
Abstract
Aim
To assess both ant-PR3 and anti-MPO IgG anti-neutrophil cytoplasmic antibodies (ANCA), in autistic children with gastrointestinal symptoms and controls, and to test the hypothesis that there is an association between the presence of these antibodies and inflammatory GI disease seen in many autistic children.
Subjects and Methods
ELISA's were used to measure anti-PR3 and anti-MPO IgG in 40 autistic children with chronic digestive disease (many with ileo-colonic lymphoid nodular hyperplasia (LNH) and inflammation of the colorectum, small bowel and/or stomach), and 41 controls (21 age matched autistic children with no GI disease and 20 age matched children without autism or GI disease).
Results
Six of 40 autistic children with chronic digestive disease had anti-PR3 antibodies compared to none of the 41 controls (p <0.01). Thirteen of the 40 autistic children with chronic digestive disease had anti-MPO IgG compared to only 3 (1 autistic control with no GI disease and 2 non-autistic controls without GI disease) of 41 controls (p <0.001). All six of those with anti-PR3 IgG also had anti-MPO antibodies. These results suggest a relationship between individuals with ANCA and severity of intestinal disease in a subset.
Discussion
These results suggest an association between anti-PR3 and anti-MPO antibodies and a subset of ASD children with GI inflammation.
Keywords
Introduction
The autoantibodies, ANCA (anti-neutrophil cytoplasmic antibodies), were originally detected in serum from patients with Wegener's granulomatosis (WG), 1 a disease characterized by necrotizing granulomatous inflammation of the upper and lower airways in conjunction with systemic vasculitis and necrotizing crescentic glomerulonephritis. Samples from patients with WG reveal a typical cytoplasmic staining pattern against the antigen proteinase 3 (PR3), a constituent of the azurophilic granules of the neutrophil (c-ANCA). 2
A second type of ANCA, detected in several other idiopathic forms of systemic vasculitis and glomerulonephritis, 3 is characterized by a perinuclear staining pattern on ethanol-fixed neutrophils (perinuclear or p-ANCA antibodies). The first antigen recognized by these p-ANCA was identified as myeloperoxidase (MPO), another constituent of the azurophilic granules. 4 The perinuclear staining proved an artifact caused by ethanol fixation. MPO, a highly cationic protein, apparently moves and attaches to the negatively charged nuclear membrane during the fixation procedure. 5
Following the detection of ANCA in systemic vasculitis, it became clear that ANCA also occur in other idiopathic inflammatory disorders. 6 ANCA have been detected in the inflammatory bowel diseases or IBD (which include ulcerative colitis (UC) and Crohn's disease (CD),7,8 in autoimmune-mediated liver diseases, 9 11 in rheumatoid arthritis (RA),12,13 and in systemic lupus eythematosus (SLE).14,15 A third type of ANCA, producing a diffuse cytoplasmic staining on ethanol-fixed neutrophils (atypical ANCA or a-ANCA), has also been described in these diseases. 16
IBD (UC and CD) are chronic, tissue-destructive idiopathic inflammatory conditions limited to the large bowel (UC) or occurring anywhere along the alimentary tract (CD). The etiology of these diseases has not yet been fully elucidated. 17 However, autoimmune processes may play a role in their pathogenesis, since several types of autoantibodies have been found in these diseases, such as antibodies to goblet cells, 18 antibodies to the cytoskeletal protein tropomyosin, 19 and antibodies to endothelial cell antigens. 20
In 1990, two different groups reported the presence of ANCA in serum from 84% and 59% of patients with UC, respectively.7,8 Since then, numerous reports have confirmed this finding. ANCA were also detected in CD, although the prevalence (10%–20%) in this disease is much lower than in UC (50%–90%),7,8 and in primary sclerosing cholangitis (50%–85%), a chronic cholestatic liver disease that is strongly associated with IBD.9,11,21
Because ANCA have been shown to be associated with inflammation of the bowel and rest of the alimentary canal, and many autistic children may have GI disease related to inflammation, we used ELISAs to measure the levels of anti-PR3 and anti-MPO ANCA in 40 autistic children with chronic digestive disease (most with ileo-colonic lymphoid nodular hyperplasia (LNH) and inflammation of the colorectum, small bowel and/or stomach), and compared the results to ANCA in 41 controls (21 age, gender and diagnosis matched autistic children with no GI disease and 20 age and gender matched children without autism or GI disease).
