
Abstract
Inadequate patient handoffs have been an area of focus for patient safety improvement. Insufficient communication and risks or “shortcuts” taken by staff members during handoffs could negatively affect the safety of patients in a department of obstetrics and gynecology. Other factors that contribute to inadequate handoffs are the caregiver feeling fatigued or stressed, level of urgency, volume of information, language barriers, noise, lighting, ambiguity of describing treatment, not allotting enough time for questions asked, and/or interruptions from other staff members. There have been several methods developed for improving the handoff process, such as the mnemonic devices SBAR, SHARQ, I PASS THE BATON, and the 5 P's. A new method for improving the quality of patient handoffs has been developed and presented in this article. It is a mnemonic device entitled “HANDOFFS”. It covers key aspects of what a handoff process should entail. Teamwork is essential to effective communication, and by using a mnemonic such as this, team members can work together in a more positive and accessible environment that will result in improved patient safety.
Introduction
Patient handoffs are an area of importance in departments of obstetrics and gynecology, as it is a key part of patient safety in general. A patient handoff is when the responsibility of a patient is transferred from one caregiver to another or from one department to another. 1 The primary objective of a patient handoff is to provide accurate, complete, and unambiguous patient specific information in a timely manner. 2 When this information becomes inaccurate, and/or unclear during a transition, the patient's safety may be at risk for an adverse event to occur.
Patient treatment begins with the acquisition of a new patient's medical information. If things go smoothly during this transition, it allows for a safer treatment of the patient overall. 3 One of the major causes for inadequate patient handoffs is inadequate communication, including handoffs in the specialty of obstetrics and gynecology. 4 Handoffs occur when a patient is transferred to a new location or to a new care provider and/or care providing team. The patient could be transferred to a labor and delivery unit from an ante-partum unit, from a labor and delivery unit to a post-partum floor, from the labor and delivery unit to a rapid response team, or between different departments in the hospital such as from the Emergency Department to the Operating Room. Obstetrical emergencies that could occur during delivery that would require handoffs to others include circumstances such as a patient experiencing an obstetrical hemorrhage, the rare case of a prolapsed umbilical cord, uterine rupture, and the incident of shoulder dystocia, among others. 5 Handoffs occur between obstetrician-gynecologists, certified nurse midwives, nurses, residents, anesthesiologists, neonatologists, and any other staff members involved with a particular patient. It is not rare for a patient to have been seen regularly throughout her pregnancy by her primary obstetrician-gynecologist, and then be cared for during delivery by a different caregiver, such as a laborist. Also, some obstetricians will be faced with several deliveries at the same time, sometimes between two different hospitals, and be scheduled for the office at the same time. 4 This is a circumstance where problems may occur because when a patient chart is not immediately available and her physician is not on call, then vital information may be delayed to the new patient care team, which could potentially result in a compromise of the patient's safety. In this manuscript, we review patient handoffs, with an orientation towards obstetrics and gynecology teaching services.
Resident Experience with Handoffs
Residents are working shorter shifts, and fewer hours per week. 6 On July 1, 2003, the Accreditation Council for Graduate Medical Education (ACGME) limited the workweek for all residency programs to 80 hours. 7 Prior to that, some residents, such as general surgery residents, were working up to 90–110 hours per week. 6 The 80 hour work week is a significant decrease for a number of reasons. This decrease lessened time for hands-on education, increased the number of shift changes, and, potentially, created up to 300 patient handoffs in a month for a given resident. 8 The increase in patient handoffs results in increased opportunity for medical errors and miscommunication between caregivers to occur. Residents have to keep up-to-date information about each patient that they are covering during their shift. They then have to relay this information on to the next resident who will assume the responsibility for the patient. Perhaps due to the number of patient handoffs that occur within one resident's rotation, some residents feel that they are doing all their handoffs accurately. Handoffs could be done poorly, and residents may not recognize these errors and inadequacies. This may be due to the incoming shift dealing with the mistakes, the residents perhaps not associating patient harm with a handoff error, or because they have not experienced a prior complication due to a problematic handoff. Thus, the decrease in the residents' workweek hours may contribute to a potential gap in quality of patient handoffs.
