autistic children with GI disease.
Introduction
Autism is a complex, behaviorally defined neurodevelopmental disorder characterized by social deficits, language impairments, and repetitive behaviors. There has been a dramatic increase in the diagnosis of autism over the past decade. 1
Celiac disease is an inherited autoimmune disorder affecting the gastrointestinal tract. It is caused by a modification of gliadin, a gluten protein, by tissue transglutaminase. Causing an immune response and inflammation. 2
The incidence of Celiac disease in newborns may be as high as 1 in 100 births.3–5 However, the incidence of CD in children with other autoimmune disorders may be as high as 1 in 12. 6 It might also be expected that a higher incidence of CD would be found in children with existing GI disease.
There is conflicting evidence to support whether there is a relationship between CD and autism.7,8 Recently, however, Atladóttir et al, reported a significant association between maternal history of celiac disease and autism, suggesting a possible genetic link between the two disorders. 9
Research also suggests that low levels of AAT (AAT deficiency) may be associated with the etiology of Celiac disease (CD).10–17 We previously reported that a significant number of autistic family members had lower than normal serum levels of alpha-1 antitrypsin (AAT). 18
ANCAs are directed against several myeloid enzymes. By indirect immunofluorescence microscopy on neutrophils, two major categories can be distinguished: cytoplasmic ANCA and perinuclear ANCA. By ELISA testing, cytoplasmic ANCA nearly always reacts with proteinase 3 (ANCA-PR3). The major perinuclear ANCA target is myeloperoxidase (ANCA-MPO). 19
Our lab has reported that a significant number of autistic children with GI disease have anti neutrophil cytoplasmic antibodies (ANCA), both anti-PR3 and anti-MPO. We have also reported that there is a relationship between individuals with ANCA and severity of gastrointestinal disease, 19 and that low serum AAT, anti-PR3 ANCA and high serum PR3 also correlate with severity of GI disease. 20 This suggests that low AAT levels may result in high levels of PR3, 21 which may, in turn, be associated with the formation of ANCA and ultimately be related to the etiology of CD.
This study was designed to determine if there is a relationship between CD and autism in autistic children with GI disease, and, if so, determine if the presence of CD biomarkers correlates with low levels of AAT and/or ANCA(s).
There is evidence to suggest that anti-transglutaminase screening (using the IgA+/-IgG isotype) is the most sensitive and specific serological assessment of CD.22,23 We chose to use these autoantibodies as the biomarker for CD in these experiments.
Materials and Methods
Subjects
The diagnosis of autism for all subjects in this study was made using the standard Autism Diagnostic Interview-Revised (ADI-R) algorithm, and ASSQ assessment was used to exclude autism in controls.
GI pathology was determined through medical history data and, in the case of those with GI disease, through endoscopic diagnosis.
Experimental
Serum from autistic individuals with GI disease (n = 55) was obtained from the Thoughtful House,** Austin, Texas and the Autism Genetic Resource Exchange (AGRE).* All of these children (median age 6.2 years; range 2–16) had chronic digestive disease. The individuals from whom serum samples were collected from the Thoughtful House were characterized with ileo-colonic lymphoid nodular hyperplasia (LNH) and inflammation of the colorectum, small bowel and/or stomach (identified by endoscopy).
The Thoughtful House is a comprehensive treatment and research center, specializing in the care of children with neurological disorders, including autism.
The Autism Genetic Resource Exchange (AGRE) is is a collaborative gene bank for the study of autism spectrum disorders currently founded by the National Institute of Mental Health and Autism Speaks.
The 27 autistic children with GI diseae tested for AAT, ANCA and PR3 were chosen randomly as the first 27 received.
Controls
Three control groups (n = 67; median age 6.4 years; range 3–18) were studied–-including 28 non autistic children with no GI disease, 30 autistic children with no GI disease, and 9 non autistic children with GI Disease. Serum and medical history of controls were obtained from AGRE. The 9 non autistic children with GI Disease represent all the serums in this category available from AGRE.
