
Abstract
Objective
Our objective was to review the involved mechanisms and propose actions for controlling/treating abnormal uterine bleeding during climacteric hormone therapy.
Methods
A systemic search of the databases SciELO, MEDLINE, and Pubmed was performed for identifying relevant publications on normal endometrial bleeding, abnormal uterine bleeding, and hormone therapy bleeding.
Results
Before starting hormone therapy, it is essential to exclude any abnormal organic condition, identify women at higher risk for bleeding, and adapt the regimen to suit eachwoman's characteristics. Abnormal bleeding with progesterone/progestogen only, combined sequential, or combined continuous regimens may be corrected by changing the progestogen, adjusting the progestogen or estrogen/progestogen doses, or even switching the initial regimen to other formulation.
Conclusion
To diminish the occurrence of abnormal bleeding during hormone therapy (HT), it is important to tailor the regimen to the needs of individual women and identify those with higher risk of bleeding. The use of new agents as adjuvant therapies for decreasing abnormal bleeding in women on HT awaits future studies.
Introduction
Hormone therapy (HT) is the most effective method for relieving the effects of hypoestrogenism following menopause, particularly vasomotor symptoms with high prevalence in different populations.1–3 Despite the benefit of the HT, unscheduled/unwanted bleeding decreases patients' compliance with long-term use.4,5 Though abnormal bleeding is the main cause for HT discontinuation, there are no established guidelines for preventing or treating it during HT in climacteric women. Few studies have been published on this subject6–9 likelybecause the knowledge of the exact mechanisms of bleeding use of different regimens remains limited.10,11 In the absence of clinical guidelines, the objectives of this review are (1) to propose actions to treat bleeding in combined sequential regimens based on current knowledge of mechanisms that trigger the onset of bleeding and assure endometrial repair, and (2) to propose actions to correct breakthrough bleeding that occurs with combined continuous regimens regardless of the duration of use. According to the current classification of the causes of abnormal uterine bleeding, the bleeding that occurs with the use of sex steroids is defined as iatrogenic, 12 and this review considers the definitions of spotting/bleeding occurring with combined hormonal contraceptives for defining spotting/bleeding occurring in combined HT (Table 1).
Proposed definitions of different types of bleeding during hormone therapy.*

Adapted from reference 12.
Methods
The review, structured in sections, was developed after a detailed analysis of the publications found on scheduled or unscheduled abnormal bleeding in menopause women receiving HT via different administration routes, doses, and regimens. The main objective was to provide recommendations for the management of women with abnormal bleeding on hormone therapy. The databases SciELO, MEDLINE, and Pubmed were searched to identify the most relevant publications over the last few years. This database search was expanded through a search for and review of bibliographic citations in the articles consulted. If the citations provided essential knowledge, older articles were also included. Only articles or reviews published in journals with an editorial board were examined. Studies were limited to levels of evidence 1 to 3 and degrees of recommendation/strength of evidence from A to C. Therefore, the best available research evidence was used to develop some of the recommendations. Keywords included in the search were hormone therapy, menopause, climacteric, abnormal uterine bleeding, dysfunctional uterine bleeding, endometrium, sex steroids, and menstrual bleeding.
