
Abstract
Background
In IVF, Luteal phase support is usually performed using vaginal progesterone. A part of patients using this route reports being uncomfortable with this route. We tried to study whether the rectal route could be an effective alternative and associated with less discomfort.
Patients and Methods
A prospective randomized controlled study. All patient were eligible for IVF treatment for infertility. After oocyte pickup, 186 patients were allocated to one the following protocols for luteal phase support: (i) rectal pessaries group: natural progesterone pessaries administered rectally 200 mg three times a day, (ii) vaginal pessaries group: natural progesterone pessaries administered vaginally 200 mg three times a day), and (iii) vaginal capsules group: natural micronized progesterone capsules administered vaginally 200 mg three times a day. On the day of pregnancy test, patients were asked to fill in a questionnaire conducted by an investigator in order to assess the tolerability and side effects of the LPS treatment taken. The primary endpoint was the occurrence of perineal irritation.
Results
Fifty eight patients were assigned to the rectal pessaries group, 68 patients to the vaginal pessaries group, and 60 patients to the vaginal capsules group. All patients adhered to their allocated treatment. Implantation and clinical pregnancy rates per transfer did not differ between the three groups. Perineal irritation, which was our primary endpoint, was the same for all the three groups (respectively 1.7 % versus 5.9 % versus 11.7%). Regarding the other side effects, more patients experienced constipation and flatulence with the rectal route, whereas more patients reported vaginal discharge in the vaginal capsules group.
Conclusion
Rectal administration for luteal phase support is effective and well accepted alternative to vaginal route.
Introduction
It is well established that the luteal phase is defective during stimulated in vitro fertilization (IVF) cycles due to a low progesterone production by the corpus lutea. 1 This phenomenon is probably due to the supraphysiological concentrations of estradiol produced by the numerous corpus lutea during the early luteal phase. 2 Therefore, luteal phase support (LPS) is compulsory during IVF cycles. Both human chorionic gonadotropin (HCG) and progesterone are effective for LPS. However, HCG is associated with an increased risk of ovarian hyperstimulation syndrome. 3
During IVF cycles, similar outcomes are observed for progesterone using either the intramuscular or the vaginal route; however, intramuscular progesterone injections are associated with more side effects. The vaginal route seems to be the preferred option. Different forms are available for vaginal progesterone: gel, capsules, pessaries, and inserts. Even though the vaginal route is more convenient, some patients may feel uncomfortable using it. This is mainly due to the vaginal discharge that occurs after use, which could end up in perineal irritation. Patients may also feel some anxiety related to a possible lack of efficiency due to the vaginal loss of the product.
Although they both contain the same active ingredient (natural progesterone) and are administered vaginally, capsules and pessaries are different from the pharmacogalenic point of view. This implies that they could show a difference in their effectiveness and their associated side effects. Natural progesterone pessaries can be administered rectally, and despite the availability of this form of administration on the market, there are very few related studies on its use for LPS indication.4–6
We designed a prospective study to compare the effectiveness and acceptance of three different forms of progesterone used for LPS: rectal or vaginal natural progesterone pessaries (Cyclogest®) and vaginal capsules of micronized progesterone (Utrogestan®).
Patients and Methods
Inclusion Criteria
All patients aged less than 39 years undergoing IVF treatment with no history of repeated embryo implantation failure were included in the study. Patients who did not have an embryo for transfer were excluded.
All included couples had the standard fertility assessment prior to their IVF treatment: a hormonal ovarian reserve assessment (day 3 basal follicle-stimulating hormone [FSH] and E2) for the female partner, a recent semen analysis for the male partner (less than one year prior to treatment), and a complete infection screening. All female patients also had a uterine cavity assessment by hysterosalpingography or hysteroscopy. The local institutional review board approved the study. The study complied with the principles of the Declaration of Helsinki. Patients gave their informed consent to participate in the research.