Residents of the medicine and surgical departments at the Massachusetts General Hospital in Boston were asked to fill out an anonymous survey about patient handoffs that occurred during their most recent rotation. 8 Rotations average about one month at the Massachusetts General Hospital. Before residents were given the survey, they were given definitions for minor and major patient harm. Minor patient harm was when a patient was not significantly affected by the error, but could have prolonged hospital stay or a slightly worsened condition because of it. Major patient harm consisted of significant effects to the patient's health, such as their condition severely worsening, organs being harmed, and, in some cases, death. 8 The authors reported that 67.6%, or 161 out of 238, physicians responded to the survey. More than half of the physicians surveyed (59%) said at least one patient or more had been harmed by handoff errors within a rotation (12.3% reported that this was major patient harm). Furthermore, 31% rated general handoff quality to be fair or poor. Less than half the physicians (43.6%) said that handoffs were rarely or never done in a quiet setting and 36.6% reported that they were interrupted one or more times during the majority of handoffs. 8 Based on the survey results, the authors estimated the number of events per year where handoffs resulted in major patient harm. They determined that there were anywhere from 174 to 348 events within a 12 month period where patients experienced major harm due to an inadequate handoff. This range of complications is due to both underestimation and overestimation. 8 Underestimation may occur because residents may not have recognized when the situation occurred or could not recall the event. Also, not every resident responded to the survey. Overestimation may occur from the hindsight bias that residents, as well as any person, would experience. The hindsight bias, also referred to as the “knew-it-all along” effect, entails remembering the situation as worse than it actually was.89 For example, if a student answers a question incorrectly on an exam and later sees the correct answer, he may feel he “knew it all along”, and wonder how he could have forgotten. This applied to the residents surveyed because when they looked back at a situation after having learned that poor handoffs result in harm, they may suddenly assume that it had occurred when it indeed did not. 10 Also, more than one resident could have recounted the same event. There are other cognitive reasons for the possibility that the number of events per year is skewed in either direction. This is because, over time, the human memory is constantly changing the way it recognizes the experiences the way it truly happened the first time. In the case of the residents, they were told new information about handoffs and how they can cause patient harm. This newly acquired knowledge made it difficult to fully assess past handoffs as they really occurred.9,10
Risks Associated with Handoffs
An inadequate patient handoff can impact a patient's safety for many reasons. As an example, the incorrect information about a patient is passed on to the next caregiver, and then the wrong medication or the wrong dosage of medication could be administered. Also, a discharge could be issued when the patient is still ill and, in the case of surgery, an incorrect operation may be performed. Also, if the patient's chart is not up-to-date, treatment that was already administered may be ordered again, or treatment that should be given will not be. Medical charts could also be mishandled and papers from one person's chart could find its way into another's. In the rare cases that two patients have the same last name, the care provider may be reading off the wrong chart. However, this error can be made even if the names were not identical. These are all serious mistakes that could lead to either minor or major harm to the patient.
There are many factors contributing to an incomplete transition of patient specific information. Such factors could be the caregiver feeling fatigued or stressed (which possibly causes them to forget information), limited time, urgency of patient's condition, volume of information, confidentiality, language barriers, noise, lighting, ambiguity of describing information and treatment, not allotting enough time for questions by the recipient, any distractions whatsoever, and/or interruptions from other staff members.11,13 This could lead to wrong treatments, severe adverse events, patient complaints, patient family complaints, and increased hospital costs (due to prolonged hospitalization).
