
Abstract
Background
Brucellosis is a zoonotic disease, with low incidence rate in developed countries, however the incidence rate in Middle Eastern countries remains high.
Chest symptoms in brucellosis cases account for about 15% of the cases, but dealing with respiratory system involvement is rare particularly pleural involvement.
Case Report
We report a case of a 60-year-old Saudi woman who was admitted with two months history of fever, productive cough anorexia and weight loss, contact with sheep. She was ill looking, underweight and febrile while she was on treatment. Examination of the chest showed signs of pleural effusion on the right side with right infrascapular crepitations. Chest X-ray: showed pleural effusion and right LL infiltrates. CT chest: showed right loculated, pleural effusion. Pleural fluid examination showed exudative changes, on culture of pleural fluid, Brucella species grew. AFB in pleural fluid was negative. She was treated with Streptomycin, Doxycyclin and Ciprofloxacin. She improved within one week of treatment and was discharged, after 14 days on antibrucella therapy.
Discussion
Pulmonary brucellosis is reported in medical literature occasionally but only few reports are available about pleural brucellosis. The challenge with pleural brucellosis and the association of loculated abscesses lies in therapy. Due to lack of previous information with such cases, we suggest that a period of more than six weeks is needed to treat this condition. We recommend that pleural brucellosis needs to be treated with at least two therapeutic agents for nine weeks.
Keywords
Introduction
Brucellosis is a zoonotic disease and remains endemic in several areas in the world. 1 3 The clinical polymorphism usually hinders correct and prompt diagnosis of the disease. 4 Mode of transmission of brucellosis is usually through direct contact with contaminated animals, inhalation of infectious aerosol particles, and ingestion of infected dairy products.3,4
The clinical manifestations of brucellosis are variable, however pulmonary features of brucellosis are uncommon particularly the pleural involvement.4–9
Brucellosis is endemic in Saudi Arabia with an incidence of 40 cases per 100,000 persons per year.6,8 However, there is only one previous report of pleural brucellosis in this country. 8 We report here a case of pleural brucellosis and discuss the mode of therapy.
Case Report
A 60-year-old woman who presented with fever for two months, remitting in nature associated with night sweats and productive cough of greenish sputum. She had a history of weight loss and anorexia for the duration of three weeks. No other chest symptoms were reported. There was a history of raw milk consumption and brucellosis was reported among her relatives.
On physical examination, she was febrile (38.2 °C), with bilateral axillary lymphadenopathy which was discrete, non tender and mobile. On chest examination, there were decreased breath sounds in the right lower zone with inspiratory crepitations. The liver and spleen were not palpable.
White blood count 9.6 × 109 cells/L with 79% neutrophils and 12% lymphocytes. Erythrocyte sedimentation rate was 123 mm/hr. Liver function tests showed that ALT was 89 µ/L and AST 89 µ/L. Sputum gram stain and culture were negative for any organism. An acid-fast bacilli in sputum was negative. Serum was negative for Brucella antibodies as Brucella titer (ELISA test was <:160) was negative. Chest x-ray showed right lower lobe infiltration with right slight pleural effusion (Fig. 1).
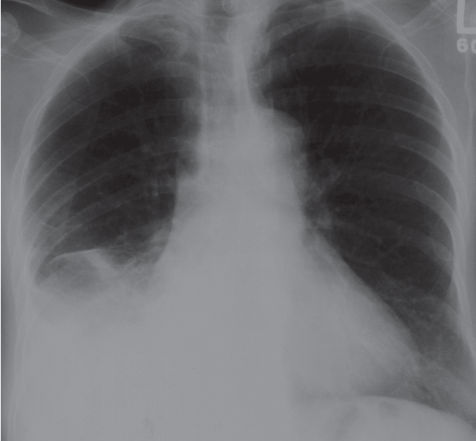
Chest x-ray.