Steroid preparation for hormone therapy
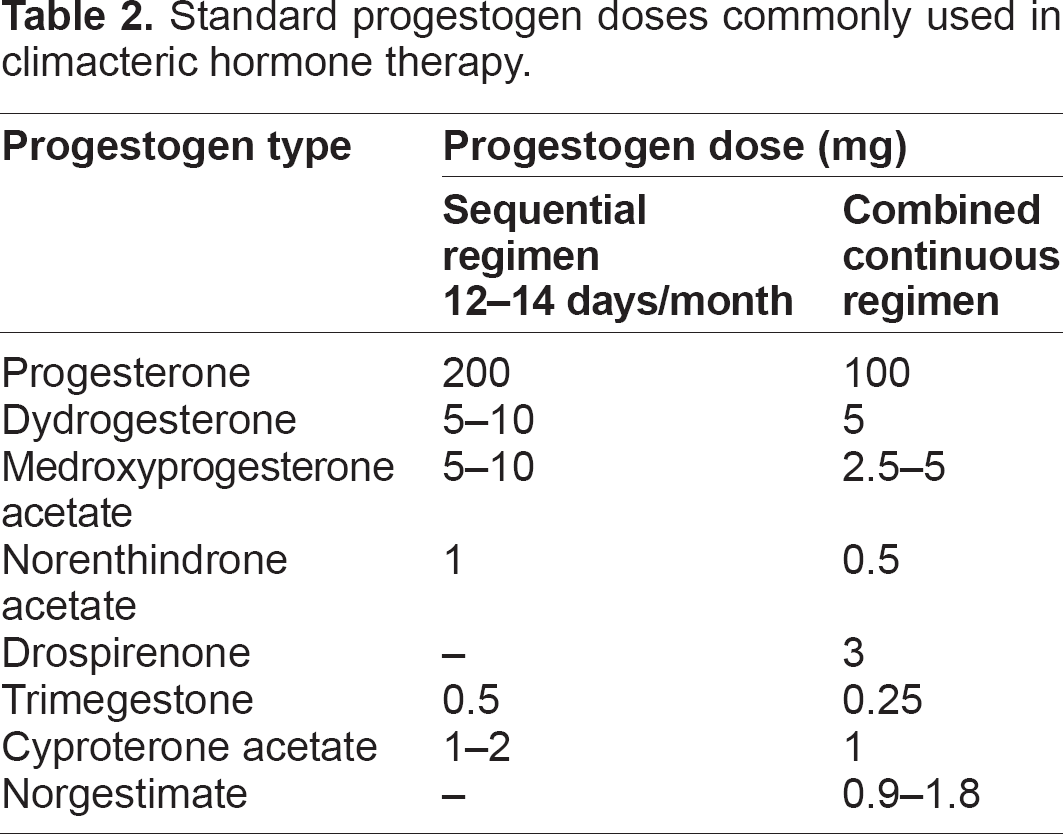
Even though the endometrial response is highly variable with different preparations, regimens, and women's ages, an estrogen/progestogen balance should be individualized to assure the protective effect of the endometrium and avoid abnormal bleeding. Concerning the estrogen component, 2 mg of estradiol valerate, 1 to 2 mg of oral 17β-estradiol, 0.625 mg of oral conjugated estrogen, and 50 μg of estradiol transdermally are the recommended standard daily doses. Nevertheless, it must be taken into account that the estrogen dose by itself may influence the incidence of irregular bleeding.9,11 A variety of progestogens are used combined with estrogens in HT. As some of these progestogens may cause unwanted metabolic effects or negate the beneficial effects of estrogen, the choice of progestogen type, dose, route, and the number of days of its administration should be based on a consideration of adverse effects and endometrial impact. 13 There is little information concerning how to choose a progestin for a particular patient, but the progestin's androgenic and metabolic properties and the impact on the endometrium should be considered. 14 The recommended progestogen doses for endometrial protection in HT are shown in Table 2. Considering the type of progestogen, it seems that endometrium hyperplasia is more prevalent with regimens containing levonorgestrel or medroxyprogesterone acetate (MPA) than those containing norethisterone acetate.11,15,16 The cyclic combination of 2 mg of 17-beta-estradiol and 10 mg of dydrogesterone offers adequate endometrial protection even if given for three years. 17 Conjugated estrogen 0.625 mg associated with 2.5 mg of medroxyprogesterone acetate also assures endometrium protection for three years of use. 18 When these estrogens were associated with 5 mg of MPA, the positive result was a decrease in bleeding intensity. 19
Standard progestogen doses commonly used in climacteric hormone therapy.