One could hypothesize that a contributor to inadequate patient handoffs for a department of obstetrics and gynecology is that since there are few adverse outcomes each year, and a high volume of normal outcomes, the level of vigilance may be lowered. 4 Because of this low number of sentinel events, “shortcuts” may be taken. Caregivers may feel if what they are doing does not result in error, then they do not need to follow standardized formats and protocols for every situation. People then begin to see risks as justifiable “shortcuts” and attempt to handle more in less time. There are psychological aspects to this. People may be ridiculed for following out safety precautions and thus taking longer time for one patient, versus someone who accomplishes more or sees more patients in an equivalent shift length. 4 When the risks aren't always apparent, they are justified mentally as not being considered risks anymore. An analogy would be a reckless driver on the road. If he drives over the speed limit without any accidents occurring, he feels he can continue this unsafe behavior. However, there comes a time when a car accident does occur and he realizes the risks are indeed there. Unfortunately as time passes after the accident this man will “forget” the risks, and again is speeding on the road. The same could be theorized to apply to medical care. When unsafe behaviors do not always result in patient harm or medical errors they are rewarded and are seen as justified, and therefore caregivers may be less hesitant to use them. 5 The risks will fade into the background until they again negatively affect a patient.
Communication in Patient Handoffs
Communication gaps may be present between different levels of staff. Routinely nurses sign out to nurses, midwives to midwives, physicians to physicians, etc. 5 However, ideally, there should be working teams and all members of the team involved with the specific patient in care should communicate effectively and often. This includes nursing staff, certified nursing midwives, obstetricians, and anesthesiologists as well as others involved. The Joint Commission for Accreditation of Healthcare Organizations (JCAHO) alerted hospitals in July of 2004 that miscommunication between caregivers was a significant factor of adverse events. Sixty-six percent of sentinel events and 85% of the cases for perinatal death and injury reported that year were in part due to miscommunication. 5 When improvements to staff communication are implemented, the amount of adverse outcomes may decline. A study was done at Yale University School of Medicine by the Yale's Obstetric Services to determine if lack of communication contributed to patient safety 14 Yale's Obstetric Services suggested that formal training in communication should be taught not only to caregivers, but to all levels of staff, from those in housekeeping to the most experienced attendings. Furthermore, members of the Yale team initiated new efforts to improve communication. These efforts included the development of a new position of Patient Safety nurse, the establishment of protocols, and the implementation of team training, as well as ensuring that all physicians and nurses obtained their certification in electronic fetal monitoring. There was also a department-based Patient Safety Committee created to oversee any progress being made. Over the course of 3 years, after implementing the previous efforts, the Adverse Outcome Index showed a decline from approximately 3.3% to approximately 1.7%, with R2 = 0.50 and p = 0.01. The decline in adverse events supports the thesis that communication is an essential part of improving patient safety. This ultimately contributes to improved patient handoffs, because effective communication is the foundation of an adequate handoff.
According to the Joint Commission, communication problems contributed to the majority of cases of sentinel events. 15 Adequate communication is required for an adequate handoff. This includes communication between caregivers during a handoff, between the caregiver and patient, between the caregiver and patient's family, and among all members of a teaching team. When exchanging patient specific information, caregivers should introduce themselves to each other. 1 They should also eliminate the barriers to effective communication as much as possible. This includes distractions, ambiguity in language, and location, among others. If caregivers followed standardized formats and were better educated in communication and handoff skills, transitions may result in fewer errors.
Communication between caregiver and patient is also vital. The patient should know who is treating them at all times. Nurses, physicians, surgeons, and whoever else is treating the patient and handling their records should introduce themselves to the patient. It could be postulated that if the patient cannot refer to the name of the caregiver who is attending to them, confusion may arise, as well as anxiety for the patient. In recent years, it has become evident that malpractice lawsuits have increased dramatically 16 and one of the reasons is because patients are becoming more educated in their illnesses. Also, the rise in lawsuits can be associated with the decline in respect for physicians. Paul Nisselle from Australia has stated that the medical profession is “no longer ‘doctor's orders’, it is ‘patient's choice’”. 17 Patients may be unhappy with the lack of communication that they may receive from their physicians. Families of patients may sometimes feel that they are kept in the dark as well. Unfortunately, the doctor-patient relationship is between two individuals who are both human and human error is inevitable. 17 The physician should encourage the patient to ask questions and should make the patient feel comfortable. Ideally the patient should be cognizant about their medical condition and should be forthcoming about any symptoms or concerns. Both patient and physician must work together in order to ensure effective communication between them.