Patients and IVF Procedure
All patients underwent pituitary desensitization using Triptorelin (Decapeptyl®, Ipsen). Two desensitization protocols were used: flare-up protocol where patients were given Triptorelin 0.1 mg daily from the first day of their menstrual cycle or long agonist protocol where patients were given the same dose of Triptorelin from the 21st day of their previous menstrual cycle. Ovarian stimulation was performed using recombinant FSH (Gonal-F®, Merck Serono) or HMG (Menopur®, Ferring) and monitored according to follicular size growth and plasma estradiol levels. When three follicles had reached a diameter of at least 17 mm, ovarian hyperstimulation was stopped and HCG (Ovitrelle®, Merck Serono) was administered. Oocyte retrieval was performed 36 hours later. Intracytoplasmic sperm injection was the fertilization method for all the cycles included. Embryo transfer was performed two or three days following egg retrieval. At this stage, consented patients who had embryos available for transfer were randomly assigned (by drawing sealed envelopes) to one among three protocols for LPS: rectal pessaries group: natural progesterone pessaries administered rectally 200 mg three times a day (Cyclogest® 200, Actavis), vaginal pessaries group: natural progesterone pessaries administered vaginally 200 mg three times a day (Cyclogest® 200, Actavis), and vaginal capsules group: natural micronized progesterone capsules (Utrogestan®, Besins International) administered vaginally 200 mg three times a day. Each patient was individually instructed by a nurse on how to administer the LPS treatment correctly starting on the day of embryo transfer.
Embryo transfer was carried out using Frydman flexible catheter (CDD) or a rigid catheter (CDD). A serum pregnancy test was performed 15 days following embryo transfer. The pregnancy test was considered as positive when serum βHCG exceeded 50 mIU/mL and gestational(s) sac(s) observed on ultrasound 10 days after the pregnancy test.
On the day of pregnancy test, patients were asked to fill in a questionnaire conducted by an investigator in order to assess the tolerability and side effects of the LPS treatment taken. The investigator (SS) had no knowledge of the protocol of LPS treatment. The questionnaire consisted of questions relating to the occurrence (during the 15 days of progesterone administration) of nausea or vomiting, constipation, diarrhea, flatulence, abdominal pain, pelvic or epigastric pain, vaginal discharge, perineal irritation and pruritus, vertigo, headache, and drowsiness. All questions were answered by “yes” or “no”.
Perineal irritation was defined as the perception by patient of a vulvar erythema. The presence of vaginal discharge was recorded if the patient reported the presence of residues of progesterone or any other type of discharge.
Patients who were pregnant were followed up by a telephone interview. They were asked about the pregnancy development until the eighth gestation week and about any vaginal bleeding occurrences. And the primary objective was to know whether the patient reported any perineal irritation.
Statistics
Assuming that 20% of patients in the vaginal pessaries group 7 will experience perineal irritation versus 2% in the rectal pessaries group, 6 the sample size required is 60 in each arm to be able to make a test with 0.05 significance and a power of 90% to the study. χ 2 test was used to compare qualitative variables. Student's t-test was used to compare quantitative variables. P-value ≤0.05 was considered as statistically significant. SPSS 17.0 (IBM) software was used for statistical analysis.
Results
A total of 278 patients were eligible for enrollment and were started on ovarian stimulation. Ninety two patients were excluded as no embryos were available for transfer or embryos were available, but a decision not to transfer the embryo(s) was made for different reasons (Fig. 1).
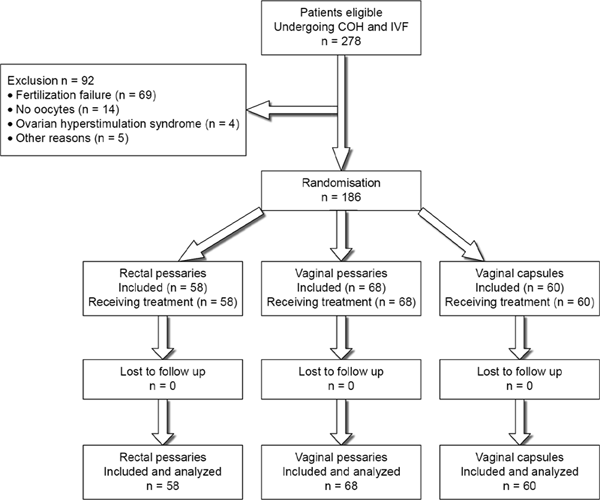
Flowchart of patients included in the study.
