
Abstract
Objectives
To report a case in where a mural endocarditis caused by Candida parapsilosis was successfully treated with the combination of 2 antifungal agents, caspofungin and voriconazole, in an extremely premature infant.
Description
A female infant born at 30.7 weeks with weight 925 g. The infant had a pneumothorax and respiratory distress syndrome, requiring prolonged mechanical ventilation, 1 venous umbilical and 3 central catheters, and broad-spectrum antibiotics. At 51 days of life, an echocardiogram showed an image compatible with fungal vegetation on the junction of the superior vena cava to the right atrium. Blood cultures grew Candida parapsilosis in various sequential samples, despite treatment with fluconazole and amphotericin-B and in vitro sensitivity to these drugs. A treatment of combined voriconazole and caspofungin was initiated resulting in clinical improvement and no need for surgical removal of vegetation.
Comments
Combined therapy with newer antifungal agents can be life-saving in premature infants with Candida parapsilosis complicated sepsis.
Introduction
In the premature newborn, invasive fungal infections are the second leading cause of morbidity and mortality. During the past decade, the incidence of Candida infections has dramatically increased, especially in very low birth weight (VLBW) infants. The smaller the birth weight the greater the chance of developing a Candida infection. Candida albicans and Candida parapsilosis are the most frequently isolated species. The primary risk factors are low birth weight, use of central venous catheters (CVC), prolonged mechanical ventilation, parenteral nutrition with lipid solutions, use of broad spectrum antibiotics, steroids and previous fungal colonization.1,2,3,4 Candida parapsilosis has been responsible for one quarter of all cases of invasive fungal infections in VLBW. Previous studies have suggested that C parapsilosis is more likely to be tolerant to amphotericin B.5,6,7
We report the case of a VLBW premature infant with an invasive infection caused by Candida parapsilosis, isolated from repeated blood cultures, and complicated by endocarditis. There was no response to the usual drugs; however the infection was successfully treated with a combination of caspofungin and voriconazole.
Case Report
Cultures, antibiotics, antifungal agents and clinical/laboratory data.
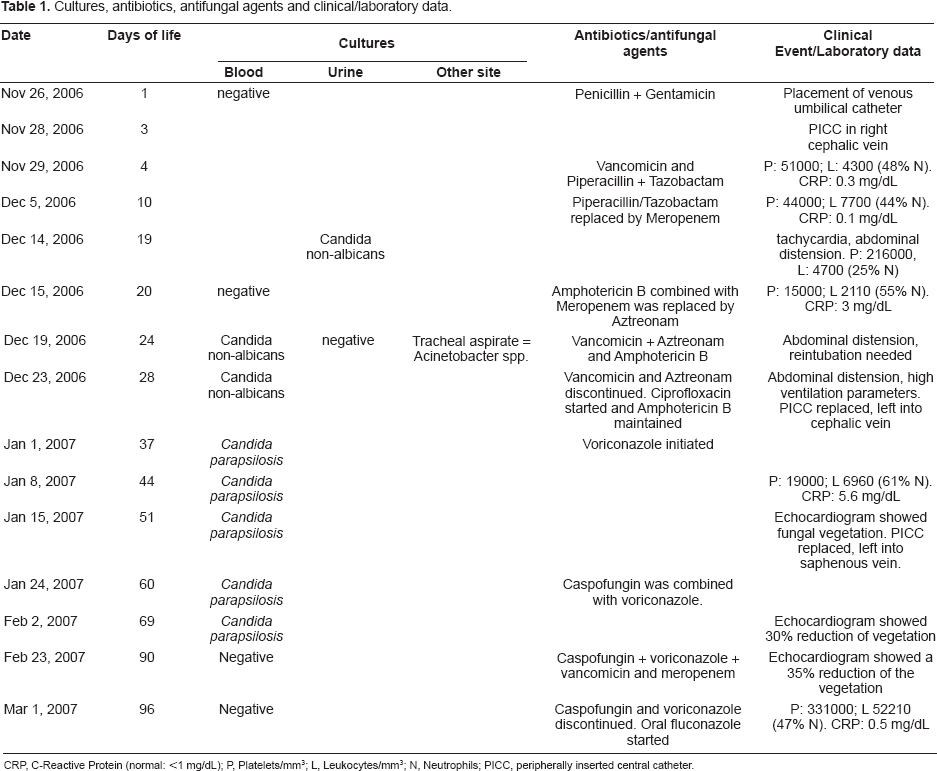
CRP, C-Reactive Protein (normal: < mg/dL); P, Platelets/mm3; L, Leukocytes/mm3; N, Neutrophils; PICC, peripherally inserted central catheter.