Endometrial modifications with hormone therapy
In the abnormal menstrual cycle, the diameter and total glandular area of the endometrium are greater than those seen in the normal cycle even though the stromal cellularity remains unaltered in the luteal phase. If the progestogen dose is unbalanced or high in any HT regimen, the result is small total area and glandular diameter, lower height of the glandular epithelium, reduced glandular secretion, a lower number of microvessels, and a higher number of dilated venules. All of these modifications facilitate abnormal bleeding. 20 Therefore, in HT, the progestogen dose should be high enough to inhibit glandular cell division without causing secretory modifications. It must be considered that there are different endometrial responses to the same regimens among individuals, however. Concerning the type of progestogen, it appears that levonorgestrel, desogestrel, and medroxyprogesterone acetate when given in low doses do not reduce the estrogen receptors, but the expression of progesterone receptor density may suffer significant alterations with the different regimens of HT. 21
It seems there is no significant increase in the endometrial vascular density in patients using HT when compared with nonusers, but in HT users, the endometrial vessels are fragile and have only endothelial cells, basal lamina, and pericytes to support their structure and lack the muscle cells responsible for vasoconstriction. 22 In the endometrium, HT seems not to determine significant increases in stromal vascular caliber, alteration in the expression of Matrix metalloproteinases (MMP), or increases in the vascular endothelium growth factor (VEGF) production.22,23 However, the different progestins used in HT preparations may alter the balance between angiogenic promoters (VEGF) and inhibitors (thrombospondin-1). 23 Despite the HT regimen, either combined sequential or continuous, endothelial cells are found spread among the vessels and extravascular tissues. 24 With the combined continuous regimen, there is a reduction in smooth muscle actin in the vascular wall and pericytes and greater leukocyte invasion, explaining the greater endometrial vascular fragility in users of this regimen. In fact, some studies have shown that leukocyte invasion, expression of metalloproteinases (MPs), and their tissue Inhibitor of metalloproteinases (TIMPs) may be altered in the endometrium of HT users, mainly during the bleeding episode. 25 With this regimen, increased endometrial stromal proliferation, alteration in endometrial integrity, remodeling, and repair also occur as a consequence of the increased endometrial microvascularization associated with the higher activity of local enzymes, growth factors, and other regulatory molecules.21,23,25
Histological aspects of the endometrium under the influence of hormone therapy
Atrophic, inactive, proliferative, early secretory, late secretory, and hyperplasic endometria have been reported in HT users of different regimens. Endometrial biopsies have been performed both in the absence of and during bleeding episodes. 17 Comparison of the biopsies found in bleeding patients with those performed in patients with no bleeding, under the same regimens of HT, have not shown different results. 26 In those patients with abnormal bleeding, biopsies have shown atrophic (12.5%–44%), proliferative (6%–35%), hyperplastic (3%–19%), secretory (8%–16%), carcinomatous (1%–2%), hyperplastic associated with cancer (11%), and dysfunctional abortive (1%–2%)8,21 endometria.
In general, partial or complete secretory transformation occurs in most patients receiving the combined sequential regimen,15,26 and biopsies performed during the progesterone phase have shown endometria weakly secretory, secretory (40%–48%), proliferative (5.5%–36%), inactive (7%–40%), atrophic (7%–25%), dysfunctional (1%–2%), or hyperplastic (5%–8%).21–30 In the users of the combined continuous regimen, biopsies have shown endometria atrophic in 26% to 69%, proliferative in 13%, dysfunctional in 5%, or hyperplastic in 2% to 5%. 31 Nevertheless, adding the results of biopsies with atrophic endometrium plus those with insufficient material for analysis, the percentage increases up to 90% of cases. 32 The presence of endometrial polyp or other endometrial pathology have been reported in 7% to 8% of cases, regardless of which regimen is used.27,33
Mechanisms of abnormal bleeding during hormone therapy