Regulatory Bodies and their Requirements
JCAHO has recognized that patients can be adversely affected by inadequate shift changes and handoffs. They initiated requirements for all accredited hospitals to work on their quality of patient handoffs by having standardized formats. 18 Each hospital is allowed its own method, as long as that method is utilized throughout the hospital. Figure 1 is taken from the Joint Commission's Website, 18 and is an explanation of what is meant by “standardizing” an approach to improving hand-off communication. Essentially, JCAHO requests that staff throughout the hospital be educated of a standardized format that is to be implemented throughout an institution. The handoff process should be consistent throughout an institution, although small changes are allowed to suit each setting for practicality. 18 Such factors that should be incorporated into the standardized approach are as follows: identification of the caregivers involved, the current condition of the patient, diagnoses of the patient, any recent as well as anticipated changes in condition or treatment of the patient, and future recommendations for the next step in treatment. Also, time must be allotted for questions to be asked and answered, preferably face-to-face. Staff members should also identify when to use certain tools or methods during a handoff such as a mnemonic device or repeating back the information.
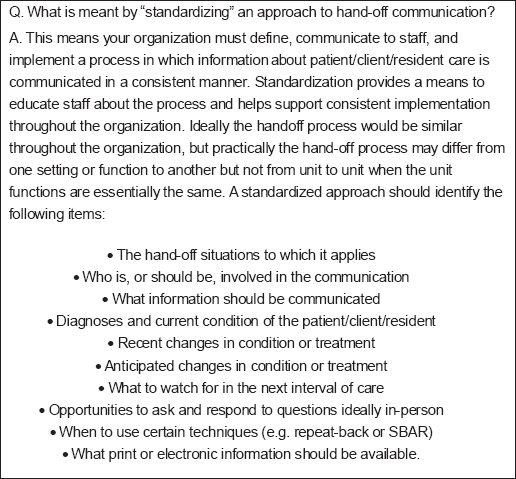
Taken from The Joint Commission's Website. 18
The JCAHO has defined Patient Safety Solutions as, “Any system design or intervention that has demonstrated the ability to prevent or mitigate patient harm stemming from the processes of health care.” 19
Based on the current recommendations in the literature and JCAHO's requirements, 18 any method can be implemented by hospitals as long as it is comprised of the following parts:
An introduction of both caregivers to each other, and to the patient, as well as stating job title (nurse, specialty of physician, specialty of surgeon, etc.) and responsibilities for the patient.
General patient information such as their name, age, gender, location/department, social security number, and any other identifiers necessary.
History of the patient should be included. This entails any background history, prior treatments, previous problems, current medications, and family medical history.
Situation of the patient. This is the patient's level of urgency, current status, medications, code status, fluids, intake, output, intravenous access, and response to treatment.
Assessment of the patient. Any abnormal findings should be reported as well as their pain scale, vital signs, chief complaint, symptoms, and diagnosis.
Risks and or concerns such as if the patient needs isolation or has any allergies. Also any critical lab values should be recorded and fall precautions should be assessed.
Actions/recommendations for future treatment as well as brief rationale.
Time for questions. Questions should be encouraged by both caregivers if any confusion arises or if any information was not covered that should have been.
A Newly Developed Mnemonic: HANDOFFS
A new mnemonic tool that we propose for use in obstetrics and gynecology that would consist of all of the previous criteria mentioned is displayed in Table 1. The mnemonic is “HANDOFFS” and may be useful in the transfer of patient specific information within a department of obstetrics and gynecology. This is because the word HANDOFFS is simple enough for residents and others to easily recall, especially in an event with time constraints, and it covers every aspect of an adequate patient handoff.