One hundred and eighty six patients were randomly allocated to one of the three arms. Fifty eight patients were assigned to the rectal pessaries group, 68 patients to the vaginal pessaries group, and 60 patients to the vaginal capsules group. All patients adhered to their allocated treatment.
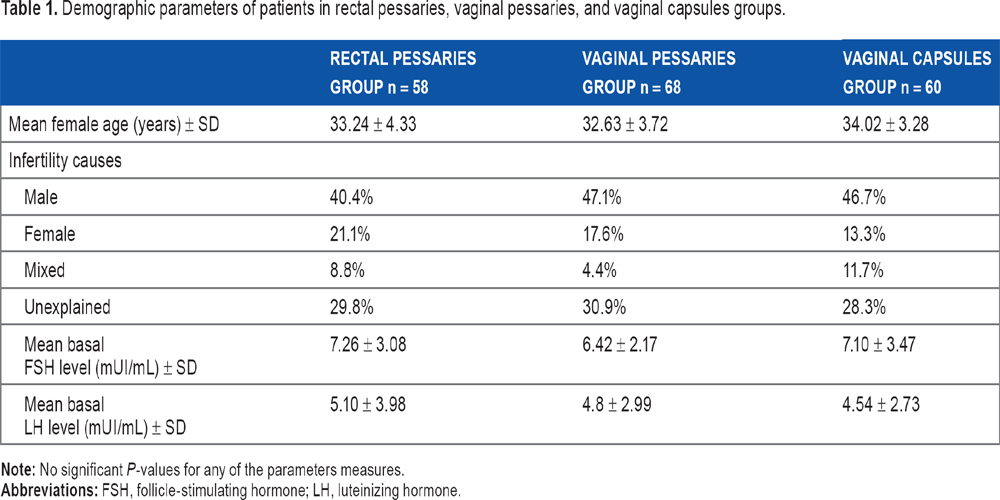
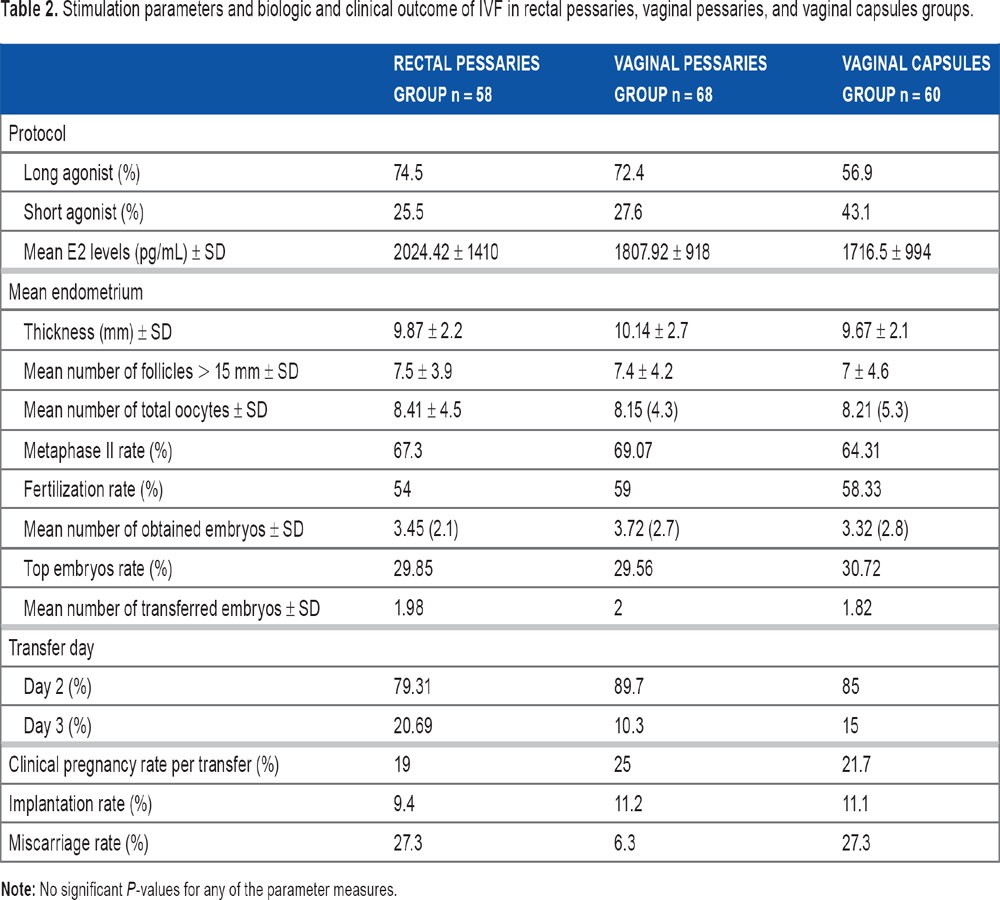
We observed no significant difference in patients' characteristics (age, basal FSH, luteinizing hormone levels, and infertility diagnosis) between the three groups (Table 1). All three groups showed no significant difference concerning ovarian stimulation parameters or IVF outcomes (Table 2). Implantation and clinical pregnancy rates per transfer did not differ between the three groups.
