
Abstract
Women with gestational diabetes mellitus are at increased risk for developing diabetes mellitus (DM), mainly type 2 DM, as well as metabolic syndrome. The presence of subsequent pregnancies increases the risk. In addition, pregnancy in patients with type 1 and type 2 DM also elevates the risk of morbidity and mortality for both mothers and offspring. Thus, all women with pre-existing type 1 or type 2 DM should receive preconception care to optimize glycemic control (HbA1c ≤ 6%). In those cases with macrovascular or microvascular complications, family planning is even more important in order to avoid the risk of aggravation of such complications associated with a new pregnancy. The present review analyzes the metabolic and cardiovascular repercussions of hormone contraception in non-diabetic women as well as in type 1 and type 2 DM patients with and without macrovascular and microvascular complications. Finally, the recommendations pertaining to hormonal contraceptive methods for women with diabetes are summarized.
Introduction
Women with gestational diabetes mellitus (GDM) are at increased risk for developing diabetes mellitus (DM), usually type 2, after pregnancy. In addition, women with prior GDM are found to have higher risk of developing metabolic syndrome that includes altered lipid profile and high blood pressure. 1 The presence of subsequent pregnancies together with other risk factors such as obesity increase the risk, and, therefore, it is imperative to establish effective choices for contraception.
Pregnancy in patients with type 1 and type 2 DM also increases the risk of morbidity and mortality for both mothers and offspring. 2 Therefore, women with DM and childbearing potential should be educated about the need for good glucose control, that is, stabilizing hemoglobin A1c (HbA1c) at ≤6% before pregnancy. A prospective review of seven cohort studies analyzed the absolute risk of having a congenital anomaly in relation to periconceptional HbA1c levels. 3 The analysis showed that for each standard deviation unit increase in HbA1c, the associated risk of a congenital malformation increased by an odds ratio (OR) of 1.2 (95% confidence interval [CI] 1.1–1.4). Thus, all women with pre-existing type 1 or type 2 DM should receive preconception care to optimize glycaemic control. 4 In addition, those DM patients with macrovascular (ischemic cardiopathy) or microvascular complications (nephropathy, retinopathy, or neuropathy) should also receive preconception care in order to avoid the risk of aggravation of such complications associated with a new pregnancy. 2
There are multiple contraceptive treatments currently available, and none of them are contraindicated for DM patients. Among the contraceptive methods, hormonal contraceptives are among the most reliable, presenting a similar Pearl Index in both healthy and diabetic women. 5 The results of observational cohort studies have suggested that because hormonal contraception interferes with carbohydrate and lipid metabolism, caution should be used when this contraceptive method is selected for DM patients. It is also important to point out that DM patients are more likely to lack contraception compared with women without DM. 6
The present review analyzes the metabolic and cardiovascular repercussions of hormone contraception in non-diabetic women as well as in type 1 and type 2 DM patients with and without macrovascular and microvascular complications. Finally, the recommendations pertaining to hormonal contraceptive methods for diabetic patients are summarized.
