
Abstract
Objective
The main aim of this study is to determine the improvement in quality of life in patients who have undergone radical surgery because of severe endometriosis.
Patients and Methods
This nonrandomized interventional study (quasi experimental) was carried out between January 2009 and September 2014. A total of 46 patients with diagnosis of severe endometriosis were included. Radical surgery, including hysterectomy, was performed. Acting as their own control group, the patients were asked to fill in a validated questionnaire of quality of life [Endometriosis Health Profile-5 (EHP-5)] and a visual analog scale of pain at the moment of the preoperative visit (one month prior to surgery) and six months after the surgery.
Results
Radical surgery for endometriosis was performed in 46 patients at our center over the period of six years. Among the patients, 73.9% of them had undergone previous surgery for endometriosis. In 82.6% of cases, a complete laparoscopic resection was carried out. Gastrointestinal tract resection was performed in 21.7%, and urinary tract resection was necessary in 8.7%. The mean age of the patients was 38.6 years. The rate of complications was 30.4%. Six months after the surgery, all items of the EHP-5 questionnaire had a lower score, which means an improvement in all aspects of quality of life related to endometriosis. The difference obtained between the scores before and after the surgery was statistically significant. The mean visual analog scale score before the surgery was 8.5, whereas it decreased to 1.4 after the surgery (P < 0.001).
Conclusion
Performing a radical surgery is a difficult decision to make; however, it can provide optimal results in terms of improvement of quality of life and, therefore, should be considered when conservative therapy fails.
Introduction
Endometriosis is a chronic, nonmalignant, estrogen-dependent disorder that affects 6%–10% of women of reproductive age. It is also the cause of pelvic pain in 50%–60% of the cases and accounts for up to 50% of infertility. 1 Its etiology remains unclear today, although a group of risk factors have been described, such as retrograde menstruation because of obstruction of menstrual flow, exposure to diethylstilbestrol during neonatal period, and prolonged exposure to endogenous estrogen.1,2
Although endometriosis usually affects ovaries and peritoneum, deep endometriosis, defined as infiltration of the peritoneum by >5 mm, can affect other structures. Intestinal infiltration occurs in 6%-35% of the cases of deep endometriosis, while urinary tract involvement has been reported in 1%–5% of the cases (Fig. 1). 3

Great endometriosic nodule in vesicouterine fold.
The classic symptoms of endometriosis are dysmenorrhea, pelvic pain, dyspareunia, and/or infertility. When gastrointestinal or urinary structures are involved, dyschezia, dysuria, or hematuria may also be present. Symptomatology and diverse imaging studies can approximate the diagnosis of the endometriotic lesions; nevertheless, the final diagnosis is obtained by surgery.4,5
Because endometriosis is a chronic disease, medical treatment should be the first choice, while surgical procedures should be reserved for patients who do not respond to conservative treatments and whose symptoms greatly affect their quality of life. Radical surgery is proposed for these cases.
Radical surgery for endometriosis refers to the elimination of all possible endometriosis implants found in pelvic and abdominal cavity, including hysterectomy and bilateral adnexectomy, and excision of the deep endometriosis lesions that can involve the urinary and digestive organs, as well as the rectovaginal and/or vesicouterine space. 3 It requires high specialization and a multidisciplinary approach (Fig. 2). 6

The firm adherences of the genital tract internal to the rest of pelvic organs are frequent, as in this case the sigma (called frozen pelvis).
The main aim of this study is to determine the improvement in quality of life in patients who have undergone radical surgery because of severe endometriosis. Secondary, we analyzed the clinical and surgical characteristics of the procedures.
Patients and Methods
Between January 2009 and September 2014, a total of 46 radical surgeries for endometriosis have been performed at our center. A nonrandomized interventional study was carried out (quasiexperimental). The study was approved by the local ethics committee of Hospital Universitario 12 de Octubre, Madrid, Spain (010/20008). The research complied with the principles of the Declaration of Helsinki.
The inclusion criteria were as follows: diagnosis of endometriosis by ultrasound or by previous surgery and severe symptoms because of endometriosis. All the included patients signed a written informed consent for radical surgery.
Severe endometriosis was defined according to the revised American Fertility Society classification stage IV. Acting as their own control group, the patients were asked to fill in a validated questionnaire of quality of life [Endometriosis Health Profile-5 (EHP-5)] and a visual analog scale of pain at the moment of the preoperative visit (one month prior to surgery) and six months after the surgery.