Demographic parameters of patients in rectal pessaries, vaginal pessaries, and vaginal capsules groups.
Stimulation parameters and biologic and clinical outcome of IVF in rectal pessaries, vaginal pessaries, and vaginal capsules groups.
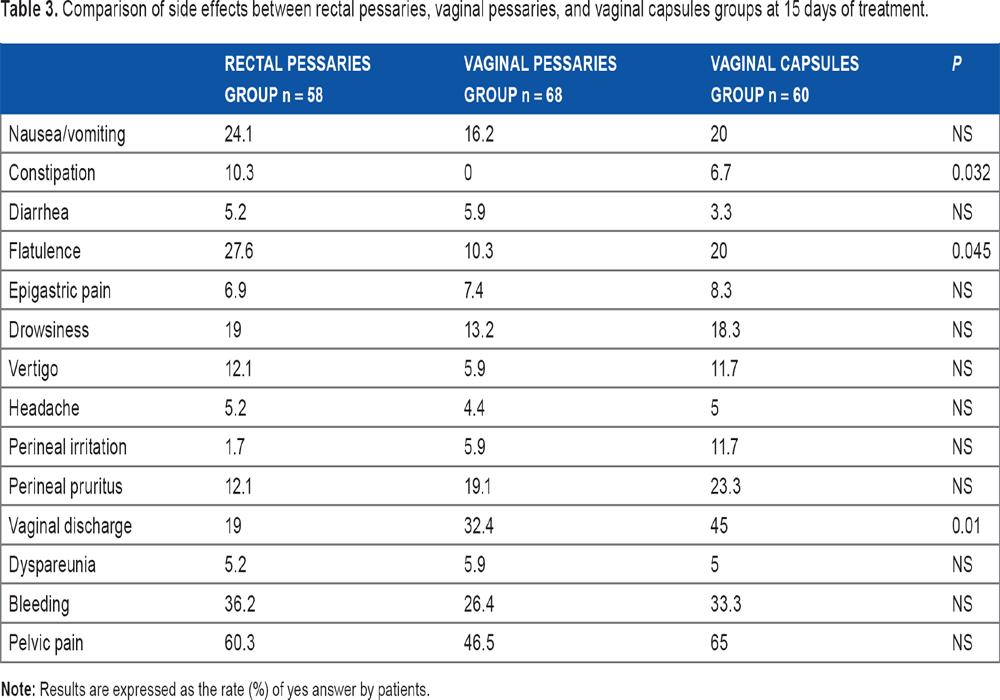
Perineal irritation, which was our primary endpoint, was the same for all the three groups (Table 3). Regarding the other side effects, more patients experienced constipation and flatulence with the rectal route, whereas more patients reported vaginal discharge in the vaginal capsules group (Table 3).