A new mnemonic device created to be implemented in the handoff process. This may improve the quality of patient handoffs and ultimately lower the amount of adverse events.
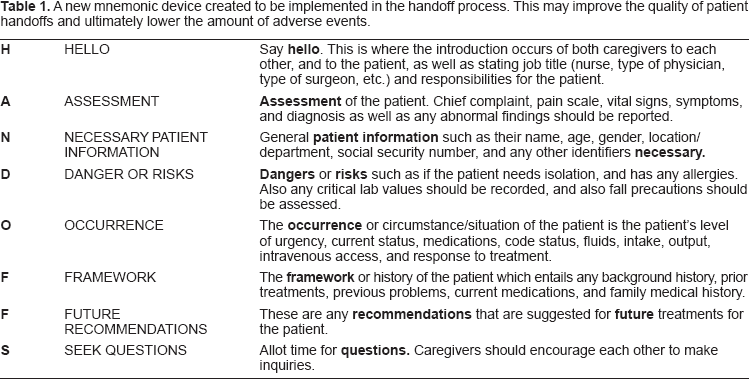
The H represents the word “Hello”, which will instill a friendlier approach to handoffs. It will remind the caregivers, or care providing team involved, to introduce themselves and simply say “Hello” which can instantly make two caregivers who have never met before feel more comfortable with each other. Teamwork is essential to effective communication in obstetrics and gynecology, and by using this device, staff members can work together in a more positive and sociable environment.
This mnemonic can aid with breaking the communication barriers between different members of the team taking care of patients in the department of obstetrics and gynecology. Handoffs may occur between a nurse and a physician, a resident and a medical student, an obstetrician-gynecologist and an anesthesiologist, as well as between other members of a medical team. It reminds people to greet each other with a simple salutation, and to help close the communication gaps between all levels of staff. It is intended to be a user-friendly tool that any member of an obstetrical team could utilize, including nurses and obstetricians and gynecologists.
The remaining letters are as follows: A stands for assessment, N is for necessary patient information, D represents dangers or risks, O is occurrence, the first F is framework, the second F is future recommendations, and lastly, S brings up the opportunity to seek questions.
This mnemonic device may prove to be as valuable as others used thus far. However, there are certain drawbacks to using this mnemonic. This may be too lengthy for a time sensitive situation, in which case the caregiver may forget what each letter represented. Another point is that elements of a handoff may be out of order according to the way a caregiver may have presented their patient specific information in previous handoffs. During the process of a handoff, caregivers may begin with the patient's identifiers as well as a brief