Impact of Hormonal Contraception on Carbohydrate Metabolism in Women without Diabetes
Oral hormonal contraception
In general, estrogen does not appear to have an ostensible effect on carbohydrate tolerance or insulin sensitivity.7,8 Progestins do not affect the clotting factors or blood pressure, and their effect on lipid metabolism is usually low and variable. 9 While some studies have shown a nonsignificant effect on the lipid profile, others have found an increase in LDL-cholesterol and a decrease in HDL-cholesterol and triglycerides.10,11 Combination of estrogen and progestin modulates the effects of each steroid on lipids profile, and it has been suggested the effect of second generation pills is different from third or fourth generation combination estrogen and progestin pills. 12 Progestins can also induce a mild impairment of carbohydrate tolerance and increase insulin resistance (Table 1). 13
Main secondary effects of different types of steroidal compounds of hormonal contraception.24,81
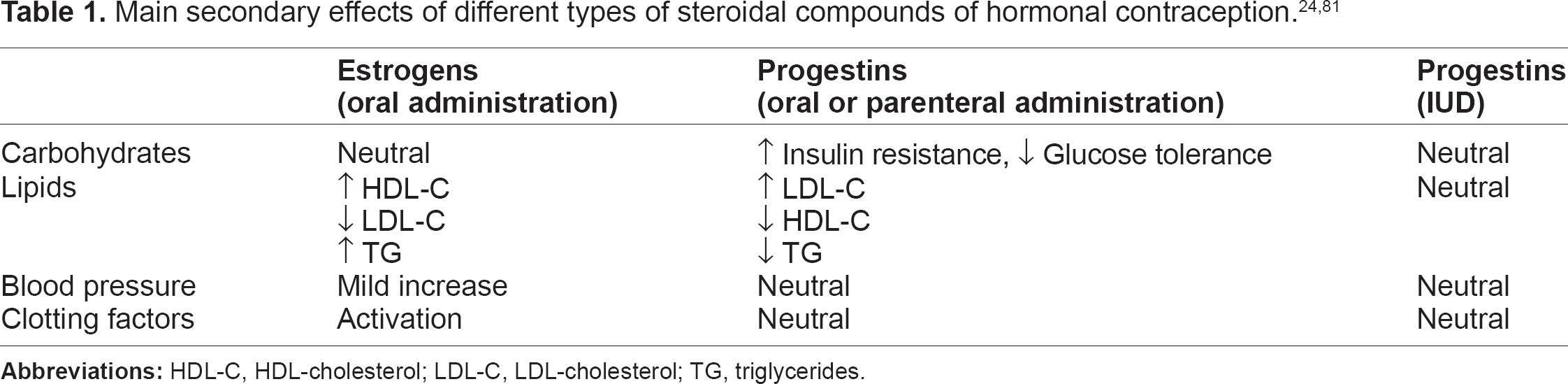
The study of Godsland et al 7 compared seven oral contraceptive formulations that contained various doses and types of progestin combined with ethinyl estradiol (combined oral contraceptives [COCs]) versus two formulations that contained progestin alone. As compared with controls, women taking combination drugs did not have increased serum total cholesterol levels but did have increases of 13% to 75% in fasting triglyceride levels. Levels of LDL-cholesterol were reduced by 14% in women taking the combination containing desogestrel and by 12% in those taking low-dose norethindrone. Levels of HDL-cholesterol were lowered by 5% and 16% by the combinations containing low-dose and high-dose levonorgestrel, respectively; these decreases were due to reductions of 29% and 43%, respectively, in the levels of HDL subclass 2. Combination drugs with norethindrone and desogestrel were associated with lower plasma glucose levels of the glucose-tolerance test as well as lower insulin response. 7 In addition, the use of combined oral contraceptives increased insulin resistance as opposed to the use of progestin alone. 14
Shoupe et al analyzed the effects of desogestrel on carbohydrate metabolism. 14 Although the use of COCs was associated with a significant decrease in glucose tolerance (10%–15%) and insulin response (10%–30%), the effect on carbohydrate metabolism was less prominent with desogestrel compared with levonorgestrel and norethindrone. 15 On the contrary, the results of a randomized clinical trial that compared the combination of a low dose of ethinylestradiol (EE) in addition to desogestrel (DSG) versus a low dose of EE in addition to chlormadinone acetate (CMA) showed that DSG, even when associated with low EE dose, decreased insulin sensitivity, while the combination of EE and CMA did not deteriorate insulin sensitivity and induced a favorable lipid profile. 16
A recent meta-analysis by Lopez et al that analyzed 27 randomized clinical trials conducted in nondiabetic women who were receiving different hormonal contraceptives (COC, progestin alone, intramuscular, and vaginal rings) showed the low impact exerted on the carbohydrate metabolism by the different contraceptive methods analyzed, although most of the studies reviewed included a small number of participants, with a significant dropout rate. 17
In summary, the effects on carbohydrate metabolism of the different hormonal contraceptive methods are relative low using low doses of progestins, with a limited clinical effect. These effects are far less pronounced with lower dose preparations of estrogens and with formulations using low doses of progestins. 8