Materials and Methods
ELISA to measure anti-PR3 antibodies and anti-MPO antibodies (IMMCO Diagnostics, Buffalo, N.Y.)
All reagents and specimens were equilibrated to room temperature before the assay was performed as instructed. Patient and control sera (diluted 1:50 with serum diluent) and calibrators (prediluted 20–200 Eu/ml) were added to microculture wells containing PR3 or MPO antigen, then incubated for 30 minutes (±5 min) at room temperature. Wells were washed 4 times, then pre-diluted anti-human IgG conjugated with alkaline phosphatase was added to each well. Wells were incubated again for 30 minutes at room temperature, then washed 4 times. One hundred microliters of enzyme substrate were added to each well. Color change was read at 405 nm with an ELISA reader after 30 minutes at room temperature. Serums were determined to be positive for ANCA if greater than 20 eu/ml when compared to calibrators (IMMCO).
Subjects
Autistic Children with GI Disease
Serum from autistic individuals with GI disease was obtained from the Thoughtful House, Austin, Texas. These patients ranged in age from 2 to 16 years with a median age of 71 months, thirty-four (85%) were male. Most patients were referred by their primary care physician for evaluation of ongoing gastrointestinal symptoms, while some patients were parent-referred.
All patients had a diagnosis of autism, autistic spectrum disorder, pervasive developmental disorder (PDD) or Asperger's syndrome. The developmental diagnosis was established by either single or multiple members of the following specialties: pediatric neurologists, developmental pediatricians, pediatric psychiatrists, or psychologists. A clear history relating to the onset of developmental disorder was obtained from the parents of all 40 patients. Of these, the large majority (65%) was reported to have had a regressive onset. Regression was determined as a normal development until at least age 12 months followed by inexplicable loss of previously achieved developmental milestones between 12 and 24 months and accompanied by the appearance of typical autistic behaviors or normal development until at least age 12 months followed by a developmental plateau in which milestones are not noticeably lost but the rate of development suffers marked deceleration, accompanied by the appearance of typical autistic behaviors. Non regression individuals had definite onset of autistic behaviors prior to age 12 months.
Scoring of Severity of GI Disease
All the children in our study (40) had chronic gastrointestinal symptoms and all were investigated by ileo-colonoscopy. Macroscopic and histological features of the upper and lower GI tract were scored. A point system was developed to assess the severity of GI disease (particularly inflammation). Patients were scored according to mild (1 point), moderate (2 points) and marked (3 points) disease in each area (upper and lower GI) and for endoscopic assessment (macroscopic) and histological assessment of each area. Therefore, the maximum score for GI disease was be 12 (3 points each for upper scope, upper histology, lower scope and lower histology). A point system was also developed for severity of lymphoid nodular hyperplasia (LNH). Patients were scored according to mild (1 point), moderate (2 points) and marked (3 points) LNH in each area (upper and lower GI) for a maximum of 6 points. And finally, a point system was also developed for severity of erythema. Patients were scored according to mild (1 point), moderate (2 points) and marked (3 points) erythema in each area (upper and lower GI) for a maximum of 6 points (Table 2).
Controls
Two control groups (total n = 41) were studied, including 21 age (mean 68 months), gender (80% male) and diagnosis (61% regressive onset) matched autistic children with no GI disease and 20 age (mean 71 months) and gender (75% male) matched children without autism or GI disease. Serum and medical history were obtained from the Autism Genetic Resource Exchange—AGRE.
Statistics
Inferential statistics were derived from t-test and odds ratios with 95% confidence intervals.