history and background. However, when using this mnemonic in order of each letter, the patient's detailed history is discussed towards the end of the handoff. Despite these drawbacks, the mnemonic HANDOFFS covers all aspects of what a handoff should entail and therefore can still serve as a useful tool for improving handoff quality.
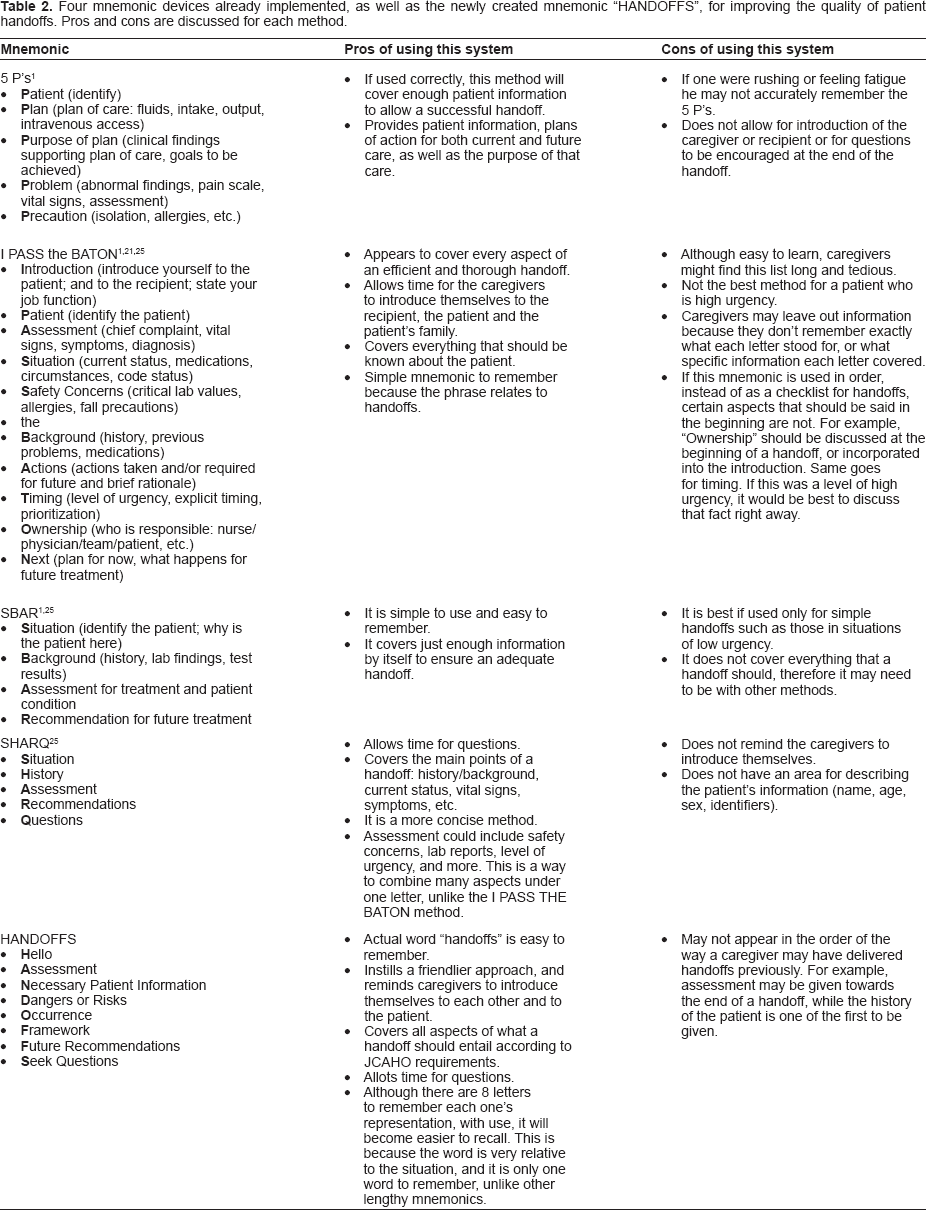
Four handoff methods that also attempt to address the JCAHO requirement which have been implemented by hospitals are shown in Table 2, as well as a comparison of their pros and cons. The methods are the 5 P's, SBAR, I PASS the BATON, and SHARQ. The 5 P's method was developed by Sentara Healthcare in Norfolk, VA. 1 Sentara Healthcare reported a 21% increase in effective handoffs with this method and a decrease in liability claims. 20 I PASS the BATON is recommended by the Department of Defense's Patient Safety Program for use in both simple and complex handoffs. 21 SBAR is a mnemonic device that was inspired by a similar process used on nuclear submarines. 1 This method is a concise way to deliver the information needed between caregivers. SHARQ is also a concise summary of what patient handoffs should entail; however, it covers a bit more than the SBAR method. Our new mnemonic HANDOFFS is also on Table 2 to show a clear comparison of its pros and cons over other methods already utilized. Overall, each mnemonic device covers similar patient specific information that is required to be passed during a handoff.
Four mnemonic devices already implemented, as well as the newly created mnemonic “HANDOFFS”, for improving the quality of patient handoffs. Pros and cons are discussed for each method.
These following are additional recommendations that may enhance the patient handoff process to improve patient safety:
Utilize computerized systems throughout the hospital to allow access to patient information from any department or even at home. 11 This aids in the handoff process because caregivers can quickly access or update patient information from any unit. Patient information could also be accessed at home for a physician who is taking call outside of the hospital.