The risk of developing DM in women treated with COCs has been shown to be similar or even lower compared with the general population.18,19 Thus, a study conducted in 98,590 female nurses free of diabetes, cardiovascular disease, and cancer that were followed up for four years showed that women who had used oral contraceptives in the past did not present a higher risk of developing type 2 DM. 20 On the contrary, the results of the CARDIA (Coronary Artery Risk Development in Young Adults) study that included 1940 women concluded that the use of COCs was associated with lower baseline glucose levels as well as a lower odds (OR = 0.56) of diabetes after 10 years of follow-up. 21 More recently, a nested case-control study analyzed the association between hormonal contraceptive use, categorized by the androgenicity of the progestin component, and the risk of GDM. The use of low-androgen hormonal contraceptive before pregnancy was associated with a slight reduction (16%) in risk of GDM (OR 0.84, 95% CI 0.58–1.22), whereas the use of high-androgen hormonal contraceptive was associated with a modest increase (43%) in GDM risk (OR 1.43, 95% CI 0.92-2.22). 22
Non-oral hormonal contraceptives
The progestins alone, such as medroxyprogesterone acetate (MPA) (Depo-Provera®), administered every three months, and norethisterone enanthate (NET-EN), administered monthly, are among the contraceptives administered intramuscularly. There are also combined intramuscular contraceptives such as cypionate estradiol + medroxyprogesterone acetate or norethindrone + estradiol valerate. Both compounds MPA and NET-EN when used for a year cause an increase in blood glucose and insulin levels (baseline and 2-hour oral glucose tolerance test), with minor increases observed with NET-EN although not causing glucose intolerance. 23 MPA has been shown to decrease bone mineral density without altering carbohydrate tolerance, with an increase in levels of insulin and LDL-cholesterol and a decrease in HDL-colesterol. 24
Among the subcutaneous implants are levonorgestrel (Norplant®) and etonogestrel (Implanon®), with effectiveness of five and three years respectively. Norplant®, as well as other hormone contraceptives with progestin, were found to have altered minimally the carbohydrate metabolism, increasing both glycaemic (12.3%) and insulin (37.7%) areas after oral glucose tolerance testing, although such increases did not have clinical relevance. 25
Insulin susceptibility, assessed by insulin tolerance testing, showed no significant changes with the use of such implants. 26 The meta-analysis by Kahn et al that reviewed 25 studies of women from developing countries without diabetes and not obese who were treated with progestin (intramuscular or subcutaneous implants) confirmed the existence of impaired carbohydrate tolerance. 27 In eight of the studies that included the use of levonorgestrel or MPA, the response to an oral glucose tolerance test showed increased concentrations of insulin. In three others, with the use of injection MPA, an increased early insulin response was observed following intravenous glucose challenge, which may reflect an underlying insulin resistance. In this sense, there are isolated reports of decreased insulin sensitivity after the use of subcutaneous implants of progestins, as assessed by hyperglycaemic clamp or with minimal Bergman model.28,29 The relative weight gain resulting from the use of such contraceptives was considered among the mechanisms that explain this possible insulin resistance. 27
An epidemiological study conducted in a cohort of 7977 non-obese women from developing countries found an increased risk of diabetes (relative risk [RR] 2.4, 95% CI 0.7–8.1) among women using levonorgestrel implants compared with women treated with non-hormonal intrauterine devices (IUD) or surgical sterilization. 30 In addition, a case-controlled study conducted in Navajo women, a special diabetes mellitus-prone population, showed that depot MPA was associated with a greater risk of diabetes compared with COC use only (OR 3.8, 95% CI 1.8–7.9). 31 The excess risk persisted after adjusting for body mass index (OR 3.6, 95% CI 1.6–7.9). In addition, users of depot MPA were also more likely to develop diabetes than patients who had never used hormonal contraception (OR 2.4, 95% CI 1.4–3.6).