Results
Results and specificity of a typical anti-PR3/anti-MPO ELISA are shown in Figure 1. All data represents mean +/- SD of two separate assays with multiple wells tested in each assay. In total, 6 of 40 autistic children with chronic digestive disease had anti-PR3 antibodies compared to none of the 40 controls (p <0.01). Thirteen of the 40 autistic children with chronic digestive disease had anti-MPO IgG compared to only 3 of 41 controls (p <0.001) (Fig. 2). All six of those with anti-PR3 IgG also had anti-MPO IgG (p <0.01) (Table 1).
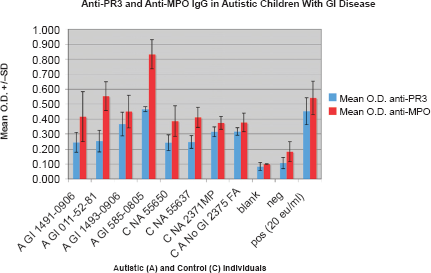
Results of a typical ELISA measuring the presence of anti-MPO IgG in an autistic (A) child with GI disease (GI), A GI 011-52-81, and both anti-MPO and anti-PR3 IgG in an autistic (A) child with GI disease (GI), A GI 585–0805. None of the controls (C NA – non autistic; C A—autistic without GI disease) have anti PR3 or anti-MPO antibodies.
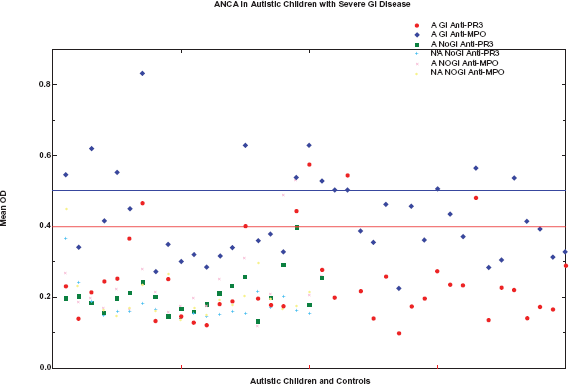
Forty autistic children with severe GI disease (A-GI) and 41 controls (21 age matched autistic children with no GI disease and 20 age matched children without autism or GI disease) were tested for anti-PR3 and anti-MPO IgG. Six A-GI had anti-PR3 IgG (greater than 20 Eu/ml, above 0.4 OD —); 13 A-GI had anti-MPO IgG (greater than 20 Eu/ml, above 0.5 OD —). Whereas none of the controls had anti-PR3 IgG and only 3 had anti-MPO IgG.
Presence of ANCA correlates with severity of GI disease. Fourteen of the 40 autistic children with GI disease were categorized as having severe GI disease (score equal or greater than 7-bold), 6 of 40 had severe LNH (score equal or greater than 4), and 5 of 40 had severe erythema. Of those individuals with anti-MPO IgG (n = 13 out of 40-bold), 7 had a total GI severity score greater than 7 (p <0.05). Five (of 6) of the individuals with anti-PR3 IgG had severe Total GI disease (p <0.01). Three (of 6) of the children with severe LNH also had both ant-PR3 and anti-MPO IgG (p <0.05), and 4 (of 5) children with severe erythema had either anti-MPO IgG (n = 1) or both anti-PR3 and anti-MPO IgG (n = 3) (p <0.05). (Diagnosis: A-autistic early onset, RA-regressive onset, ASP-Asperger's, PDD-pervasive developmental disorder).