Designate a sign-out checklist for each team member who is working on the patient to update any information before leaving. This can be done on any one computer through a word processing file as a cost-effective option. 11 Any standardized form would encourage the caregivers to be more organized, and allow the handoff process to be concise and consistent throughout the units of an organization.1,13
Provide enough time during handoffs to allow both caregivers to ask and answer questions. 22
The recipient should take notes during the process.
Set aside a designated room that is quiet, well lit, and without distractions (such as radio, television, other staff members walking in and out) for patient handoffs to occur.8,22,23
If there are any noticeable errors or questionable information, delay the handoff. Do not continue without addressing these concerns. Errors should be acknowledged during the transfer, before the handoff is complete. 22
Language should be clear and unambiguous. Abbreviations or jargon should not be used. Explain thoroughly the symptoms of the patient (i.e. do not say “she is feeling a little unstable”). 12 Avoid confusing terms and vague statements.
Lower the hierarchical barriers. For example, if a resident is speaking to an attending, or any physician with higher status within the hospital (or who has more experience), the resident may fear asking questions or correcting information because they feel they are wrong. The physician should recognize this when the staff is perceived as more junior, and should encourage their questions and concerns. 23
Handoffs should be conducted face to face. 23 This may be due to clarity in reception of information, and a more controlled environment. If a handoff must be done over the phone, information received should be repeated back by the recipient to confirm that it was heard correctly. 22
Use of technology as an enhancement. 12 Audiotapes allow the caregiver to update the patient's information as soon as it is acquired. They can then listen to it later and record it on file or hard copy. 1
Protocols. Certain emergency situations should have protocols that the entire staff is aware of. An emergency can be taken care of more smoothly and effectively with protocols. For example, antenatal care record's detachable pages should be sent at 20 weeks' gestation to labor and delivery area of the woman's hospital. 24 This protocol will ensure that records will not be misplaced or delayed, and be present during a woman's delivery.
Simulation training of emergency events will increase the rate and quality of the handoff process during the response. The entire medical and nursing staff should be trained in certain situations such as emergency cesarean delivery, shoulder dystocia, postpartum hemorrhage, maternal cardiac arrest, and eclamptic seizures. 4 Prior training to a real life situation will better prepare the staff for handoffs during emergency situations.
Education for how to improve patient handoffs should be taught as early as medical school. In addition, it should be incorporated into resident education. 8
Annual hospital meetings dedicated to improving or assessing patient handoffs should be considered for all members and levels of the medical and nursing staff.
Self-awareness. Implementing the use of a camera, a tape recorder, or a nurse designated for patient safety, during the handoff process. This allows monitoring of transitions, which will make caregivers feel more self-aware and less likely to leave out information or to rush a handoff.
Use of activity boards in patient care units to keep staff updated about current status for each patient. 24
Future Directions and Conclusions
There are many improvements for patient handoffs that can be implemented throughout a department of obstetrics and gynecology. This may be a challenge, considering all of the responsibilities that the medical and nursing staff already undertakes. However, patient safety methods should be incorporated to reduce adverse outcomes. Effective leadership and contribution from all levels of staff will aid in the initiation of new methods and the continuity of the use of the methods. Certain aspects of inadequate handoffs may be addressed in future studies. Studies can be conducted to see if there is a certain time of day where handoffs result in the most medical errors. Also, a mechanism could be proposed in which the process of a handoff could be paused immediately when an error occurred. Another factor that could be measured is if there is a difference between genders during the handoff process. For example, if a male handing off to another male, or a female handing off to another female, are there any differences in the number of medical errors that occur? In addition, studies could be done to compare the new method “HANDOFFS” versus already implemented methods (SBAR, SHARQ, etc.) to show which is the most effective for which circumstance. The search for improving the quality of patient handoffs will continue until the most effective methods are found and implemented, given its vital role in patient safety.
Disclosure
The authors report no conflicts of interest.