The mechanisms involved in endometrial bleeding during HT are poorly understood. While normal menstrual bleeding is universal and involves two-thirds of the endometrium, the bleeding that occurs during HT is focal and involves only the upper layer of the endometrium. As a result of this difference, unwanted, unpredictable, intermittent, and, at times, prolonged bleeding are common occurrences in women on HT. Unlike what happens during menstruation, when bleeding is mainly the result of the spiral arterioles rupture, 34 bleeding during HT comes from damaged newer microvascular capillaries developed in the endometrium. 35 Abnormal bleeding does not occur in all women on HT, and the reason for this is unknown, but in those with bleeding, the bleeding may be associated with endometrial changes already mentioned: higher stromal expression of growth factors, alteration in the synthesis of MMP and its TIMPs, increased proliferation of the endothelium vascular, reduced proliferation and differentiation of the musculature of spiral arterioles, and reduced endothelin expression.25,36
The type of bleeding may or may not be related to the histology, dose, and type of estrogen and progestogen used or to an imbalance between these two steroids. 37 Exogenous estrogens, both natural and synthetic, with doses used in HT, have practically the same endometrial impact as endogenous estrogens. However, exogenous progestogens are more potent than progesterone, and, generally, they induce premature atrophy in the glandular epithelium and stromal cell decidualization. 13 In case of an excess in the progestogen component in a certain formula, an increased 17-hydroxysteroid dehydrogenase activity may promote greater conversion of estradiol into estrone and increased endometrial vascular fragility.35,38
Little attention has been paid to the vascular and molecular mechanisms underlying breakthrough bleeding in users of the combined continuous regimen, but, under this regimen, there is little formation of spiral arterioles and endothelins,11,23 and breakthrough bleeding seems to occur as a result of atypical microvascularization formed, enzymatic vascular alteration, and impaired hemostatic mechanisms.11,23 Because the microvascularization has only endothelial cells and the basal membrane is poor in laminin, proteoglycans, and pericytes, there is greater vascular fragility, facilitating the appearance of bleeding in the first months of HT. In addition, the bleeding by itself can stimulate local release of regulatory molecules (MMPs, interleukins, and growth factors) and compromise the integrity, remodeling, and repair of the microvascularization.23,25 With continued and more prolonged use, the normal structure of the basal membrane of the endometrial vessels is restored, reducing the likelihood of breakthrough bleeding in the following months. 39
In the combined sequential HT regimen, with continuous estrogen and cyclic progestogen, withdrawal bleeding should occur at the end of the progestogen sequence and present the characteristics of normal menstrual bleeding. 17 With this regimen, the expected normal bleeding should occur only after the 10th day of progestogen, when administered orally15,40 or after the 8th or 9th day, when administered transdermally. 41 If the estrogen dose is insufficient in relation to the action of the progestogen in the formula used, normal bleeding may occur for 4 to 5 days after the end of the progestogen sequence, and endometrial healing may be delayed, translated by persistent spotting at the end of the bleeding period. On the other hand, if the progestogen dose is insufficient, early sloughing of the endometrium may start before the end of the sequence of progestogen tablets, and this bleeding may persist in small amounts for several days before increasing; the result may be a prolonged flow.35,40,42
Prevalence of abnormal bleeding during hormone therapy
Both combined sequential and continuous HT regimens were developed to result in the patient having predictable bleeding or to have no bleeding at all. 43 In clinical practice, the prevalence of abnormal bleeding in HT users will depend on myometrial integrity, endometrium thickness, whether the woman is in the premenopause or postmenopause period at the start of replacement therapy, the time that has elapsed since menopause, the pattern of bleeding before menopause, the dose and type of sex steroids, the regimen used, and the treatment duration.31,44–49
