
Abstract
Background
Patient satisfaction is becoming an increasingly prevalent topic in medicine, but little is known about patient satisfaction in women's health and other specialties. We review current methods of improving patient satisfaction in the field of obstetrics and gynecology with the intent to increase patient satisfaction even further by enhancing and combining previously used strategies.
Methods
A search from inception to June 2010 for electronic literature was performed using Medline. The search strategy used the medical subject heading terms “patient satisfaction”, “obstetrics”, “gynecology”, “patient-centered communication”, “communication training”, and “malpractice”. The company websites for Press Ganey Associates, Inc and Integrated Health Associates' were also reviewed. Studies in both general medicine and the field of obstetrics and gynecology were reviewed to emphasize disparities between patients' satisfaction in diverse medical specialties.
Results
Studies indicating the importance of patient satisfaction, the factors contributing to patient satisfaction, and an evaluation of current, evidence-based methods of increasing patient satisfaction were reviewed. The studies included suggest that current methods of assessing/improving patient satisfaction are effective, but may not be the most productive.
Conclusions
We expect that the combination of previously successful methods of improving patient satisfaction to allow physicians to employ individualized patient-centered communication may improve patient satisfaction even further. Studying the use of our proposed enhancements in physician-patient communication may be worthwhile tools to increase patient satisfaction and optimize the quality of women's healthcare.
Keywords
Introduction
A heightened focus on patient satisfaction is becoming more prevalent throughout the medical field, as several associations have been drawn between patient satisfaction and pay-for-performance payouts, malpractice litigation, and overall patient health outcomes and compliance.1–12 In this article, we review several factors that may affect a patient's overall satisfaction, such as the physician's communication style, patient's expectations for the visit, and whether patients have unanswered questions at the end of their visit.2–10,13 Current methods of assessing and improving patient satisfaction, which abstract data from surveys to develop overall conceptual ideas on the origins of patient satisfaction will also be discussed. 14 Deficits in communication skills training will be reviewed and possible solutions to enhance patient satisfaction through the training will be suggested. Finally, a new method is proposed in this review, which may enhance patient satisfaction in the field of obstetrics and gynecology, as well as in other fields, by combining and enhancing previously successful methodologies of increasing patient satisfaction. The effectiveness of the previous methods of increasing patients' satisfaction leads us to the hypothesis that a more comprehensive method may increase patient satisfaction even further.
Modern Significance of Patient Satisfaction
Pay-for-performance programs
Patient satisfaction is quickly being incorporated into modern medical jargon, as it may have several fundamental implications in the medical field today.1–12 Economically, pay-for-performance programs are on the rise due to the shift toward patient-centered care and the need for improved payment systems. Pay-for-performance programs are meant to promote improvements in the quality of patient care such as greater patient satisfaction and patient safety by providing medical institutions with monetary incentives. Patient satisfaction has been a key indicator in the measurement of medical institutions' performance in pay-for-performance programs and has been incorporated into the majority of them, as research shows a strong correlation between patient satisfaction and patient quality and quality outcomes. 1 Both the American Academy of Family Physicians (AAFP) and The Medical Group Management Association (MGMA) emphasize the importance of incorporating patient satisfaction as an indicator of performance in pay-for-performance programs. 1
The Integrated Healthcare Association (IHA), a leadership group of California health plans funded through membership dues and grants, is an example of an organization involved in a pay-for-performance program with patient satisfaction as an indicator of performance. The IHA's goal is to “reward physicians for their performance in clinical care and patient experience by providing a clear set of health plan expectations, use of common metrics, and public reporting”.12,15 Performance measures incorporated into the company's pay-for-performance plan include clinical quality, patient satisfaction, and investment in information technology. Clinical measures of performance instituted by the IHA which may influence the field of obstetrics and gynecology include breast cancer screening, evidence-based cervical cancer screening, and Chlamydia screening. 16 The area of patient satisfaction from measurement years 2003 to 2007 accounted for 40% of the total performance score throughout all medical institutions with IHA plans; overall performance in this concentration is based on communication with the doctor, timely care and service, specialty care access, and an overall rating of care. 12 Total pay-for-performance payouts made by the IHA, with 40% of the total payouts made up of patient satisfaction measures, have generally increased from 2003 to 2007. 12 More substantial payouts to a medical institution may result from improvements in patient satisfaction, as many health plans are using patient satisfaction as an indicator of physician performance in pay-for-performance programs.