The use of transdermal patches with EE and noregelstromin does not appear to have adverse effects on carbohydrate tolerance, despite releasing more estrogen than low dose COCs. 32 As regards to the use of vaginal contraceptive ring (NuvaRing®), which releases constant amount of EE and etonogestrel, appears to have minimal impact on the carbohydrate metabolism. 33
Finally, the use of levonorgestrel-releasing IUD (Mirena®) was not associated with alterations in lipid metabolism or blood pressure, having minimal (elevated fasting plasma glucose) or absent impact on carbohydrate metabolism. 34
Hormonal Contraception in Women with Prior History of Gestational Diabetes Mellitus
The presence of GDM is a risk factor for subsequent development of DM, especially type 2 DM. In the immediate postpartum period, about 5% of women with previous GDM develop DM, and about 20% experience some degree of glucose metabolism alterations (hyperglycaemia and/or carbohydrate intolerance).35,36 In all women with previous GDM, and especially in the group with postpartum glucose metabolism alteration, it is essential to provide the means necessary to prevent the development of subsequent DM. Therefore, it is imperative to control risk factors for diabetes, such as obesity and development of new pregnancies. Obesity prevention is achieved through diet and the practice of regular exercise. With regard to new pregnancies, it is essential to use appropriate contraception that does not enhance the already substantial risk of developing either overt DM or metabolic syndrome and associated sequelae.11,13,37
Initial studies conducted by Skouby et al showed that after administration of triphasic COC for 2 to 6 months in women with prior GD, no significant impact on either carbohydrate or lipid metabolisms was observed, specifically as to the binding of monocyte or erythrocyte insulin receptors. 38 In addition, the same research group found, after the same treatment and by using an euglycaemic clamp, a significant decrease in insulin sensitivity without alteration in glucose tolerance. 39
In another study by Kung et al, 26.7% of the study women with prior history of GDM treated with a triphasic COC developed impaired glucose tolerance along with an increase in insulin response. However, impaired glucose tolerance reverted to normal after treatment cessation. 40 Subsequently, Kjos et al analyzed the incidence of DM in women with prior history of GDM treated with three different contraceptive treatments: non-hormonal contraception; EE 35 μg+norethindrone, and 35 μg EE+levonorgestrel. Similar percentages of DM—17%, 15%, and 20% respectively—were found among the three groups. 41 The same author analyzed a large cohort of Hispanic women with prior history of GDM treated with either a non-hormonal form of contraception or low-dose oral contraceptives beginning in the immediate postpartum period and followed for seven and a half years. No differences in cumulative incidence of diabetes were found among both groups. 42 In this study, the group of nursing women was treated initially with norethindrone alone and subsequently with COCs when breastfeeding ended. It was found that the incidence of DM was three times higher than in the group treated with COCs uninterruptedly (RR: 2.87; 95% CI: 1.5–5.2). Therefore, the authors suggested the use of progestin alone should be prescribed cautiously in breast-feeding Latina women with recent GDM due to the low rate of estrogen during this period that could potentiate the effect of progestin agents on induction of insulin resistance and β-cell dysfunction (underlying phenomena of GDM). However, the recommended hormonal contraception during lactation is the use of progestin agents alone.6,12
Another study conducted in the United States compared the effect of COC use and MPA use in 526 Hispanic women with previous GDM (without diabetes in the immediate postpartum) who were followed for a minimum 12 months (maximum 9.2 years). The annual incidence of DM was 12% and 19% respectively, with an unadjusted hazard ratio (HR) of 1.58 (95% CI 1.0–2.5) for MPA compared with COCs. After adjustment for baseline body mass index, presence of breastfeeding, family history of diabetes, HDL-cholesterol, triglycerides, and weight gain, the HR decreased to 1.06 (95% CI 0.58–1.95). 43 The same authors conducted another observational study in 972 non-diabetic, normotensive, postpartum Latina women with prior GDM who during the postpartum period were subjected to non-hormonal contraception or hormonal contraception with a COC or depo-MPA. It was found that after one or two years of follow-up, the depo-MPA treated group showed a greater increase in weight than the other two groups, while changes in blood pressure and lipid profile were minimal. 44