In the sequential regimen, irregular bleeding is expected to occur in 8% to 40% of users (Table 3). More than half of users of this regimen may bleed before day 11 of the progestogen sequence, and less than 10% of women may experience recurrent episodes of breakthrough bleeding. 50 On the other hand, the percentage of women with abnormal bleeding on the combined continuous regimen, either oral or transdermal, ranges from, 0% to 77% in the first few years of treatment (Table 4).44,51–54 With this continuous regimen, the percentage of women with bleeding decreases after 6 to 12 months of use, and after 9 months, it is expected that only 3% to 10% will still present this complication.32,45,55 In the transdermal route, the percentage of women who still present bleeding or spotting after 12 months of use ranges from 10% to 20%. 56
Occurrence of abnormal bleeding with different hormone preparations used in the combined sequential HT regimen.

Occurrence of abnormal bleeding with different hormone preparation used in the combined continuous HT regimen.

It must be always considered that both regimen and estrogen dose are important factors in the occurence of abnormal bleeding.31,53,57,58 With the continuous combined regimen with the lower dose of estrogen, bleeding occurs in around 20% of users, and when higher doses are used, bleeding may occur in up to 43% of users.19,59 Besides the estrogen dose, the types of estrogen and progestogen used also seem to be relevant in inducing bleeding.14,31,60 Information on this aspect is very limited, but endometria exposed to conjugated estrogens associated with medroxyprogesterone appear to be more vulnerable to bleeding than endometria exposed to the association of estradiol and norethisterone (12% vs. 26%, respectively). 19 When the years postmenopause are considered, it seems that the longer the time period after menopause that HT is started, the less prevalent is abnormal bleeding.19,61
Causes of abnormal bleeding during hormone therapy
The most common causes of abnormal bleeding during climacteric HT are poor compliance, the incorrect use of steroids, concomitant use of some broad-spectrum antibiotics, forgetting to take the HT tablets, alterations in absorption or metabolism/excretion of hormones, lack of synchronization between endogenous and exogenous hormones in the perimenopausal users, endometrial exposure to an unbalanced percentage/quantity of estrogen-progestogen, excess of estrogen, prolonged use of estrogen without association of adequate doses of progestogen in women with a uterus, abnormal influence of specific local factors, presence of arteriovenous abnormalities in the uterus, and myoendometrial alterations not identified in the initial assessment of the patient.9,62–64 Despite the strong recommendation not to start HT in the presence of uterine abnormalities to ensure better compliance with treatment, uterine pathologies such as fibroids, polyps, and adenomyosis still seem to be responsible for 27% to 30% of reported cases of abnormal bleeding associated with HT.11,65,66
Management of abnormal bleeding during hormone therapy
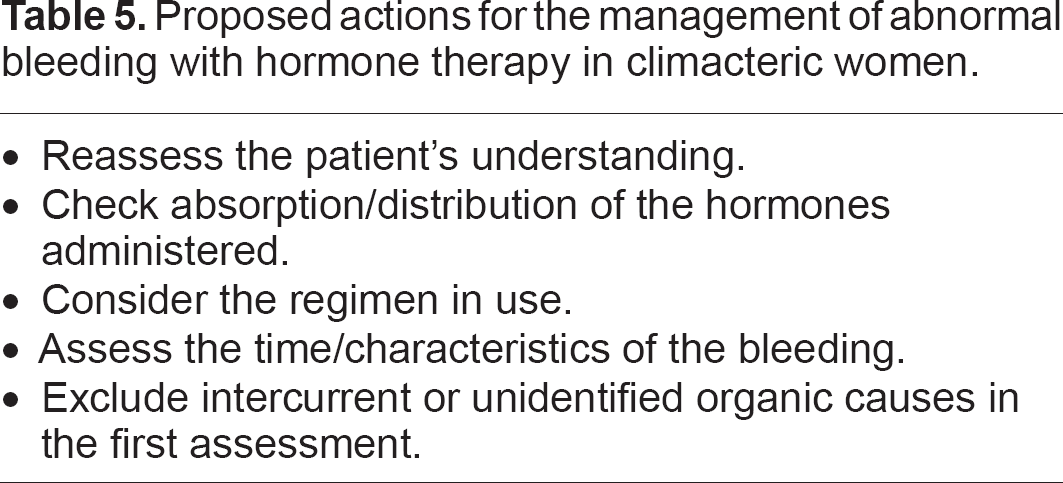
There is little consensus regarding what to do about persisting bleeding or when reinvestigation should be performed on HT users with bleeding. As no practice guidelines to help clinicians in managing their patients have been available till now, this review offers some rationale recommendations. It is important to highlight that any action to stop the bleeding at an appropriate time should be based on the correct identification of the underlying cause. 34 Specific objectives for managing abnormal bleeding during HT are provided in Table 5. All the recommendations proposed in this review are based on the current knowledge of the role of sex steroids in menstrual physiology; interactions between sex steroids and endometrium; and the role of growth factors, interleukins, and MMPs in abnormal endometrial bleeding. Previous publications concerning HT and bleeding management have been extensively reviewed.7,11,35,46,67
Proposed actions for the management of abnormal bleeding with hormone therapy in climacteric women.
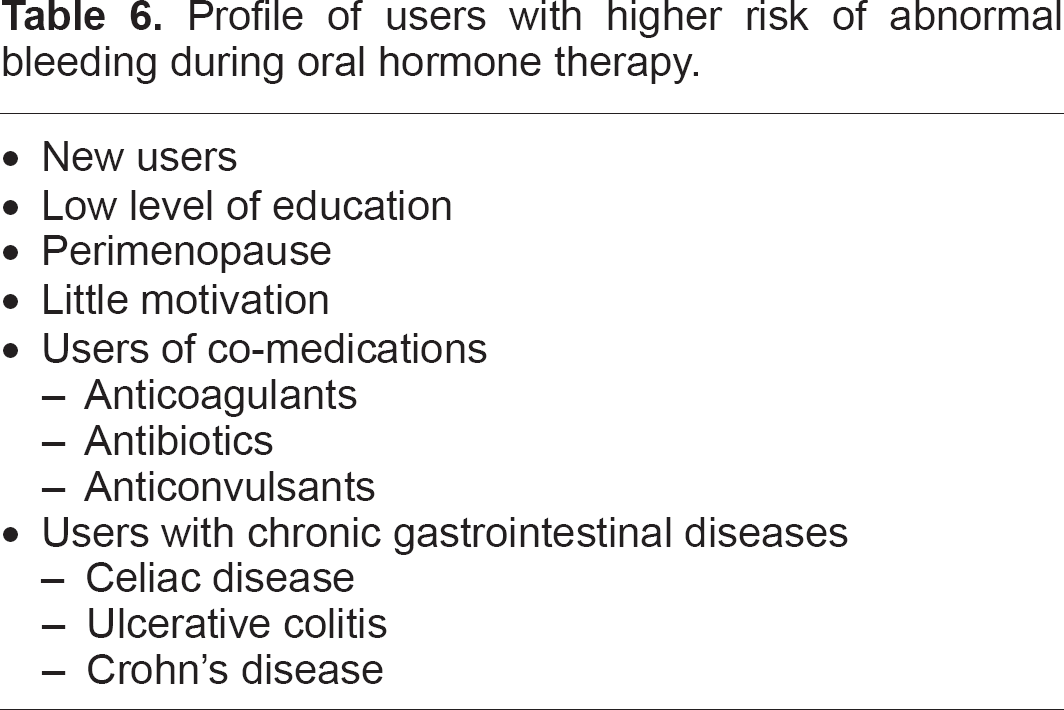
