
Abstract
Purpose
The purpose of this study is to compare the health of primary caregiving African American grandmothers with diabetes with African American women with diabetes who were not primary caregivers.
Design
Using a comparative, descriptive, cross-sectional design, 34 African American primary caregiving grandmothers were compared with 34 non-caregiving women with diabetes mellitus; women aged 55–75 years were recruited for this study throughout the central Arkansas.
Methods
To measure the overall health, data on blood pressure, body mass index measurements, HbA1c levels, total cholesterol, and urine protein and creatinine levels were collected from all the participants.
Results
Statistically significant differences between the caregivers and non-caregivers groups in systolic pressure (t = −3.42, P = 0.001) and diastolic pressure (t = −3.790, P = 0.000) and urine protein (W = 294.00, P = 0.000) were noted. Additionally, a clinically significant difference in HbA1c was noted between groups.
Conclusion
Differences in systolic and diastolic pressures, urine protein, and clinically significant differences in HbA1c suggest that African American primary caregiving grandmothers with diabetes mellitus may have more difficulty in maintaining their diabetic health than non-caregiving African American women.
Introduction
Diabetes is particularly burdensome for African American women over the age of 50 years. 1 In addition to the challenge of managing their diabetes, an increasing number of older African American women are overseeing the role of primary caregivers of their grandchildren. 2 Other studies have shown that caregiving responsibilities may also affect physical health3,4 and caregivers often have more health problems than non-caregivers.4–6 In particular, caregiving of a grandchild has been associated with increased risk for diabetes, hypertension, cardiovascular disease, and insomnia. 7 Considering that a quarter of all African American women over the age of 50 years have diabetes, it is likely that at least a quarter of African American primary caregiving grandmothers have been diagnosed with diabetes mellitus. Yet, few studies have focused on the impact of caregiving responsibilities on the diabetic health of this population of women. 8
However, multiple studies have noted that caregiving grandmothers' experience increased stress and other health concerns because of the caregiving role.9–11 For example, stress of caregiving can also lead to depression.4,12 Musil et al 4 found that depression was associated with greater parenting, primary responsibility for caregiving to grandchildren, and avoidant and minimizing coping among caregiving grandparents.
Caregiving grandparents tend to neglect their health, which leads to health problems. 13 Indeed, caregiving has been found to exacerbate pre-existing conditions such as diabetes, high blood pressure, or cardiac disease as a result of stress of caregiving.14,15 In a study of African American primary caregiving grandmothers, worsening health was found in participants after the initiation of caregiving in 28% of the sample. 16 However, no studies have examined the clinical impact of caregiving on diabetic health in African American grandmothers raising their grandchildren. As a first step in moving toward interventions, the current study compared the diabetic health of African American primary caregiving grandmothers with diabetes to the health of African American women with diabetes who do not have caregiving responsibilities.
Theoretical Framework
Orem's Self-care Deficit Theory of Nursing (SCDTN), a model for determining an individual's self-care deficit, needs, and the role of nursing, provided the framework for this study. SCDTN is an extensively used nursing theory developed by Dorothea Orem. The theory is very similar to Betty Newman's system model; both focus on the patient need for nurse guidance to meet a health care need. Therapeutic self-care demand, self-care deficit, and self-care agency are the main concepts of the SCDNT. 17 Therapeutic self-care demand is defined as the totality of measures required to maintain health, development, and well-being. 18 Self-care agency is the acquired ability to perform self-care. 19 It is composed of several power components that are the capabilities specific to health-related self-care actions. 20 Self-care deficit occurs when one is unable to perform the actions necessary to maintain health. 17
The SCDNT's fundamental premise is the lack of self-care agencies that meet some or all of the components of therapeutic self-care demand. An increase in therapeutic self-care demand or a decrease in the individual's self-care agency may interfere with the attainment of the self-care requisites; thus, a self-care deficit exists. 20 The diabetic African American primary caregiving grandmother may experience deviations in power components due to stress and fatigue resulting in decreased self-care agency. This diminished the ability for performing self-care management activities (therapeutic self-care demand), subsequently impacting her overall diabetic health (Table 1).
SCDTN.
Methods
As described in Carthron et al, 3 this comparative, descriptive, cross-sectional design study compared 34 African American grandmothers with Type 2 diabetes mellitus who were the primary caregivers of their grandchildren with 34 African American women with diabetes who were not the primary caregivers of their grandchildren. This study was part of a larger study examining self-management activities and health of African American primary caregiving grandmothers with diabetes.