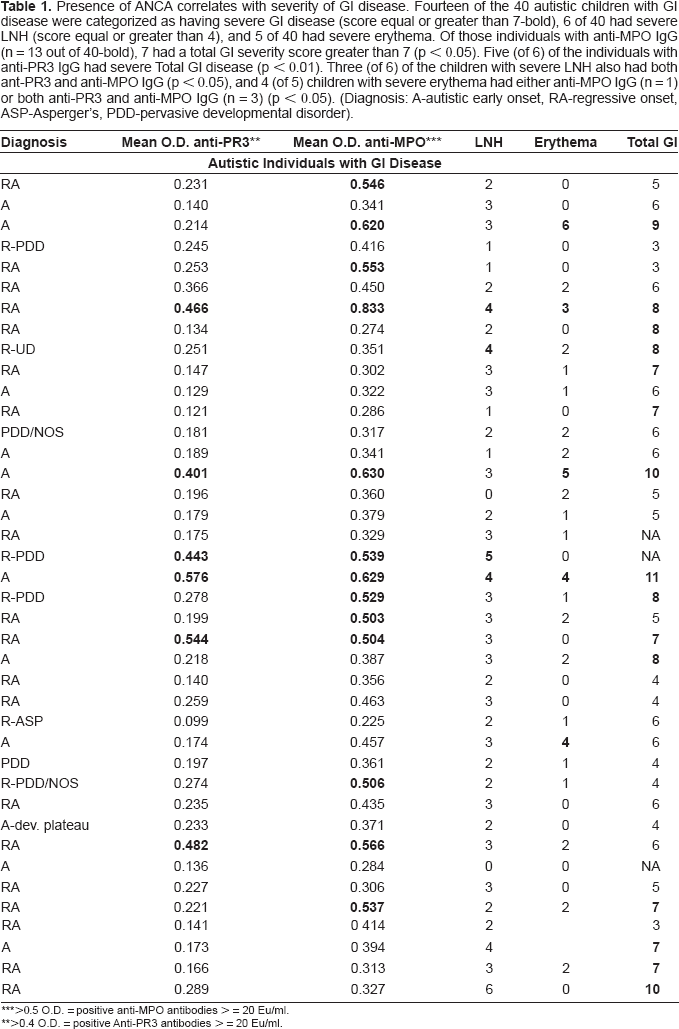
>0.5 O.D. = positive anti-MPO antibodies > = 20 Eu/ml.
>0.4 O.D. = positive Anti-PR3 antibodies > = 20 Eu/ml.
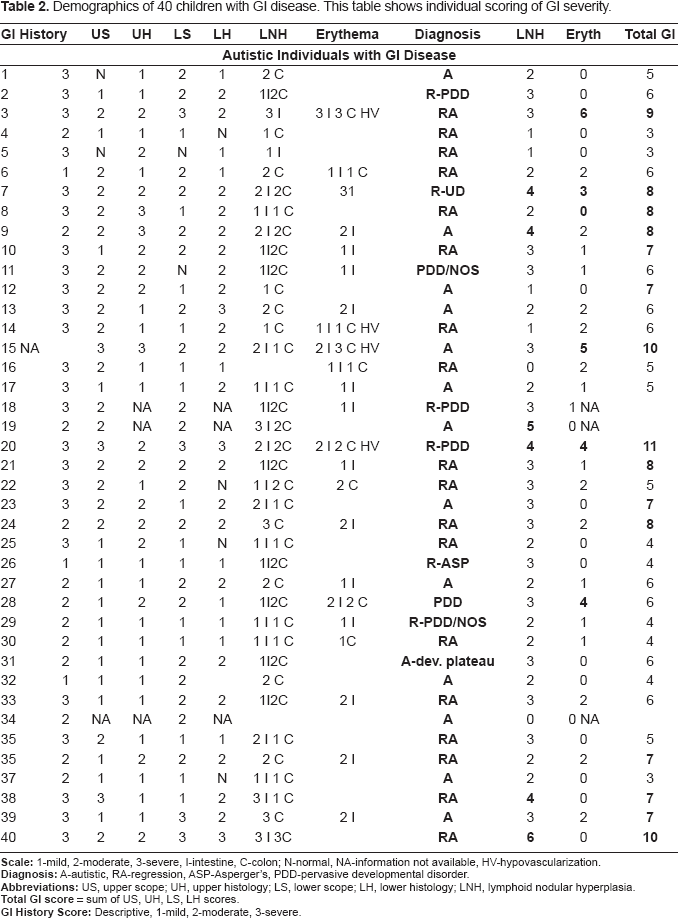
Demographics of 40 children with GI disease. This table shows individual scoring of GI severity.