Finally, in the study by Nelson et al that followed 189 women with prior history of GDM for one year, a worsening in glucose tolerance of 22%, 35%, and 34% respectively, was observed among women receiving non-hormonal contraception, COCs, or progestin alone (P value no significant). However, the influence of other simultaneous factors such as breastfeeding was not analyzed. 45
Hormonal Contraception in Diabetic Women without Vascular Complications
Several studies have analyzed the metabolic impact of oral hormonal contraceptive use in women with diabetes, although most of them included small numbers of patients and, therefore, the results are highly variable.46,47 Radberg et al examined the changes in both lipid and glucose metabolism in 23 insulin-dependent diabetic who were randomized to lynestrenol (0.5 mg) or lynestrenol (0.5 mg) + EE (50 μg) exchanging treatments after six months. 47 No changes in blood glucose levels and body weight in either group were observed, although the group receiving COC required increasing insulin. Regarding lipid profiles, use of lynestrenol only was associated with a decrease in serum cholesterol, triglycerides, and phospholipids, while the COC treatment was associated with a significant increase in serum triglycerides. Similarly, Skouby et al examined changes in the metabolism of glucose and lipid metabolism in 27 insulin-dependent women in relation to three types of COC or norethindrone alone. 47 After six months of follow-up, no differences were observed among the four groups regarding fasting glucose, percentage of HbA1c, insulin requirements, blood pressure, body weight, free fatty acids, LDL-cholesterol or HDL-cholesterol/total cholesterol ratio. Likewise, in a one-year follow-up study conducted in women with type 1 diabetes who used a COC treatment with EE 30 and gestodene 75 μg, Petersen et al found no significant changes in either carbohydrate metabolism or lipid control. 48
Regarding the use of non-oral hormonal contraceptives, Gershberg et al analyzed a group of eight women with type 2 DM undergoing diet alone who received MPA treatment. After three months of follow-up, an increase in blood glucose values and a decrease in insulinaemic response after oral glucose overload was observed. 49 Diab and Zaki analyzed the effects of long-term intake of low-dose COC, MPA, or levonorgestrel implants versus copper IUD on glycaemic control and lipoprotein metabolism in 80 diabetic women. The results showed that COCs produced a greater disruption on lipid pattern (elevated triglycerides and HDL-cholesterol and decreased LDL-cholesterol) compared with MPA (increased cholesterol and LDL-cholesterol and decreased HDL-cholesterol), while only mild alterations were found with the use of levonorgestrel. 50 In another recent study by Vicente et al of 23 women with diabetes on insulin therapy, after two years of use of etonogestrel implant, no evidence of impaired control of the carbohydrate and lipid metabolism or aggravation of vascular lesions was observed. 51 Regarding the effect of levonorgestrel IUD compared with copper IUD, a study conducted in 59 women with type 1 DM showed that after six weeks of use, no difference in relation to carbohydrate metabolism (fasting glucose, HbA1c, or dose of insulin) was observed between the two groups. 52 In another study by Grigoryan et al conducted in perimenopausal women that compared the use of levonorgestrel IUD and various types of COCs, it was observed that while COC treatments had an unfavorable effect on lipid profile, platelet activation, and coagulation parameters, levonorgestrel IUD had a neutral effect on coagulation and fibrinolisis. 53
Given the risk of diabetic women developing endometrial cancer and because of the profound anti-proliferative of levonorgestrel IUD, which reduces the risk of endometrial hyperplasia and adenocarcinoma, this contraceptive device may have a protective effect against the development of endometrial hyperplasia and adenocarcinoma. 54 Regarding the use of the vaginal ring (NuvaRing®) in women with type 1 DM, no metabolic changes have been reported, and, therefore, this birth control method could be used in diabetic patients. 55
Hormonal contraception in Diabetic Women with Vascular Complications or cardiovascular Risk Factors
The diabetic woman is prone, due to the duration of their disease and the poor metabolic control, to develop both microvascular (retinopathy and nephropathy) and macrovascular complications (atherosclerosis myocardial, cerebral and peripheral vascular disease). It is also common to find the presence of cardiovascular risk factors (obesity, lipids, and hypertension) especially in type 2 DM patients. Given these circumstances, before selecting the hormonal contraception, it is imperative to analyze the possible adverse effect on the aforementioned risk factors, as well as its impact in the short- and long-term development and progression of vascular complications.