EHP-5 questionnaire, a scaled-down version of EHP-30, contains 11 questions (items): five items (including pain, control and powerlessness, emotional well-being, lack of social support, and self-image) from the core questionnaire and six items (including work, intercourse, and worries about infertility, treatment, and relationship with children and medical professionals) from the modular questionnaire. The score given to each item ranged between 0 and 4 (never = 0, rarely = 1, sometimes = 2, often = 3, always = 4, and not relevant if not applicable).
The visual analog scale (VAS) of pain comprises a horizontal line 10 cm in length anchored by the verbal descriptors no pain (score of 0) and worst imaginable pain (score of 10). The patient was asked to place a line perpendicular to the VAS line at the point that represented her pain intensity.
The baseline characteristics of the patients (age and parity), the presence or absence of major symptoms associated with endometriosis [dysmenorrhea, dyspareunia, dyschezia, or chronic pelvic pain (CPP)], and the history of previous surgery for endometriosis were noted down at the preoperative visit. The type of surgery and the complications when there had been any were checked at the medical history record.
Statistical analysis was performed using the statistical package for the social sciences, version 17.0. Special importance has been given to the results derived from the improvement in the patients' quality of life after surgery, which have been studied with the sign test, for the comparative study of nonparametric means. Statistical significance was considered as P < 0.05.
Results
From January 2009 to September 2014, a total of 366 interventions for suspected endometriosis have been performed at our center; 46 (12.5%) of them were considered for radical surgery.
Patients
Characteristics of patients are listed in Table 1. The mean age of the patients was 38.61 years (range 28–45 years). A total of 30.4% (14) of the patients had no history of pregnancy. Before radical surgery, the most commonly reported symptoms were dysmenorrhea (78.3%) and dyspareunia (47.8%). A total of 34.8% (16) of the patients were treated at the Chronic Pain Unit of our center for CPP.
Characteristics of the study population.
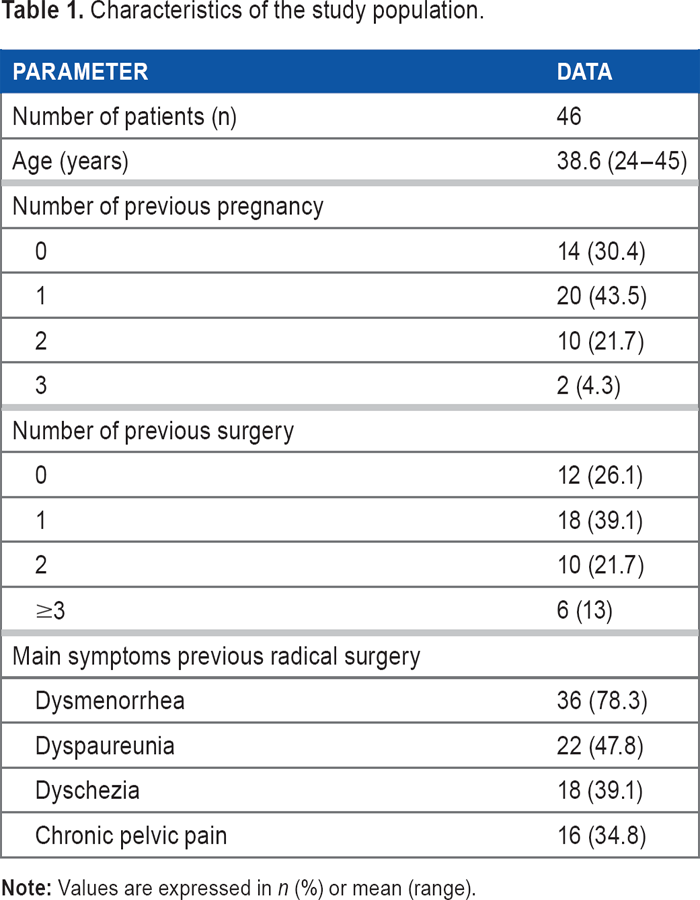
Approximately 28% (13) of the patients were treated with levonorgestrel-releasing intrauterine system. A total of 28% (13) of the patients were treated with GnRH analogues to induce pseudomenopause. A total of 73.9% (34) of the patients had undergone previous surgeries for endometriosis, up to three interventions in 13% (6) of the cases.
Surgical Procedure, Outcome, and Complications
Surgical procedures performed are listed in Table 2. In all patients, surgical treatment was assessed in a multidisciplinary team consisting of gynecologists, general surgeons, and urologists.
Surgical procedure and complications (n = 46).