Serums
Experimental (Thoughtful House) and control (AGRE) serums were all morning draws and then treated in an identical fashion–-frozen at -70 C immediately after collection. Cells were separated from serum by centrifugation, then stored at -70 C until thawed for use in ELISAs.
Elisas
Each sample was tested with a minimum of three replicate well in each ELISA and assays were repeated a minimum of two times.
ELISAs to measure serum anti-transglutaminase IgG and IgA (Immco Diagnostics, Buffalo, NY; Catalogue numbers 1144G and 1144, respectively).
A 1:51 dilution of the patient samples were prepared by mixing 10 µl of the patient sera with 0.5 ml of Serum Diluent. 100 µl of Ready to Use Calibrators, Positive and Negative controls and diluted patient samples were added to the appropriate microwells. Plate was incubated 60 minutes (±5 min) at room temperature, then washed 4X with wash buffer. 100 µl of Conjugate was added to microwells. The plate was incubated for 30 minutes (±5 min) at room temperature, then washed 4X. 100 µl of Enzyme Substrate was added to each microwell in the same order and timing as for the Conjugate. The plate was incubated 30 minutes (±5 min) at room temperature, then 100 µl of Stop Solution was added to each microwell using the same order and timing as for the addition of the Enzyme Substrate. The absorbance was read at 405 nm using an ELISA Reader (Biorad, CA).
ELISAs to measure AAT, PR3, ANCA, (anti-transglutaminase IgG and IgA (Immco Diagnostics, Buffalo, NY; Catalogue numbers 1144G and 1144, respectively) were previously described (18, 19, 20–-respectively).
Statistical Analysis
Inferential statistics were derived from t-test and odds ratios with 95% confidence intervals. ANOVA analysis was used to do an analysis of variance and multiple comparisons.
Results
Two autistic children with GI disease (total n = 55) had a diagnostic level of IgA anti-glutaminase for Celiac disease. One of the controls (total n = 67) (non autistic with GI disease) also had a diagnostic level of IgA anti-glutaminase.
Fourteen autistic children with GI disease (total n = 55) had diagnostic levels of IgG anti-glutaminase. However, thirteen controls (n = 67) also had diagnostic levels of IgG anti-glutaminase (seven non autistic children with no GI disease, 5 autistic children with no GI disease and 1 non autistic with GI disease).
We analyzed levels of AAT, PR3 and ANCA concentration/presence in 27 of the 55 autistic children with GI disease, as well as 15 non autistic controls, and found a significant relationship between IgG anti-glutaminase autoantibodies (measured in enzyme units (EU)) and the presence of ANCA (individuals with both MPO and PR3 ANCA (P = 0.0016 t test) and individuals with only MPO ANCA (P = 0.0056 t test) (Table 1); ANOVA analysis (P = 0.002) (Fig. 1) in the autistic group, but not in the control group. All individuals with PR3 also had MPO antibodies. We did not find a significant relationship between these CD markers and AAT or PR3 concentrations (ANOVA P = 0.467) (Fig. 2).
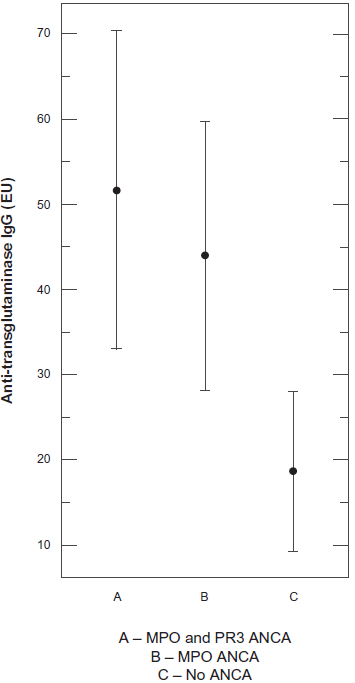
Association between celiac disease marker and ANCA in autistic children with GI disease.