Petersen et al evaluated established cardiovascular risk factors within lipoprotein metabolism, haemostasis, and endothelial function in 35 women with type 1 DM treated for one year with a monophasic COC (EE 30 μg + gestodene 75 μg) or with non-hormonal contraception. In the monophasic COC treatment group, an increased activity of factor VII clotting activity without modification of the fibrinolytic system was noticed. 56 Compared with women without diabetes, the use of COCs in women with diabetes have shown to increase the risk for developing acute myocardial infarction and cerebral thromboembolic attacks, although the presence of diabetes did not significantly increase the risk for developing venous thromboembolism.57–59
Regarding the development of retinopathy in insulin-dependent DM, the study of Klein et al, that followed 384 women of 14 to 30 years of age for four years showed that neither past nor present use of oral contraceptives nor the number of years of oral contraceptive use influenced retinopathy severity. 60 Likewise, a retrospective analysis conducted by Garg et al evaluated in a case-control study the effects of oral contraceptives as a possible risk factor for early diabetic renal and/or retinal complications in 43 juvenile insulin-dependent diabetic women who used oral contraceptives for an average of 3.4 years. The results showed that the use of oral contraceptives did not increase the risk for the development of early diabetic retinopathy and/or nephropathy. 61 Klein et al evaluated whether the use of exogenous estrogen was associated with changes in the severity of diabetic retinopathy and the incidence of macular edema. 62 It was observed after 10 years of follow-up of two groups of DM patients, 576 juvenile-onset group (<30 years) and 979 of older-onset group (≥30 years), that the use of oral contraceptives or hormone replacement therapy was not related to the severity of retinopathy and the incidence of macular edema. The same authors, from a similar population of 2990 women with DM followed for 12 years, found that the use of oral contraceptives or hormone replacement therapy is unrelated to cardiovascular mortality. 63
Concerning the influence of hormonal contraception on the presence of diabetic nephropathy, contradictory results have been reported. Thus, Ahmed et al conducted an observational study in 114 women with type 1 DM. After a mean follow up of 20.7 years, the incidence of microalbuminuria was significantly higher in the group using COCs compared with the control group (18% vs. 2%), and OC use was also a predictor for the development of macroalbuminuria (RR 8.9, 95% CI 1.8–44.4). 64 Similarly, the Prevention of Renal and Vascular End Stage Disease cohort study that included 4301 women without diabetes, found that regular and long-term use of COC with high doses of estrogen and second generation progestin was associated with an increased risk for microalbuminuria. 65 On the contrary, the study by Coustaco et al study that followed 216 women with type 1 DM found a protective effect of COC use in the clinical development of diabetic nephropathy. 66
Prevalence of Hormonal Contraception use among Women with Diabetes
The use of contraception by women with diabetes does not follow any particular pattern, with wide differences between countries. Thus, in a secondary analysis of the 2004–2005 Pregnancy Risk Assessment Monitoring System database conducted in the United States (in Michigan and Oregon) by Beydoun et al, no difference in the percentage of use of hormonal and non-hormonal contraceptives was observed among primiparous women without diabetes and those with a prior history of GDM, although there was a higher frequency of female sterilization and a lower use of depot-MPA among the group of patients reporting GDM diagnosis. 67 The review conducted by Napoli et al in 667 Italian diabetic women (type 1 DM or type 2 DM) found that 30.4% of women used hormonal contraception, 12% used an IUD, 47% used natural or barrier methods, and 10.7% used no method contraception. The percentage of women using oral contraceptives differed between women with type 1 DM and type 2 DM. 68
In a survey conducted by Manolopoulos et al among Greek gyneocologists, the authors reported that COCs were recommended as a contraceptive method for young women with type 1 DM by 14.3% of the physicians, while the minipill with progestin was recommended by 5.7% of the participanting gynecologists. 69 In similar study conducted among German gynecologists, COCs and the minipill were recommended by 66.9% and 3.5% of the gynecologists surveyed. 70 Regarding type 1 DM patients who smoke, data from both surveys showed a decreased in the use of hormonal contraception and an increase in the use of male condoms, barrier methods, and IUDs.69,70 More recently, Shaw et al reviewed the data form the United Kingdom General Practice Research Database that includes 947 cases of type 1 DM and 365 cases of type 2 DM patients respectively. 71 A lower frequency of use of hormonal contraception was found among women with diabetes compared to women without diabetes. Women with type 1 DM most frequently used COCs compared with progestin alone, while women with type 2 DM used COCs less frequently. Depot-MPA was more frequently used by diabetic women compared with non-diabetic women. Considering that diabetic women should avoid pregnancy until good metabolic control has been achieved, should these women use more hormonal contraception, the number of pregnancies under less appropriate conditions would be fewer. Due to the low risk of hormonal contraception in these diabetic women, it appears suitable to increase its use.