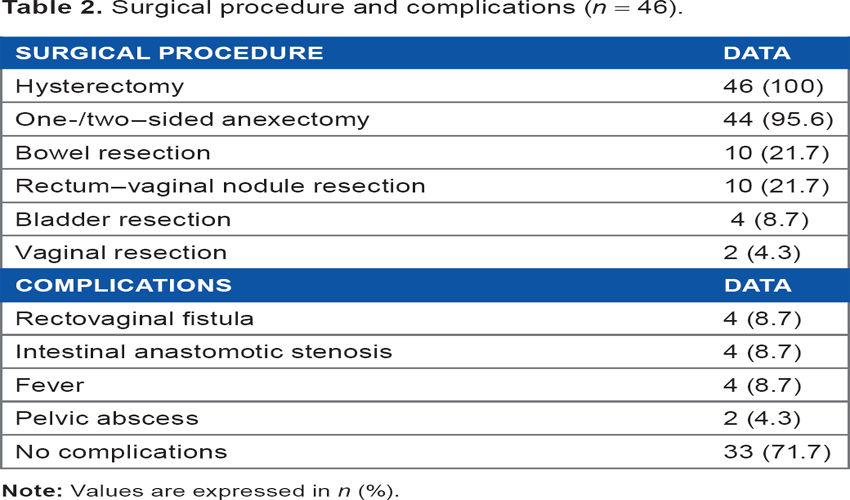
Hysterectomy was carried out in 100% (46) of the patients, associated with one-sided/two-sided oophorectomy in 95.6% (44) of the cases. Gastrointestinal tract was involved in 10 (21.7%) patients; a multidisciplinary team consisting of gynecologists and general surgeons was necessary to perform surgery in these cases. Also, in four (8.7%) patients, urinary tract resection was necessary, and therefore, the urologists were additionally consulted. In 82.6% (38) of the cases, a complete laparoscopic resection was carried out.
The rate of complications was 30.4% (14). Major complications occurred in eight (17.4%) patients: four (8.7%) patients with rectovaginal fistula and four (8.7%) patients with intestinal anastomotic stenosis. Neurological disorders did not occur. Up to now, none of the patients included have needed an intervention because of persistent pain. During the follow-up, none of the patients had undergone surgery in a different facility.
Response to the Questionnaires
Regarding the results of the EHP-5 questionnaire, the initial response rate (preoperative questionnaire) was 100%. Six months after surgery, the questionnaire was completed by 100% of the patients.
As shown in Table 3, before surgery, the worst scores were for the items of functional impotence (mean 3.2 out of 4), dyspareunia (mean 2.8 out of 4), pain (mean 2.7 out of 4), and emotional well-being (mean 2.6 out of 4). Six months after the surgery, all items had a lower score, which means an improvement in all aspects related to endometriosis. The difference obtained between the scores before and after the surgery was statistically significant in every item, except the concern about fertility and childbearing (During the last four weeks, how often because of your endometriosis have you felt depressed at the possibility of not having children/more children). The patients referred a significant improvement in pain, control, and powerlessness (During the last four weeks, how often because of your endometriosis have you felt as though symptoms are ruling your life?), emotional well-being, self-image, and sexual relationships.
Results of Endometriosis Health Profile-5 questionnaire one month prior to surgery and six months after surgery.
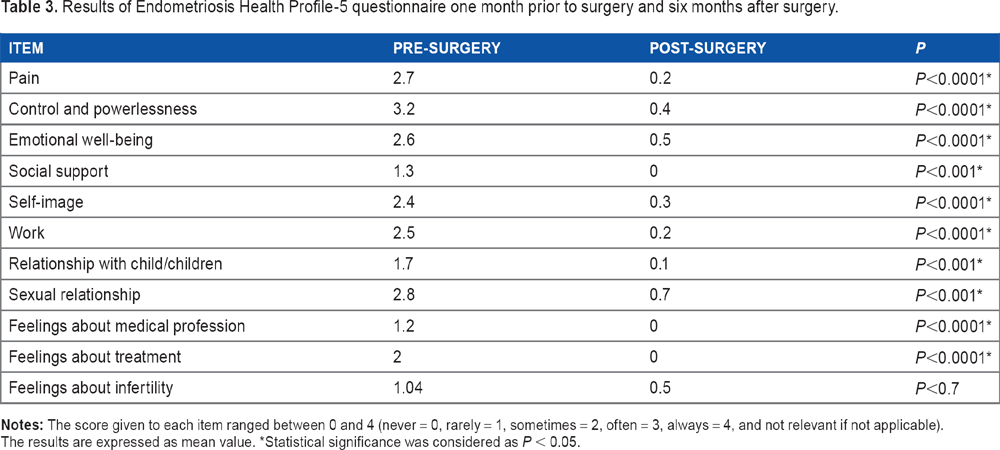
Statistical significance was considered as P < 0.05.