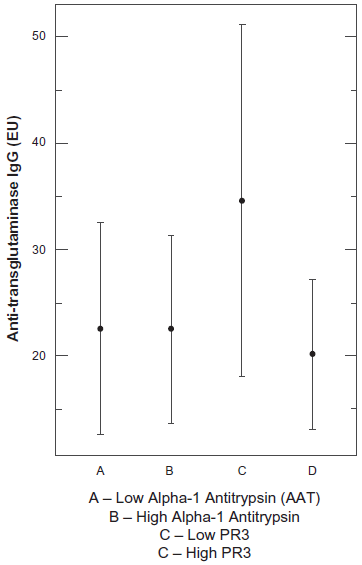
No association between CD marker and AAT and PR3.
Significant difference between anti-transglutaminase IgG concentration (EU) levels and ANCA (PR3 and MPO; and MPO alone) in children with autism.

The two-tailed P value equals 0.0016.
The two-tailed P value equals 0.0056.
Discussion
This preliminary study was designed to determine whether CD is associated with autism, particularly in children with both autism and GI disease. It also attempted to demonstrate whether AAT deficiency and/or the presence of ANCA is associated with anti-transglutaminase autoantibodies.
Our study supports a recent study at Tehran University of Medical Sciences, where 34 autistic children and controls were screened for anti-gliadin autoantibodies. 24 Four autistic children and two controls were positive and the authors concluded that there was no significant difference between the groups. In contrast, Barcia et al, at The University of Brussels in 2008, 18 retrospectively evaluated 150 autistic subjects (123 males, 27 females; mean age 6 years 8 months). Five subjects (3.3%) were diagnosed with CD, which was significantly higher (P = 0.014) than CD prevalence for the general pediatric population.
There have been several reports of immune dysfunction in autistic children with GI disease.25–32 Immune dysfunction has been reported in autistic children, including autoimmunity to central nervous system (CNS) proteins.33–35 This has led to speculation that exposure of the developing neuronal system during critical periods of aberrant immune activation may result in the brain pathology of ASD. Neuroactive compounds, that share immunomodulatory properties, have been implicated in the disease process. For example, elevated platelet serotonin levels are observed in approximately one third of children with autism.36–38 Analysis of data from small but representative groups of ASD patients has shown that approximately 30%–70% of autistic patients have circulating anti-brain autoantibodies, including autoantibodies to a serotonin receptor, 39 myelin basic protein 40 and unknown antigens from adult brain tissue extract. 41
Separate epidemiologic studies suggest that a family history of autoimmune disorders is more common in children with autism compared to healthy control children.42,43 There is also increased incidence of asthma, allergy, autoimmune psoriasis and Type I diabetes in mothers of children with ASD, 44 and first degree relatives of children with autism and Aspergers are more likely to have an autoimmune disease compared to controls.45,46
The results of our study indicate that there is no significant difference in levels of IgA and IgG anti-transglutaminase autoantibody between children with and without autism, including the sub population of autistic children with GI disease. We did not find a relationship between AAT deficiency and anti-transglutaminase autoantibodies.
Interestingly, however, we found that a significant number of children, both autistic and non autistic have clinically significant levels of IgG anti-transglutaminase autoantibody, and, in the autistic group, there is a significant relationship between the presence of ANCA and IgG anti-glutaminase autoantibodies.
We previously reported that a sub population of autistic children with GI disease has generalized autoimmune disease. 47 The results presented here support the premise that immune dysfunction in these individuals may be generalized (multiple autoantibodies). This may explain why general immune suppression, such as the use of steroids and other anti-inflammatory drugs, can be successful treatment for some autistic children with GI related illness.
Disclosures
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers of this paper report no conflicts of interest. The author confirms that he has permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
I'd like to thank Scott Filer, Executive Director, and Allen Lewis, Medical Director of The Pfeiffer Treatment Center for their support and help in this research and manuscript preparation.
I'd also like to thanks Laurie Myers and Kyle Andrews for their technical assistance.
Supported by a Grant from The Autism Research Institute.