The patient was admitted to the hospital and was started on community acquired pneumonia therapy (Cefuroxime 750 mg IV Q8 hrs for 10 days + Azithromycin 500 mg PO OD). The patient's condition did not show any improvement. A moderate size pleural effusion was seen on repeated chest x-ray in two days. Two days after admission a pleural tap was performed and it showed: RBC 1458 cells/µl, WBC 1280 cells/µl; lymphocytes 44%, neutrophils 30% and monocytes 25%. The lactate dehydrogenase in the pleural fluid was 1658 µ/L (133 in serum). Protein in the pleural fluid was 45 g/L (64 g/L in serum) Cytology showed no malignant cells. Four days after the pleural tap the pleural fluid grew scanty Streptococcus viridans which was thought to be a contaminant due to the fact that it was grown after 4 days with scanty amount. Six days later, the pleural fluid grew Brucella species, while blood culture remained negative after seven days.
CT scan of the chest showed right small loculated pleural effusion (Fig. 2). The treatment regimen was changed to Doxycycline 100 mg PO Bid, Ciprofloxacin 500 mg PO Bid and streptomycin 1g IM injection daily. Ciprofloxacin was used due to the fact that the patient was very sick. Five days after starting the antibrucella regimen the patient became afebrile and showed some improvement. Chest tube was removed after 11 days, and thoracic surgeon thought that the patient is inoperable regarding pleural decrotication due to other medical conditions. After 14 days on anti-brucella treatment the patient was discharged on Doxycycline 100 mg PO Bid, Ciprofloxacin 500 mg PO Bid to finish 9 weeks and streptomycin 1 g IM injection once daily to finish 21 days.
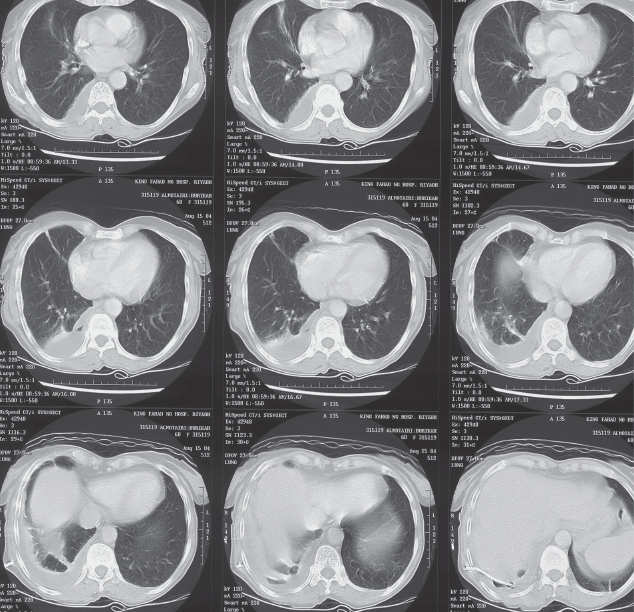
CT Scan.
The patient was seen in the clinic after four weeks on antibrucella treatment and she was doing much better clinically. She finished nine weeks of therapy and was found doing well, and a repeat chest x-ray showed no new events with minor old changes.
Discussion
Brucella species affecting the respiratory system seem to be an uncommon event.3–7 Lubani et al. described an analysis of 1500 patients with brucellosis in Kuwait. Nine patients with pulmonary brucellosis were described (0.6%), from which three patients had pleural involvement (0.2%). 5 Pappas et al. reported 37 patients with respiratory brucellosis from 450 brucellosis patients (8.0%) in the Balkan Peninsula from which four patients had pleural involvement (0.9%). 3 There are few case reports of brucella species affecting the pleura as haemorrhagic pleural effusion,8,9 chronic empyema,4,10 and exudative pleural effusion.11–13
Our case is different in the fact that the patient was having a loculated collection in the right pleural cavity and the surgical decortication was not possible. This was not described in literature before. The plan of management of a loculated pleural collection caused by brucellosis was to prolong medical therapy for longer than six weeks. The use of Ciprofloxacin in management of brucellosis in this case was based on literature review,14–16 where surgical decortication was not possible to compliment the drug regimen. Our patient was cured after nine weeks of Doxycycline and Ciprofloxacin with no need for surgical decortication. In cases of pleural brucellosis, where there is a loculated collection we recommend the use of ciprofloxacin in addition to other anti brucella agents for longer than six weeks.
Footnotes
The authors report no conflicts of interest.