Malpractice litigation
Malpractice litigation is another factor associated with patient satisfaction. “Approximately one out of four physicians receives a complaint every year, and 65% of physicians are sued sometime during their career”, which indicates the frequency of medical litigation. 3 In the field of obstetrics and gynecology, according to the 2006 American College of Obstetricians and Gynecologists (ACOG) survey on professional liability, “the risk of an ACOG member being sued for malpractice during his or her career is 89.2% and rising”. 17 The greater percentage of malpractice suits in the field of obstetrics and gynecology indicates the existence of disparities between patients' satisfaction in different medical fields.
Interpersonal aspects of care may have sizeable affects on the decision for a patient to sue their physician, as malpractice proceeding have not only been found to be associated with physician error and negligence but also with the quality of physician-patient communication.2–7,9 The lack of patient satisfaction with physician-patient communication may be an important determinant of malpractice lawsuits.3–7,9 A study done by Ambady et al found that surgeons who were deemed more dominant and less concerned in their tone of voice were more likely to have been sued than surgeons who were deemed less dominant and more concerned in the presence of their patients. 9 The dominance and lack of anxiety in the surgeon's voice may imply to the patient that the physician is unconcerned and may lead a patient to instigate a malpractice suit if poor outcomes occur. 9 Previous studies of patients who filed malpractice claims against their OB/GYNs reported “feeling rushed, feeling ignored, receiving inadequate explanations or advice”. 17 Barrier et al reported that physicians with no malpractice claims filed against them seem to allow patients to express all of their concerns, check to make sure they understand the patient's concerns, allow patients to divulge their thoughts, and are generally more warm and friendly than physicians who have malpractice claims filed against them. 4
Patient compliance
Patient satisfaction has also been linked to increased patient compliance. More specifically, the communication style of a physician has been linked to patient satisfaction and compliance on the patient's part to the recommended course of treatment.4,7–8,10–11 Zandbelt et al described that physician visits in which patients were able to freely express their feelings, concerns, opinions, and questions were seen to produce better outcomes and to increase patient satisfaction. 11 A patient who feels that she/he has a decision/role in the selected course of treatment may be more apt to follow their treatment regiment, which may lead to better outcomes and increased patient satisfaction in turn.
Factors Associated with patient satisfaction
Physician-patient communication
According to Dr. F. Daniel Duffy of the American Board of Internal Medicine, “physicians must be as attentive to developing and refreshing communication skills as they are to developing and refreshing diagnostic and therapeutic skills”. 4 Physician-patient communication may be a key determinant of how satisfied the patient is following the medical interview and is one of six core competencies for graduating medical residents according to the Accreditation Council for Graduate Medical Education (ACGME). 18 Enhanced patient satisfaction, increased compliance with the recommended course of treatment, decreased malpractice claims, and an improvement in overall clinical outcomes have been associated with the quality of physician-patient communication.5–6,8,10–11
“Biomedical” and “patient-centered” interviewing styles are the two extremes in physician-patient communication during a medical consultation. A mock dialogue between a patient and a physician who utilizes either biomedical or patient-centered communication is portrayed in Figure 1.
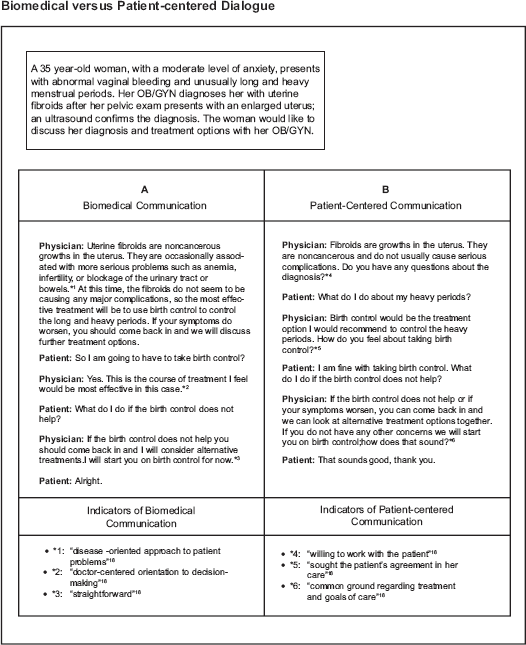
Mock dialogues between a patient and a physician applying either biomedical or patient-centered communication are portrayed.