Inclusion and exclusion criteria
African American women aged 55–75 years with a diagnosis of Type 2 diabetes and also with an ability to understand and provide informed consent as determined by a minimum score of 24 on the Mini Mental Status Examination (MMSE) were included in this study. Caregiving grandmothers had to be the primary custodial caregiver of their grandchild (under the age of 18 years), with no parent living in the home and with initiation of caregiving within the previous 3 years.
Grandmothers who were caregivers for persons other than their grandchildren were excluded from the study. Women with a known hemoglobin variant disorder such as sickle cell or thalassemia were excluded from the study since hemoglobin variant disorders often alter the accuracy of HbA1c levels, requiring the use of an immunoassay or boronate-affinity method.
Participants from both groups were recruited from African-American churches, a local children's hospital, a large metropolitan hospital in Arkansas, senior citizen recreational centers, daycare centers, and local health fairs and community events, eg, Arkansas Diabetes Walk. Written consent was obtained from all the participants, and the study was approved by the Institutional Review Board of the University of Arkansas for Medical Sciences. The research was conducted in accordance with the principles of the Declaration of Helsinki.
Measures
Demographic measures
Data on age, financial status, education, housing status, health insurance, and length of caregiving were collected using an author-developed questionnaire. The questionnaire was read to participants if requested.
Diabetic health measures
The author or a research assistant collected data on blood pressure, body mass index measurements (BMI), HbA1c level, total cholesterol, urine protein, and urine creatinine levels from all the participants. Obesity and hypertension are the major risk factors for cardiovascular diseases. 21 HbA1c, one of the best measures of glycemic control, provides an average glucose measurement of the previous 2–3 months. 22 Increased cholesterol also contributes to cardiovascular diseases in those with diabetes 23 (a normal total cholesterol level is below 200 mg/dL). Urine protein and urine creatinine levels are indicators of kidney function, and elevated urine protein is considered a marker of early kidney diseases. 24 Creatinine is removed from the body entirely by the kidneys; therefore, elevated creatinine levels often are indicative of kidney dysfunction.
Blood pressure was measured manually with each participant seated, quiet with legs uncrossed as recommended by the Centers for Disease Control and Prevention. BMI was obtained by measuring the height and weighing of each participant using the same digital scale, and BMI was then calculated using the participant's weight in pounds divided by height in inches squared. Then, the result is multiplied by 703 to obtain the BMI. A BMI over 25 is considered overweight and above 30 is indicative of obesity.
A fingerstick blood sample was collected from each participant to ascertain HbA1c levels. HbA1c was determined using the Metrika's A1CNow+ monitor. The values have been found to have a good correlation (r = 0.758) with standard laboratory testing values. 25
To obtain cholesterol levels, the Accu-Chek Instant Plus cholesterol test was used, which is a total cholesterol meter that uses a single drop of blood to determine total cholesterol, and the results have been highly correlated (r = 0.869) with the clinical laboratory results. 26 Both the Metrika's A1CNow+ monitor and the Accu-Check Instant Plus were calibrated prior to each use.
A urine sample was obtained from each participant to determine the presence of protein and creatinine in the urine using Bayer Multistix PRO 10LS urine dipsticks. Croal et al 27 evaluated the accuracy of the Bayer Multistix PRO 10LS by comparing the test strip results (both visually and by using the Clinitek 50) with central laboratory results. Overall agreement with the central laboratory was 94.9% (visual) and 91.1%. Overall agreement with the protein band was 94% (visual) and 95.7%.27,28 To ensure interrater agreement for dipstick urine results, the author and a research assistant observed the same specimen with the same results.
Statistical Analysis
All variables were initially analyzed descriptively; the mean, median, standard deviation, and minimum and maximum values were calculated. Demographic data were analyzed using independent t-tests, Mann-Whitney U, and chi-square tests. Data on blood pressure, BMI, HbA1c levels, total cholesterol, urine creatinine, and urine protein levels between the caregiving and non-caregiving group were analyzed using a one-tailed independent t-test with Bonferroni correction to control for multiple t-tests and reduce the possibility of Type 1 error. An alpha level of 0.001 was used for all statistical tests. Since the urine creatinine and urine protein data were continuous but not normally distributed, the Mann-Whitney U test was used.
