
Abstract
Background
Our incidental observation of a remarkable improvement of disease activity following vaccination against typhoid in a patient with inflammatory bowel disease (IBD) was the incentive of this pilot study.
Methods
Ten IBD-patients (7 with ulcerative colitis and 3 with Crohn's disease) with disease activity grade 2–10 on simple colitis index were included in the study. The use of 5-ASA and prednisolone < 12.5 mg/day, but no other immunosuppressive drugs, were allowed during the trial. Live typhoid vaccine containing Salmonella serovar Ty21a (Vivotif ®, Berna) was given in standard doses on day 1, 3 and 5. Symptoms and endoscopic findings were followed up for a 3-months-period.
Results
Improvement of abdominal symptoms was recorded in 8 patients after 90 days, one patient was unchanged and one slightly worse. Endoscopic findings improved in 4 patients and were unchanged in 5 patients after 90 days. No side effects were observed.
Conclusion
Our results indicate that a live typhoid vaccine is well tolerated by patients with IBD of moderate activity. The symptomatic and endoscopic improvements were not dramatic, but encouraging enough to warrant further studies on the potential therapeutic effect of live typhoid vaccine on patients with IBD.
Introduction
Vaccination has been one of the most rewarding efforts in modern medicine, reducing or even abolishing the threat of several serious infectious diseases. A limited number of vaccines are necessary when living in the western world. But with increasing international travel, the need for a wider spectrum of vaccines is rising.
Current vaccination guidelines for chronic inflammatory bowel disease (IBD) patients allow extensive use of vaccines, even live vaccines when the patient is not immunosuppressed (1). Still IBD-patients tend to underutilize immunisation against vaccine-preventable diseases (2). Vaccines like live typhoid vaccine or cholera vaccine may temporally cause slight abdominal symptoms. Information about this may deter some IBD-patients from taking the vaccine and thus increase their risk for attracting dangerous infections.
Some animal studies show a protective or therapeutic effect of vaccines on experimental colitis (3–5). But whether human IBD is influenced by vaccines seems to be unknown. The experience of one of our ulcerative colitis patients evoked our interest on this question. She is a 46 years old female, with a 20 years’ history of left-sided ulcerative colitis documented by colonoscopy and biopsies. For the first 10 years she had almost continuous symptoms, had three colonocopies, and was treated with oral 5-ASA and intermittent cures with oral prednisone and steroid enemas. Then she prepared for travel to India and therefore had an oral vaccination with a live typhoid vaccine (Vivotif®, Berna). The first two weeks thereafter she had slight worsening of the diarrhea, but then followed a 3 months’ period with practically no symptoms. She thought this must be an effect of the vaccination as she found no better explanation. So when the colitis symptoms started to recur, she repeated the vaccination with the same vaccine. Again improvement ensued, and she stayed symptom free for 9 months. After this she has continued to take oral typhoid vaccine about once a year for the last 9 years, being convinced of the vaccine's positive effect on her ulcerative colitis. But she also continued to take oral 5-ASA during these years. A recent sigmoideoscopy showed a slight proctitis.
With this story in mind we discovered two other ulcerative colitis patients who could report something similar after oral vaccination, though their improvement was less convincing. These observations inspired us to perform a pilot study in order to disclose any modifying effects, positive or negative of live typhoid vaccine on the course of IBD.
Material and Methods
Since few data exist on the effect of live oral typhoid vaccine's effect on IBD, we did an open pilot study, well aware of its limitations when the numbers are so small.
Ten IBD-patients were included, 7 with ulcerative colitis or proctitis, 3 with Crohn's disease. Median age was 43 years, range 21–52 years. Male/female ratio 4/6. Duration of disease: median 7,5 years, range 2 months-23 years.
Inclusion criteria: 1. Patients with verified IBD by endoscopy, pathologic anatomic diagnosis of chronic inflammation or IBD, negative stool examinations for enteropathogenic microbes and Giardia lamblia. 2. Good general condition, and IBD activity index ≤ 10 for the last two weeks. 3. Age between 18 and 70 years.
Exclusion criteria: 1. Simple colitis index >10 with affected general condition. 2. Fever >38 °C. 3. Altered immunocompetence due to diseases or drugs like TNFα-inhibitors, azathioprin or corticosteroids in doses > the equivalent of prednisolone 12,5 mg pr. day. 4. Ongoing use of antibiotics. 5. Known allergy to any of the ingredients in the vaccine. 6. Pregnancy and lactation.