Biomedical communication skills include “a disease-oriented approach to patient problems and a doctor-centered orientation to decision-making”. 18 A study completed by Swenson et al in which the responses patients had to pre-recorded physician-patient interviews which either focused on patient-centered or biomedical communication were investigated. 18 The study found that some patients preferred a biomedical style physician due to the fact that the physician “wanted action, like right now…She gave it her best shot right away”, was “more knowledgeable”, had “clear expectations” and a “straightforward” manner. 18
Conversely, patient-centered communication aims to ensure that the patient's concerns, expectations, and ideas are expressed so that the problem may be fully explored and understood by the physician. 18 The study by Swenson et al found that the reasons some patients preferred a patient-centered style physician included that the physician was “willing to work with the patient”, “seemed really concerned about the patient overall …She seemed to put together a comprehensive plan …[and] sought the patient's agreement in her care”, and responded to the “patient as a person”. 18 Patient-centered communication involves “developing an understanding of the patient as a person, conveying empathy, and finding common ground regarding treatment and goals of care”. 7 Patient-centered communication is thought to promote a sense of agreement between the physician and the patient about the treatment plan which is thought to increase patient satisfaction and adherence to the recommended course of treatment. 11
Overall, Swenson et al found that although the majority of patients (69%) preferred a patient-centered communication style, a considerable minority (31%) preferred a biomedical communication style. 18 Patients may have diverse preferences as to which communication style they prefer, and although the patient-centered majority was favored in the study, the minority that preferred biomedical communication may be too substantial to ignore.
In the field of obstetrics and gynecology, physician-patient communication may need to be altered to an even greater degree in order to improve patient satisfaction, as “obstetrics and gynecology patients often differ greatly from general patients, in terms of their moods and emotions”. 19 Health problems that gynecologists are faced with are often intimate in nature and may have a high emotional impact. 2 First-time expectant mothers are a prime example of patients in which physicians should be increasingly vigilant to the communication style used. Most first-time expectant mothers “are tense and nervous, with high levels of uncertainty, and an inability to control their own body”. 19 Childbearing women are also at especially high risk for depression, whether the onset was previous to the pregnancy, during the pregnancy, or postpartum. Between 10 and 20 percent of women are affected by depression either during their pregnancies or within a year of their deliveries, which may necessitate increased vigilance to physician-patient communication for the patient to be adequately satisfied with the communication exchange. 20
Overlooking patient concerns
Failure to discuss a patient's expectations during the medical interview may also decrease patient satisfaction. 7 If the physician does not allow the patient to fully express the reason for the visit, the patient may leave dissatisfied, although the physician may not even be aware of it. According to a study by Shilling et al, patients may not articulate their questions unless specifically asked by the physician, as they may feel they are wasting the physician's time or they may seem imprudent. 13 The study also found that patient satisfaction may be increased by merely asking the patient if they have additional questions before leaving the consultation. 13 Inquiring as to whether the patient has additional questions prior to the end of the medical interview may ensure that the patient does not leave with unanswered questions and that her expectations of the visit are fulfilled, which may be expected to increase patient satisfaction.
Current Methods of Assessing/Improving patient satisfaction
Communication skills training
Communication skills training may be effective in improving physician-patient communication, which may subsequently increase patient satisfaction. There is substantial evidence that structured communication skill training improves clinicians' ability to communicate with their patients.21–23 Back et al designed a communication skill workshop called Oncotalk in which 115 medical oncology fellows participated. 21 The workshop included techniques in giving bad news and discussing transitions to palliative care. 21 Oncotalk participants began with a median of 8 communication skills and acquired a median of 6 new skills when interacting with patients, demonstrating the efficacy of communication skills training. 21 Another study by Meyer et al enrolled 106 interdisciplinary clinicians involved in pediatric critical care in a one day communication training program. 22 Participants of the study were nearly unanimous (93% to 98%) in reporting that they had learned a valuable repertoire of communication skills, broadened their relational capacities, and increased their clinical confidence. 22 According to Marcia Levetown and the Committee on Bioethics, “health care communication is a skill that is critical to safe and effective medical practice; it can and must be taught”. 24 The Accreditation Council for Graduate Medical Education now requires competency in communication skills for residents and fellows, 21 which furthers the importance of educating physicians in communication skills.