Comparison of side effects between rectal pessaries, vaginal pessaries, and vaginal capsules groups at 15 days of treatment.
Discussion
The vaginal route is the mostly used route for LPS 8 worldwide. It provides ideal uterine hormone concentrations, leading to a good implantation rate and favorable IVF outcomes. 9 There are various vaginal forms of progesterone: capsules, pessaries, gel inserts, and recently, a vaginal ring. The vaginal route, however, is not free of side effects and some patients may experience vaginal discharge causing perineal irritation.6,10 Several studies have reported this side effect in 15%-20% of IVF cycles.6,7,11 Some patients may also experience discomfort with the vaginal insertion of capsules for cultural or emotional reasons, especially when a pregnancy occurs. Finally, some patients may have some concerns about a possible lack of efficiency, due to the loss of the product.
The rectal route may represent an effective alternative to vaginal P pessaries, and natural P pessaries (Cyclogest®) can be used both vaginally and rectally. Both have demonstrated similar pregnancy rates. 6 Side effects have shown to be different, with significantly more perineal irritation with the vaginal route (21.3% vs. 2.2%), but significantly more tenesmus (35.1% vs. 21.1%) and rectal itching (26.7% vs. 2.8%) with the rectal route. 6 These findings were confirmed in our study. Rectal and vaginal administration of pessaries and vaginal capsules showed similar outcomes: 19%, 25%, and 21.7%, respectively, for pregnancy rates per embryo transfer. Implantation rates were also comparable. It should be noted, however, that due to the sample size this study was not powered enough to detect a significant difference in IVF outcomes.
As expected, our study confirmed that the use of P pessaries resulted in different side effects depending on the route used for treatment: more vaginal discharge in the vaginal route and more constipation and flatulence in the rectal route. There was no difference with regard to perineal irritation between both routes, which was our primary endpoint. To our knowledge, this is the first study that compared micronized natural P capsules and natural P pessaries given vaginally. Interestingly, our study showed that the highest rate of vaginal discharge is observed with micronized P vaginal soft capsules (Utrogestan®) (45%). This may be explained by the galenic formulation and excipients used in these pharmaceutical forms. In fact, soft vaginal capsules contain active ingredients suspended in a liquefied vehicle in contrast to pessaries, which are more of a solid form. Finally, we also observed a lower miscarriage rate in the vaginal pessaries group (6.3%) compared with vaginal capsules group (27.3%) and rectal pessaries group (27.3%), although it did not reach statistical significance.
To our knowledge, our study is the first to compare the different options for LPS. It is a randomized controlled study, but it has some weaknesses such as the subjective report of side effects by the patients (no clinical examination). The overall degree of patient satisfaction has not been evaluated.
Conclusion
We did not demonstrate any difference regarding perineal irritation with any of the forms or routes assessed, despite a higher rate of vaginal discharge in the vaginal capsules group. More constipation and flatulence were associated with the rectal route. We observed similar outcomes regarding pregnancy and implantation rates, even if the study was not powered enough to detect a significant difference in such parameters. Rectal administration of progesterone is as effective and safe as the vaginal route.
Footnotes
Author Contributions
Conceived and designed the experiments: MK. Randomized the patients: KKB. Analyzed the data: MK, SS. Wrote the first draft of the manuscript: MK, SS, MRK. Contributed to the writing of the manuscript: MB, AZK. Agree with manuscript results and conclusions: KKB, GM, HEC, AZ. Jointly developed the structure and arguments for the paper: MBou, MRK. Made critical revisions and approved final version: FZ, AZ. All authors reviewed and approved of the final manuscript.