Written informed consent was obtained from each patient, and the protocol was approved by Regional Commitee for Medical Research Ethics, Norwegian Medicines Agency and Norwegian Social Science Data Service.
The patients were treated with a currently available oral vaccine containing the Salmonella Ty21a strain (Vivotif®, Berna) using the standard dosage for such vaccination against typhoid fever. One enterocapsule was taken with drinking water on day one, three and five. The patients took the capsules at home and noted on a report form when they were taken. Current medication was not changed unless medically indicated during the test period. Thus, seven ulcerative colitis patients were on oral or rectal medication with 5-ASA, two of these were steroid dependant, one using oral prednisolon 10 mg daily, the other hydrocortisone enema daily.
Bowel symptoms before treatment, on day 5, 15, and 90 from treatment start were scored. We used special diaries allowing scoring of disease activity index, the Harvey-Bradshaw Simple Index of Crohn's Disease Activity for patients with Crohn's disease, or the simple Clinical Colitis Activity Index (Walmsley) for patients with ulcerative colitis (6–8).
The patients were examined with flexible sigmoidoscopy by one of the investigators. To confirm the diagnosis, biopsies for histopathologic examination were taken from the recto sigmoid mucosa. Macroscopic changes in the mucosa were monitored by flexible sigmoideoscopy, at treatment start and at the following three consultations. The endoscopic changes were graded according to a simple scale: normal = 0, redness and edema = 1, erosions = 2, ulcers = 3. (9)
Blood tests were not included in the study because typically such tests give very little information as long as IBD activity is low to moderate.
Statistics
Data were analysed using the GraphPad Prism 5.0 (GraphPad Software Inc., U.S.A.) statistical software package. Differences between means were evaluated with nonparametric two-tailed Wilcoxon matched pairs test. P values less than 0.05 were considered statistically significant.
Results
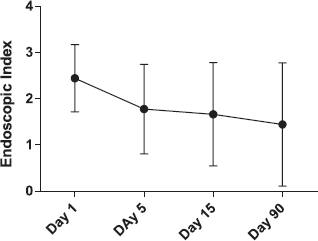
At first follow-up, 5 days after last vaccination day, there was a significant improvement of clinical symptoms, as compared with baseline, and, on average, this improvement remained for the following three months (Fig. 1). None of the patients became worse during the first five days. But one patient with a 17 years history of ulcerative colitis, who was on prednisolone 10 mg pr. day at the start, had a flare-up of symptoms after 15 days and had to increase the dose to 30 mg prednisolone per day. Disease activity was only slightly changed for the patients with Crohn's disease. A seemingly endoscopic improvement did not reach statistical significance (Fig. 2). No adverse effects appeared in any of the patients.
As compared with baseline, symptoms decreased significantly five days after oral treatment with live typhoid vaccine. Improvement persisted three months later. Endoscopic findings after oral treatment with live typhoid vaccine. Improvement appeared in some individuals but did not reach statistical significance for the whole group. Error bars = SD.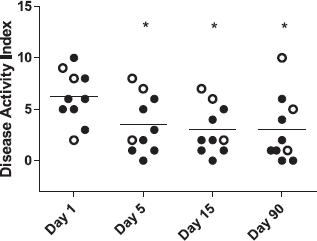
Discussion
We used a vaccine that has been in extensive use for decades in the combat of typhoid and paratyphoid fever. Its efficacy and safety is well documented through mass studies and millions of vaccinations world wide (10). But the vaccine contains live microbes that are supposed to alert the host's immune system through contact with intestinal mucosal immune receptors. It was unknown whether this contact would worsen the already inflamed mucosa of IBD-patients. Our previous patient contacts suggested there might be a period of slight exacerbation of symptoms after vaccination. We therefore followed up our patients closely, both endoscopically and with respect to symptoms, but no such early exacerbation was observed. Because the patients had symptoms at baseline, we could not withdraw their current treatment with 5-ASA or prednisolone, as this could have worsened their condition.
Already at day five of treatment, a significant improvement without any initial exacerbation was recorded. This finding encourages an active attitude to protect IBD-patients with vaccination when typhoid is a relevant threat.