Improvements in communication skills, which enhance physician-patient communication, may also increase patient satisfaction. Sullivan and Beeman examined the relationship between patient satisfaction and physician-patient communication in maternity care. 25 They looked at measures of communication such as enough time spent discussing problems, using words the patient could understand, trying to understand how the patient felt, and patient satisfaction, and found that “each of their measures of communication had a statistically significant relationship with satisfaction with prenatal care”. 25 Another experiment by Haskard et al involved the communication training of 156 physicians from three primary care specialties including obstetrics and gynecology. 26 They found that physician communication training improved patient satisfaction with “overall care”, improved physicians' information-giving skills, increased patients' quality of care ratings, and their willingness to recommend the physician. 26
Although communication skills training may be an effective component of increasing patient satisfaction, the skills learned may be difficult to implement across disparate situations, diverse personalities, and a variety of patient expectations. Psycho-oncology literature indicates that the type and amount of information provided to each patient should be modified to meet the individual needs of each patient. 23 Improvements in the implementation of communication skills training to make the training useful in a variety of contexts and medical settings may be expected to increase patient satisfaction even further. We believe that the data presented supports that physician communication skills training is an important factor in improving patient satisfaction but also acknowledge that enhancements may be necessary to optimize patient satisfaction in different medical situations.
Patient surveys
Several surveys exist that attempt to gauge patient satisfaction following the patient's meeting with the physician. Post-medical consultation surveys are collected to assess what patients liked/disliked about their physician visit, in hopes of improving patient satisfaction in the future. Press Ganey Associates, Inc. is a company providing more than 7,000 health care facilities with the tools to improve their performance. 14 Press Ganey processes more than 11 million surveys annually in hopes of improving patient satisfaction, physician engagement, patient loyalty, and patient safety. 14 A compilation of results, abstracted from the individual surveys, representing preferences of the population as a whole may subsequently be analyzed. Current survey methods provide medical institutions with valuable insight into the factors associated with increasing patient satisfaction. Stawiski et al stated that Press Ganey's surveys of patient satisfaction measures may provide “a vital roadmap to efficient and effective enhancements in health care delivery”. 1 Although surveys of a patient's likes/dislikes following their physician visit may be useful in assessing a population's preferences in general, individual preferences may be overlooked. Patient satisfaction may not be reaching an optimal level if individual preferences and patient needs are overlooked. Again, we recognize the importance of the patient survey as a technique to improve patient satisfaction, but acknowledge the opportunity for enhancement to optimize the level of satisfaction attained.
Enhancing Current Methods of Improving Patient Satisfaction
Physician communication skills training
Although the medical interview is a physician's primary and conceivably most important feature in formulating a patient's diagnosis and gaining valuable patient information, practicing physicians' physician-patient communication capabilities vary widely. 4 We believe that communication skills training will allow physicians to broaden their knowledge of different communication styles which may allow the physician to communicate more effectively with the patient. While the physician may have the tools to communicate effectively, how will the physician gauge what the patient expects, what type of communication style he/she prefers, and what questions he/she may have pertaining to the visit, in order to apply the best tools to the individual patient's current situation?
While physician communication skills training may be associated with improvements in patient satisfaction in certain medical fields, it has not shown to be statistically significantly better in others.13,25 Altering physician communication skills training techniques may be necessary to improve patient satisfaction in diverse specialties. Communication skills found to be useful in each individual medical specialty should be determined. For example, the communication skills workshop, Oncotalk, discussed earlier to improve skills in giving bad news to cancer patients and discussing transitioning to palliative care, used the acronym SPIKES to remind physicians of the steps involved in giving bad news to patients. The steps include, “1) preparing the
Patient preference form
We propose creating a new tool that may allow physicians to assess a patient's needs prior to the medical interview in order to effectively apply their communication skills training. While physicians may posses the necessary tools to communicate effectively with patients, it may be difficult for them to correctly assess the patient's desires in the context of different situations. Currently, there is no standardized, efficient way of assessing the type of communication an individual patient prefers, other than human intuition and prior experience.