Regarding the results of the VAS of pain one month before and six months after surgery, the average score given preoperatively was 8.6, whereas it decreased to 1.5 after the surgery, achieving statistically significant difference (P < 0.001).
Discussion
Endometriosis is a disease that can significantly affect quality of life and sexual function. Deep endometriosis can affect genital and extragenital systems, such as the gastrointestinal and urinary tract. Management should be carried out by a multidisciplinary team consisting of gynecologists, colorectal surgeons, and urologists.3,7
In several cases, medical treatment or conservative surgery is not enough to reduce the symptoms caused by the disease. In these cases, radical surgery should be considered, particularly when the gastrointestinal tract or the urinary tract is involved.3,6,8 Radical surgery refers to the elimination of all possible endometriosis implants found in pelvic and abdominal cavity, including hysterectomy and bilateral adnexectomy. Intestinal resection performed in cases of deep endometriosis that compromises the rectum can help to improve digestive symptoms and thereby quality of life and sexual well-being. 8
In this study, we obtained a statistically significant improvement in the quality of life of patients six months after radical surgery. Despite the improvement in quality of life, performing a radical surgery is a difficult choice due to the complexity of the surgery, the high rate of complications, and the side effects (premature menopause and infertility). This option should be restricted to patients for whom medical treatment and conservative surgery fail.
In a study conducted by Shakiba et al 9 that compared conservative surgery (n = 120) with radical surgery (n = 120) over seven years, the authors reported a rate of reoperation because of persistent or recurrent symptoms in patients for whom the uterus and ovaries were excised of 8%. In this study, up to now, none of the patients included have needed a reoperation because of persistent pain.
Regarding the surgical approach, it is noted in the literature that laparoscopy has been associated with lower rates of complications when compared to laparotomy approach (18.3% vs 49%) (9–10). Nieboer et al 10 further asserted that laparoscopic hysterectomy resulted in improvement in the quality of life when compared to laparotomy. Laparoscopic approach also allows performing pelvic nerve sparing more easily. 5 However, there is still a high incidence of urinary, rectal, and sexual neurological dysfunction described in the literature when radical surgery is performed. This can also worsen the quality of life after surgery. In this study, 82.6% of the surgeries were performed with a laparoscopic approach. The patients were inquired about any changes in urinary (frequency and incomplete voiding), bowel (severe constipation), and sexual functions (arousal and vaginal lubrication). During the immediate and long-term postsurgical follow-up, no associated neurological dysfunction was observed.
Our study has several limitations. The number of patients included in the study is small (n = 46), and, although our results reached statistical significance, they may not be widely applicable. The short-term follow-up can ignore long-term complications (such as increased cardiovascular events and increased all-case mortality) and pain recurrence in our group.
Conclusion
Although this study had only a small population of patients, most of the results were statistically significant. Based on these results, it is concluded that after radical surgery there was an improvement in all of the aspects analyzed, except of questions related to fertility. Additionally, the improvement in the quality of life of patients was reflected in the lower score on the VAS of pain after surgery. Endometriosis is a complex disease that can affect our patient's daily life. This study shows that radical surgery can provide optimal results in terms of improvement in the quality of life. However, due to its overall rate of postoperative complications, it should be considered only when conservative therapy is not enough and always with a multidisciplinary approach.
Current Knowledge on the Subject
Endometriosis is a complex disease that can impressively affect a patient's daily life and requires a multidisciplinary approach. Traditionally, radical surgery has been performed in patients resistant to conservative treatments. The decision to perform a radical surgery is difficult to carry out because of its complexity.
What this Study Adds
Radical surgery can provide optimal results in terms of improvement in the quality of life of patient and, therefore, should be considered when conservative therapy fails to deliver the expected results.
Footnotes
Acknowledgments
The authors thank Carlos Holguera, Alvaro Tejerizo, and Gregorio Lopez for their technical assistance.
Author Contributions
Study conception and design: CMDH-L, JLM-G, ROP, and JSJ-L. Acquisition of data: CMDH-L, RV-C, and AD-á. Analysis and interpretation of data: CMDH-L, JLM-G, AD-á, and ROP. Drafting of manuscript: CMDH-L, JLM-G, JSJ-L, LM-H, and CA-C. Critical revision: JLM-G, ROP, and JSJ-L.