Results
Demographic characteristics
Table 2 shows the demographic data for each group and the results of tests for equivalence. The mean age of the caregiving group and non-caregiving group was 59.34 years and 63.03 years, respectively. There was a significant difference in housing status with caregiving grandmothers more likely to reside in a house rather than an apartment. No significant differences between the two groups were noted in age, financial status, education, or health insurance.
Demographic characteristics.

Dependent t-test,
Mann-Whitney U,
Chi-square.
Diabetic health comparisons
Table 3 shows the differences in diabetic health measures between the two groups. Significant differences were found in systolic (t = −3.42, P = 0.001) and diastolic pressures (t = −3.790, P = 0.000). Mean systolic pressure was significantly higher in the caregiving group (M = 145.82, SD: 15.68) than in the non-caregiving group (M = 132.79, SD = 17.42), and diastolic pressure was also significantly higher in the caregiving group (M = 87.09, SD = 15.15) than in the non-caregiving group (M = 71.97, SD = 17.65). Hypertension was observed in 58.8% (n = 20) of the caregiving group (systolic ≥140 mmHg with a diastolic ≥90 mmHg), compared to just 20.5% (n = 7) of the non-caregivers.
Metabolic control comparisons.
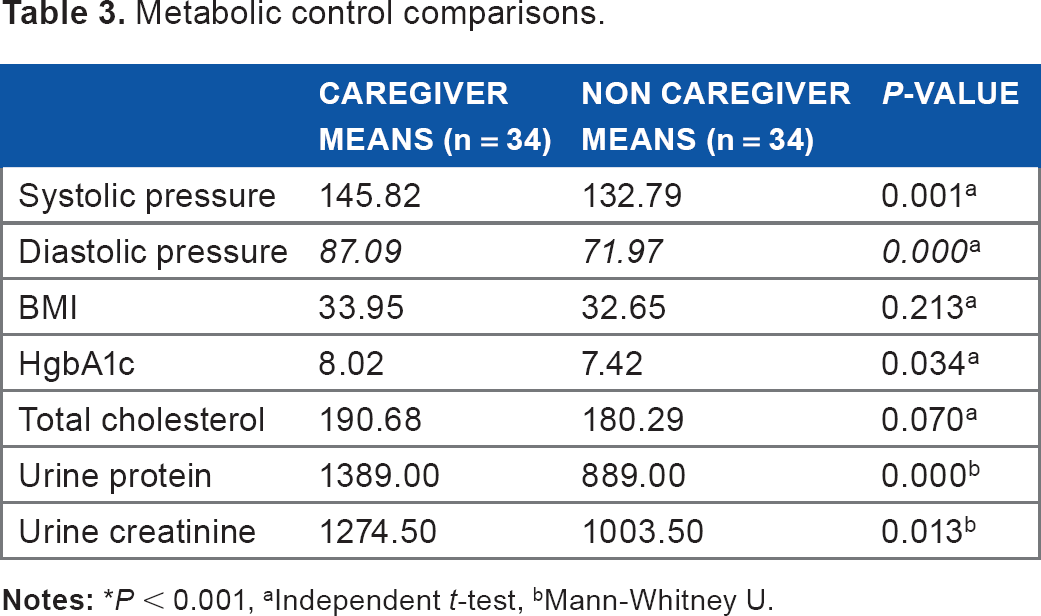
independent t-test,
Mann-Whitney U.
Additionally, a significant difference was noted in urine protein (W = 294.00, P = 0.000), with the caregiving group having higher levels than the non-caregiving group. Fifty percent (n = 17) of the caregiving group had at least 30 mg of protein in their urine, which is often indicative of early kidney disease. 29 Three participants in the caregiver group had a urine protein ≥300 mg/dL, which is indicative of more advanced kidney disease. In contrast, no one in the non-caregiving group had a protein level >30 mg/dL. No significant differences were noted between the two groups in BMI, HbA1c, total cholesterol, or urine creatinine. However, a clinically significant difference was observed in HbA1c levels with the caregiving group than with the non-caregiving group.
Study limitations
Several limitations of the study must be addressed. As previously cited, the original study by Carthron et al 3 targeted a sample size of 68 to detect clinically meaningful differences (at 1%) in HgbA1c with sufficient statistical power. The current study presents on secondary analyses with a different goal. Thus, findings should be cautiously interpreted as effects of covariates, moderators, or mediators not accounted for could have impacted conclusions (eg, physical activity levels for BMI and hypertension medication use for blood pressure). Although such variables were not included because of these a priori power considerations, the presented analyses are reasonable given the design and goal, with this explicit caveat. Next, the study was a cross-sectional design and, therefore, suggests that interpretation of the results should be limited to the groups examined at the time of this research and only associations can be examined. We did not ask about the length of underlying chronic illness, so it is plausible that the caregiving group had higher blood pressures, urine creatinine, and urine protein levels unrelated to caregiving. Finally, it is important to note that the results may not be generalizable to younger cohort of diabetic African American caregiving grandmothers.