Recommendations of Hormonal Contraceptive Methods for Women with Diabetes
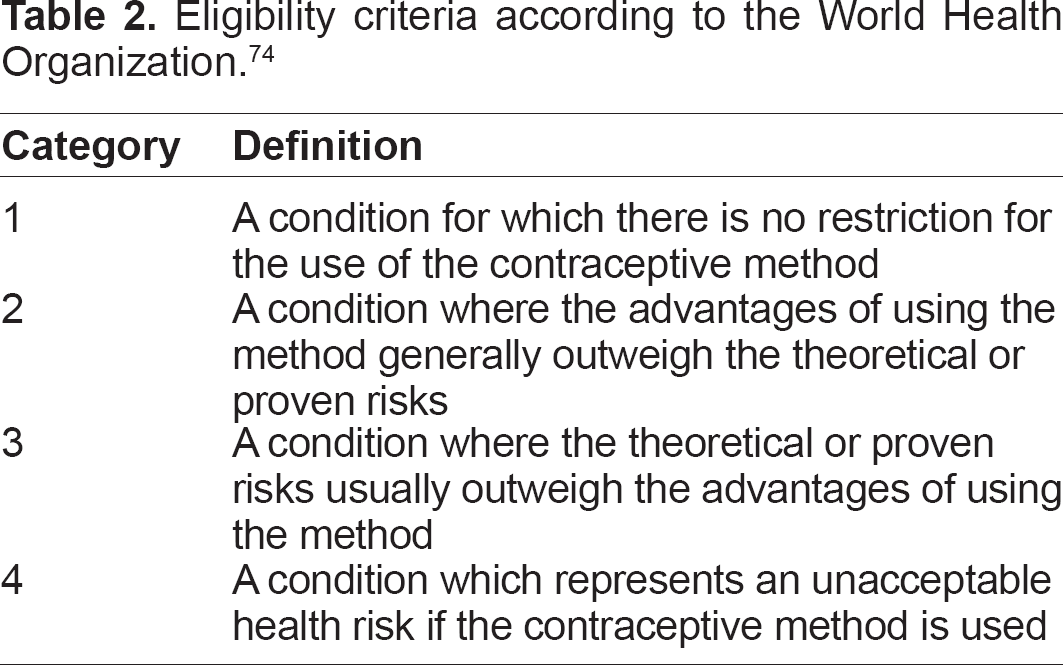
When establishing general guidelines regarding the recommended use of hormonal contraceptives in women with diabetes, there are different proposals from different organizations to consider, the most widely used, being the protocol proposed by the World and Health Organization (WHO) in 2009.5,12,72
COC has a varied impact, albeit with minor clinical significance, on lipid profile, depending on the dose of estrogen as well as the dose and type of progestin used. COC may slightly increase blood pressure as well as the risk of myocardial infarction and ischemic stroke, which is partly conditioned by other concomitant factors such as age, smoking habit, estrogen dose, type of progestin, and presence of cardiovascular risk factors (dyslipidaemia, diabetes, and hypertension).12,13,58,72 It should be noted, however, that given the low frequency of cardiovascular events in healthy women of childbearing age, the risk attributable to use of these drugs would be low.