Whether the vaccine has a real therapeutic effect in IBD, cannot be properly answered by this small pilot study. Both placebo effect and simultaneous medication influence our results. Still there was an improvement that we had not otherwise expected. An actual therapeutic effect of live typhoid vaccine in IBD can therefore not be excluded. Also, the suggestion is in fact supported by several prior experimental studies.
In animal models, the gut flora is essential for the development of colitis, and colitis may be influenced by antibiotics and certain strains of live bacilli able to alter or suppressing the flora. Thus, oral administration of Lactobacillus and Bifidobacterium attenuated DSS-colitis in mice (11; 12), while administration of the probiotic mixture VSL#3 (a mixture of bifidobacteria, lactobacilli, and streptococcus salivarius) to mice with IL-10 deficiency also reduced microscopic inflammation along with a reduction in mucosal secretion of TNF-α and IFN-γ (13).
A vaccine stimulates the immune system's targeted defence against defined pathogens, without having their mutilating effect. In addition to protection against specific microbes, vaccines may also strengthen the general defence mechanisms of the intestinal mucosa. An apparently irrelevant vaccine for the gastrointestinal tract proved to have an effect on the mouse colon, as a three-component Bordetella pertussis vaccine attenuated colitis in Gαi2-deficient mice (4). And administration of recombinant cholera toxin subunit B has been shown to inhibit murine TNBS experimental colitis (3). Cholera toxin may promote the induction of Th2 and Tr1 cells, enhance IL-10 production and inhibit secretion of IL-12 and TNF-α (14). Whether Salmonella Ty21a has similar effects, has not been shown. But experiments by Neish et al. showed that cells with previous contact with apathogenic salmonella got decreased inflammatory response when subsequently exposed to pathogenic strains (15). A vaccine against enterotoxigenic Eschericia coli (ETEC) composed of a live, attenuated Salmonella vector-expressing enterotoxigenic E. coli fimbriae, stimulated a biphasic Th cell response when given orally and suppressed the normally produced proinflammatory response. The vaccine reduced the production of TNF-α, IL-1 and IL-6, while it increased production of IL-4, IL-10, and IL-13 (5).
These results indicate that selected strains of microbes or vaccines may have a beneficial effect on a chronically inflamed mucosa in animal models of IBD. Also in human IBD the interplay between intestinal microflora and the gut seems to have a key role (16). The mucosa senses the luminal microbes through its complex system of receptors. Production of anti-microbial factors like defensins is one of the results, thereby supporting the intestinal surface with a protective layer that stops microbial invasion of the intestinal wall. Some microbes evade these protective mechanisms, by tolerating the defending peptides or down-regulating the sensing mechanisms of the mucosa, and thereby manage to invade the host. Pathogenic Salmonella is able to down-regulate the production of defensins, (17), and Shigella seems to suppress the production of cathelicidin, another important defence molecule of the colonic mucosa (18). In the case of NOD2/CARD 15 mutations, as seen in about one third of patients with Crohn's disease, the host has a defect sensing of microbes. Parallel to this a reduced amount of defensin (HD5) in terminal ileum of Crohn's disease patients has been reported (19). In these patients the amount of microbes inside the mucus covering the terminal ileal mucosa is also severely increased (20). These genetic and protective factors have not been examined in our pilot study as it contains very few Crohn's patients. But a therapeutic effect of vaccination might well be related to some change in these parameters.
In ulcerative colitis, the findings are more obscure, but here too the intestinal mucus layer is abnormally infested with microbes, suggesting a defective mucosal protection.
Recent clinical studies have given hope that altering or up-regulating the mucosal immune system may improve IBD-patients’ health. Stimulation of the mucosa by means of apatogenous paracites (21) or by granulocyte macrophage colony-stimulating factor (GM-CSF) both seem to have a therapeutic effect (22). This may signal a new policy in the treatment of IBD; to stimulate the mucosal immune system in a well designed way instead of applying a regimen for general immunosuppresion. The positive results of the present study support the idea of applying immunostimulation in the treatment of IBD, and further studies along these lines are warranted.
Statement of Interests
Declaration of personal interests: None. Declaration of funding interests: This study was fully funded by Helse Vest RHF, project number 911305.