There was a significant relationship between individuals with ANCA and severity of disease, particularly the presence and severity of LNH and abnormal vascularization. Fourteen of the 40 autistic children with GI disease were categorized as having severe disease (score equal or greater than 7 on total GI severity score described above), 6 of 40 had severe LNH (score equal or greater than 4), and 5 of 40 had severe erythema (Table 1). Of those individuals with anti-MPO IgG (n = 13 out of 40), 7 had a total GI severity score greater than 7 (p <0.05). Five (of 6) of the individuals with anti-PR3 IgG had severe Total GI disease (p <0.01) (Table 1). Although presence of anti-PR3 and anti-MPO is generally found in autistic children with higher GI severity scores, some autistic children with higher scores are negative for ANCA.
Three (of 6) of the children with severe LNH also had both ant-PR3 and anti-MPO IgG (p <0.05), and 4 (of 5) children with severe erythema had either anti-MPO IgG (n = 1) or both anti-PR3 and anti-MPO IgG (n = 3) (p <0.05) (Table 1).
Discussion
We used an ELISA to measure anti-PR3 and anti-MPO ANCA in a group of 40 autistic individuals who presented with GI symptoms and mucosal inflammation, and 41 controls (21 age, gender and diagnosis matched autistic children with no GI disease and 20 age and gender matched children without autism or GI disease). Of the autistic children with autism, all were reported to have chronic GI disease.
This study shows that ANCA (anti-MPO or both anti-PR3 and anti-MPO) are found in a significant number of autistic children with chronic digestive disease and that a significant relationship exists between individuals with ANCA and the severity of their GI disease (including LNH and mucosal erythema). We found that some autistic children with higher GI severity scores were negative for ANCA. Overall, these results suggest a relationship between anti-PR3 and anti-MPO antibodies and GI inflammation seen in at least a subset of individuals with ASD.
D'Eufemia and colleagues identified abnormal intestinal permeability, a feature of small intestinal enteropathy, in 43% of a group of autistic children with no gastrointestinal symptoms, but not in matched controls. 22 Some have also found a relationship between chronic enterocolitis and regressive developmental disorder. 23 Wakefield et al. have established that ileo-colonic lymphoid nodular hyperplasia (LNH) was found in higher prevalence in children with ASD and gastrointestinal symptoms, and is associated with mucosal inflammation. 25 These studies and evidence of anemia and immune deficiency in some autistic children, suggest an association between intestinal dysfunction and autism spectrum disorders (ASD). However, increased incidence of gastrointestinal problems in autistic children is still under study because the exact relationship between GI symptoms and ASD is unclear. 24
It is not surprising that ANCA are present in some autistic children. These autoantibodies are present in individuals with a number of autoimmune related diseases and immune aberrations consistent with a dysregulated immune response. Although Immunological abnormalities found in autistic children appear to vary in the studies, perhaps partly reflecting heterogeneity of the study subjects, immune dysfunction, including abnormal T helper cell type 1 cytokine profiles, decreased lymphocyte numbers, decreased T cell mitogen response, and the imbalance of serum immunoglobulin levels26,27 has also been found in many autistic children. In addition, autism has been linked with autoimmunity, including antibodies to human leukocyte antigen (HLA)-DRB1 and complement C4 alleles,26,27 and recently antibody to brain-specific antigens. 28 T lymphocyte cytokine profiles in the intestinal mucosa of children presenting with regressive autism and intestinal symptoms show a marked skewing towards a pro-inflammatory profile with an excess of TNFα and a deficiency of regulatory IL-10.29,30
The potential role of ANCA in autism is unknown, and even the role of ANCA in IBD and UC and other GI disorders, is not completely understood. However, this study suggests these autoantibodies are associated with inflammation (particularly LNH) and erythema found in a subpopulation of autistic children with GI inflammation-associated disease.
This suggests that the detection of ANCA in autistic children could lead to earlier and better treatment of ASD children with GI disease, and, although, at present, it is unclear whether ANCA are associated with the cause of GI disease or present because of pre-existing inflammatory factors, the understanding of why ANCA are present could also lead to new and better ways of diagnosing and treating GI problems seen in many autistic children.
Disclosure
The authors report no conflicts of interest.