With 4 days of life, a low platelet count was noted, and the antibiotics were changed. Parenteral nutrition was initiated after 5 days. At 20 days of life, platelets and leukocyte counts were noted to be decreasing, C-reactive protein levels were elevated, and the baby presented with apnea, generalized edema and abdominal distension. Empiric intravenous amphotericin B was started (1 mg/kg/24 h). A urine culture was obtained at 19 days of life which was positive for Candida non-albicans. She was reintubated on day 22. A blood culture obtained at 24 days of life also grew Candida non-albicans, and intravenous fluconazole was added (loading dose 10 mg/kg/24 h then 6 mg/Kg/24 h). Abdominal ultrasound showed ascitic fluid, and a posterior culture of this fluid proved negative. Urine cultures were negative, but laboratory tests continued to show low platelet counts and leucopenia. At 37 days of life, we were able to identify the blood isolates as Candida parapsilosis, sensitive in vitro to fluconazole (E-Test: 1.5 µg/mL), voriconazole (E-Test: 0.012 µg/mL) and amphotericin (E-Test: 0.38 µg/mL). The E-Test for caspofungin was not available at this time. At 51 days of life, an echocardiogram showed an image compatible with fungal vegetation on the junction of the superior vena cava to the right atrium (Fig. 1). Because of the baby's weight and clinical conditions, surgical removal of the cardiac vegetation was not possible. A new catheter was placed, and at 60 days we decided to add caspofungin 50 mg/m2/24 h to the intravenous voriconazole (12 mg/kg/24 h). Two days after the onset of this treatment, the child had improved and was able to be fed enterally, and extubation was possible at 68 days of life. We still had one more positive blood culture after the start of caspofungin and voriconazole, but all the subsequent blood cultures were negative. Parenteral nutrition was maintained for a total of 47 days until full enteral nutrition was achieved. Caspofungin and voriconazole were maintained for 36 days, but were suspended after two negative blood cultures. Intravenous fluconazole was started and maintained for 27 days.
Echocardiogram shows a large vegetation on the junction of superior vena cava to the right atrium.
A final echocardiogram showed an image compatible with a scarring injury in place of the old vegetation. Abdominal ultrasound showed only hepatomegaly with no other alterations of the parenquima or focal lesions of the liver. Examination of the retina showed no fungal injury, with only retinopathy of prematurity (II degree). The brainstem evoked response audiometry (BERA) was normal. Laboratory tests showed normalization of platelet and leukocyte counts, improved levels of liver transaminases, remaining only high direct bilirubin, clinically expressed by cholestasis and still present at discharge. The patient was hospitalized for 126 days, with 50 days of mechanical invasive ventilation, 13 days of mechanical non-invasive ventilation and 35 days of supplemental oxygen. The weight at discharge was 2180 g, with no need for supplemental oxygen.
Discussion
In this case, there were various risks factors for developing invasive candidemia, such as prematurity, low birth weight, use of broad spectrum antibiotics, full parenteral nutrition and central venous catheters.
Endocarditis remains an unusual complication of an invasive fungal infection. Exclusive clinical treatment with no surgery has been reported to be effective in an adult (caspofungin and voriconazole) 8 and, in one case, in a VLBW neonate (amphotericin-B and fluconazole). 9 Novel antifungal agents such as echinocandins (caspofungin) and second generation triazoles (voriconazole) have been recently introduced as treatment in life-threatening or refractory cases. Caspofungin has fungicidal activity, inhibiting B13D glucagon synthesis in the cell wall, a target present at the fungal cell and has shown excellent activity against Candida biofilm. It also has been reported to be a very safe drug in a study with 25 pediatric oncological patients, exhibiting, however, a poor penetration through uninflamed meninges and ocular vitreous. Voriconazole has a good distribution into brain, lungs, kidney, liver and spleen, demonstrating fungistatic activity, and described successfully in association with caspofungin for treatment of amphotericin-B non-responsive candidemias.10,11 Association of these drugs has not been reported in premature newborns, but we decided to try it because of the persistence of fungemia and absence of clinical improvement with amphotericin-B and fluconazole, monotherapy with voriconazole and the replacement of the central venous catheter.
We concluded that the combined treatment with caspofungin and voriconazole was effective in this Candida parapsilosis sepsis complicated by mural endocarditis, and showed no demonstrable adverse effects.
Footnotes
The authors report no conflicts of interest.