As discussed above, it has been proven that the use of progestin alone has a barely significant effect on carbohydrate and lipid metabolism, while no substantial effect on blood pressure and clotting factors has been identified. In addition, no significant risk with respect to the development of cardiovascular events (myocardial infarction, ischemic stroke) or venous thromboembolism has been reported.73–75 It is remarkable, however, that treatment with progestins alone has several minor complications such as poor control of the menstrual cycle, development of follicular cysts, and potential amenorrhea due to endometrial atrophy. 76
COC with low doses of estrogen (20–35 μg EE) and third-generation progestins (desogestrel, gestodene) can be safely used in diabetic patients (type 1 DM and type 2 DM). COCs should not be used in diabetic patients with any of the following risk factors: hypertension, smoking, age greater than 35 years, uncontrolled hyperlipidaemia, cardiovascular complications related to diabetes, or thrombophilic predisposition. In such cases, a low-dose progestin alone should be recommended.11,13
According to the American Congress of Obstetricians and Gynecologists (ACOG), use of COCs should be limited to diabetic patients that do not smoke, are under 35 years of age, and have no evidence of hypertension, nephropathy, retinopathy, or other vascular diseases. 13 The use of progestin alone is recommended for the following: women who have migraine, especially those with focal neurological signs; women over 35 years of age who smoke or are; women with prior history of thromboembolic disease; women with high blood pressure who have vascular disease or are older than 35 years of age; women with systemic lupus erythematosus with vascular disease, nephritis, or anti-phospholipid antibodies; women less than 3 weeks postpartum; and women with hypertriglyceridemia; coronary heart disease; congestive heart failure, or cerebrovascular disease.
As shown in Tables 2 and 3 and according to WHO guidelines, the different types of combined contraception (COCs, patches, vaginal rings, and injections) as well as progestin alone (oral, subcutaneous implants, injectables, and IUDs) are classified in category 1 for women with prior history of GDM. In diabetics (both insulin and non-insulin dependent) without vascular complications, all types of hormonal contraceptives are included in category 2, while in diabetic women with disease lasting more than 20 years or those with neuropathy, retinopathy, nephropathy, or vascular complications, combined contraception is included in category 3 or 4 with the recommendation to use of progestin alone (category 2), except for intramuscular use (MDPA and NET-EN) in the presence of nephropathy (category 3). Notwithstanding the foregoing, in those diabetic patients who smoke, in those over 35 years of age, in those who have high blood pressure, and in those with multiple cardiovascular risk factors, history of deep vein thrombosis, or migraine progestin alone, the lowest dose should be recommended (Table 3).
Eligibility criteria according to the World Health Organization. 74
Eligibility criteria for diabetic patients according to WHO guidelines. 74

As for the hypothetical use of hormonal contraception during lactation, while progestins alone do not seem to affect the volume of milk secretion, it has been determined that the estrogen component of COCs may reduce the volume and mineral and caloric milk content, although there seems to be no impact on the further development of the child.77,78 ACOG recommends that COCs should not be used in non-lactating women up to 4 weeks postpartum and should not be used as first choice in nursing women. 13 It is preferable to use oral progestins and DPMA, which can be successfully initiated after six weeks postpartum in breastfeeding women and immediately postpartum in the non-lactating women.
WHO guidelines establish that during the breastfeeding period, the use of progestins alone is recommended although no hormonal contraceptive should be used during the first six weeks postpartum (category 3 or 4). These precautions apply to women with diabetes, although it is important to highlight that the use of progestins alone during the lactating period in Latina women with prior GDM showed an increased risk for the development of subsequent diabetes compared with COCs. 41
Footnotes
Author Contributions
LFP, AC, IC, MAB, ML and IL conceived the article, reviewed the literature and analyzed the evidence. LFP and IL wrote the first draft of the manuscript. All the six authors made critical revisions, agree with manuscript and approved the final version of the manuscript.
Funding
The authors received funding from Schering Plough Spain to translate the original manuscript written in Spanish to English.
Competing Interests
IL has received payment for board membership, grants and speaking from Bayer, Teva, and MSD, and for development of educational presentations from Teva and MSD. Other authors declare no competing interests.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.