Discussion
Hypertension is often referred to as the “Silent Killer,” and this may be especially true for African American primary caregiving grandmothers. In this study, significantly higher systolic and diastolic pressures were noted in the caregiving than in the non-caregiving group and that may have been attributed to the increased stress due to caregiving responsibilities. This is consistent with the findings of others.15,30–32 Of course, it is possible that the caregiving group was hypertensive before to the initiation of caregiving, but even so, it is likely that the demands of caregiving exacerbated the condition.
A significant difference in urine protein was also noted between the caregiving and non-caregiving groups. Since microalbuminuria is a predictor of early mortality, 33 this finding is particularly alarming. Emotional stress has been known to increase benign microalbuminuria, 34 and it is possible that the responsibilities of caregiving contributed to microalbuminuria in the caregiving group. Furthermore, the large amounts of protein in the caregiving group, coupled with the significantly higher systolic and diastolic pressures, point to a risk of kidney dysfunction.
The lack of significant difference in BMI between the caregiving and non-caregiving group was unexpected since multiple studies have noted increases in BMI with caregiving.35,36 However, some studies have found that primary caregiving grandmothers do not experience health declines. 37 For example, Baker and Silverstein 38 found that caregivers in the role for 2 years become more health conscious after the initiation of caregiving (ie, exercising more, eating healthier).
Caregiving grandmothers had clinically significant differences in HbA1c with the caregiving group having higher HbA1c levels. This conflicts with the Balukonis et al's 8 study, which found that custodial grandmothers with the highest level of caregiving had the second lowest HbA1c levels. Yet, caregiving grandmothers have been found to have a decreased ability to integrate self-management activities into their daily lives2,3 leading to a self-care deficit. Several studies have noted that caregiving grandmothers experience stress,6,15,39 and stress increases glucose levels.32,40 However, stress was not measured in this study. Furthermore, this study was cross-sectional, and therefore, it cannot be definitely determined that what factors affect HbA1c levels.
No significant difference in total cholesterol was found between the caregiving and non-caregiving group; however, the caregiving group had cholesterol levels 5.5% higher than the non-caregiving group. This finding is consistent with the literature, which notes that caregivers consume more saturated fats than women who are not caregivers.41,42 Primary caregiving grandmothers often have time constraints, and they may have higher cholesterol levels because they eat quick “on-the-go” meals, such as fast foods, for themselves as well as their grandchildren.
Finally, higher urine creatinine levels were noted in the caregiving group. It is possible that these higher urine creatinine levels in the caregiving group are indicative of underlying renal dysfunction due to the stress of caregiving.
Implications for Practice and Research
Diabetes disproportionately affects African American older adult women and thus affects many African American primary caregiving grandmothers. Unfortunately, African American primary caregiving grandmothers' health needs may go unrecognized. Clinicians should assess caregiving grandmothers with diabetes to determine whether chronic stress as well as a decreased ability to self-manage their diabetes is ultimately leading to poorer diabetic health outcomes and then develop individualized medical and self-management plans tailored to the African American primary caregiving grandmothers because of their specific challenges in managing their diabetes. In addition, diversity among clinicians should be considered to ensure racial concordance when providing education in relation to healthy food choices that are also culturally relevant.
Replicating this study with a larger sample size is essential to gain a fuller picture of the health of these grandmothers. Also, since factors such as stress levels, comorbidities, time constraints, financial, and social needs often affect the health of primary caregiving grandmothers, exploring these factors is imperative to the development of tailored interventions, to assist them in maintaining control of their diabetes, and to delay the progression of diabetes-related complications.
Footnotes
Author Contributions
Conceived and designed the experiments: DLC. Analyzed the data: DLC. Wrote the first draft of the manuscript: DLC. Contributed to the writing of the manuscript: DLC and MRB. Agree with manuscript results and conclusions: DLC. Jointly developed the structure and arguments for the paper: DLC. Made critical revisions and approved final version: DLC and MRB. All authors reviewed and approved of the final manuscript.