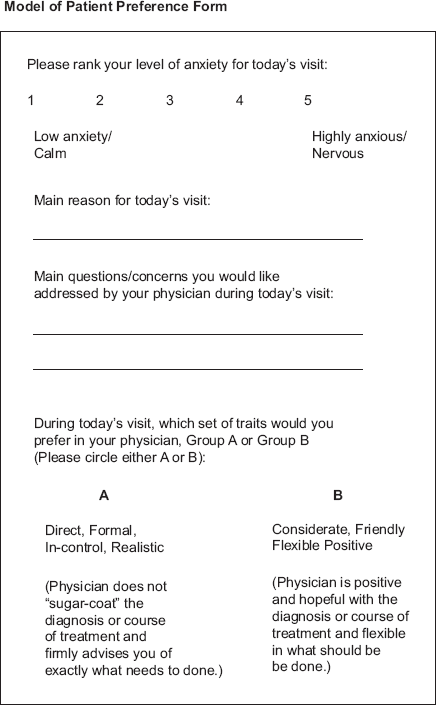
We propose a patient preference form, a tool that may allow a proper evaluation of patient needs prior to the medical interview (Fig. 2). The questionnaire, would address the patient's level of anxiety, main reason for their current physician visit, questions/concerns they may have during the current visit, and communication style preferences at the current visit (the
This model of a
The patient's self-indicated level of anxiety may provide a sign as to the communication style the patient prefers and the precaution that should be taken by the physician during the medical interview to attempt to alleviate rather than heighten patient anxiety. Assessing the patient's main reason for their current visit as well as their main questions and concerns prior to the visit may ensure the patient's needs are fully met by the conclusion of the medical interview. According to Barrier et al, discovering the patient's true complaint and expectations at the end of the interview may waste both the patient and physician's time. 4 Therefore, uncovering the patient's desires upfront may be the most effective communication strategy, as it has been seen that once the physician interrupts the patient, the patient may be more hesitant to continue expressing their true concerns. 4 The questionnaire may ensure that the patient has all of their questions and concerns addressed; if the patient becomes nervous in the physician's presence, the physician will have the responses available on the questionnaire. Prior knowledge of the patient's needs may lead to a more satisfying and efficient medical interview for both the patient and the physician.
The final portion of the questionnaire will address the patient's communication style preferences. Side A of the communication style chart represents traits of a biomedical physician, while side B represents traits of a patient-centered physician. The physician may look at the chart to see if side A or B is circled so he/she will immediately know whether to use a biomedical or patient-centered approach during the current visit. Although the two communication styles, biomedical and patient-centered, are opposites, insight into the patient's choice may provide a significant indication as to the type of communication they require during the current medical interview. The patient preference form may ensure that physician-patient communication is optimized and the major patient concerns are addressed. Since a patient's preferences may vary between different medical settings, we acknowledge that a physician may have to tailor his/her communication to fit the current needs of the patient. Communication skills training may provide the tact and skill necessary to effectively tailor the communication style of the physician to fit the current preference of the patient. It may be worthwhile to study the use of this proposed tool as an instrument for increasing patient satisfaction.
E.D.U. method of enhancing patient satisfaction
We also propose the creation of a new method to enhance patient satisfaction. The
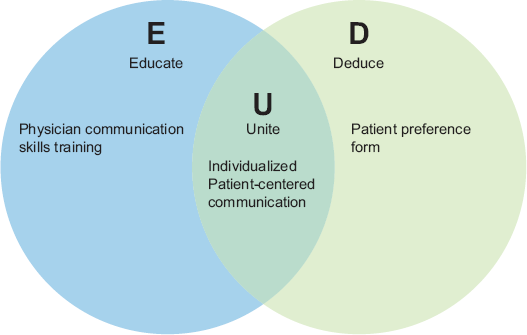
The
The term “individualized patient-centered communication”, enhances the previously used term patient-centered communication;7,11,17 the term implies the use of patient-centered communication, but will be made unique to each individual patient and medical interview. Individualized patient-centered communication may be the key to connecting better with diverse patients under different medical circumstances; for example, patients may have different expectations of their physician during a general medical consultation than during their obstetrics and gynecology consultation.
Individualized patient-centered communication is the “U” (Unite) of the
Conclusion
In summary, the diversity of patient needs in the field of obstetrics and gynecology may require more attention to physician-patient communication in order to enhance patient satisfaction. The
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.