As an initial and general preventive measure, it is important to tailor the regimen to the needs of individual women and identify those with a higher risk of bleeding (Table 6). Though it seems to have no correlation between endometrium thickness, endometrial histology findings, and bleeding patterns, biopsy is recommended when abnormal bleeding persists beyond the first 6 to 12 months of use or when it occurs after a long period of amenorrhea.6,7,9,68,69 The appropriate choice of the estroprogestogen combination seems to be relevant for minimizing the bleeding. However, regarding the control of abnormal bleeding, there is no robust data indicating any advantage of one estrogen or progestogen over another.8,11,26 As a rule of thumb, two basic actions are recommended for the treatment of abnormal bleeding during HT: (1) ensure that there is no underlying organic disease and (2) stop the undesired bleeding.
Profile of users with higher risk of abnormal bleeding during oral hormone therapy.
Management of abnormal bleeding in users of cyclical progesterone/progestogen
In the premenopausal patient suffering hot flushes but still with some endogenous production of estrogen and deficient or absent secretion of progesterone, an option for starting HT is to add a progestogen to reverse the effects of unopposed estrogen in a cyclical way. At least 10 days of the progestogen agent is required to assure a secretory transformation and prevent endometrial hyperplasia. The most commonly used progestogens are medroxyprogesterone acetate and noresthisterone acetate. 7 If the use of a cyclical progestogen is the chosen regimen, it is necessary to monitor eventual ovulation to synchronize the moment of starting the exogenous administration of the progestogen with ovulation. 70 In the continuation of this regimen, the progestogen should be maintained cyclically for 12 to 14 days each month. 71 If prolonged and/or profuse bleeding occurs when the progestogen sequence is stopped, the cause may be an either too low or too high progestogen dose or because the endogenous estrogen production is now insufficient for assuring an adequate proliferation of the endometrium.
In the case of a too-low progestogen dose, the bleeding may start before the end of the progestogen sequence, imitating what takes place in the luteal phase with insufficient progesterone production. 70 In this case, the progestogen should be increased sooner, usually by 2.5 mg of adenosine monophosphate (AMP) or an equivalent amount of another progestogen in the first 36 hours of bleeding; after two days of bleeding, the addition of the progestogen does not have the same effectiveness in stopping the abnormal bleeding.6,72 In the continuation of this regimen, the new progestogen dose should be maintained. On the other hand, if the progestogen dose is too high, the bleeding may be characterized by prolonged spotting for a few days. As a consequence of the estrogen receptor depletion,47,73 the progestogen dose should be decrease thereafter. The adjustment of the progestogen dose based only on time of appearance and the physical aspect of bleeding is still speculative, and more controlled studies are needed. If patients present abnormal bleeding after a period of time receiving this regimen, the ovarian estrogen production could be reassessed by measuring both estradiol and follicle-stimulating hormone (FSH) levels at an interval of at least seven days after stopping the hormone. 74 If the estradiol levels are normal and the FSH levels are still low, the cyclical addition of progestogen could be maintained. If the FSH level is high, the regimen should be changed to a combined sequential preparation.
Management of abnormal bleeding during combined sequential hormone therapy
Sequential HT is also recommended in the premenopause and perimenopause periods, while some ovarian activity still is present. 71 The most common preparations used in this regimen are shown in Table 3. Differences between menstruation and progestogen withdrawal bleeding are probably due to endometrial exposure to different estrogen or progestogen types, relatively low estrogen endometrial exposure in HT, and continuation of estrogen administration without decreasing it through the bleeding phase. After the progestin sequence withdrawal, the continual ingestion of exogenous estrogen at the correct dose guarantees reepithelization of the endometrium and cessation of the bleeding within a few days.7,26,70,75
When prescribing this regimen to women with ovulatory but irregular cycles, it is also necessary to synchronize the endogenous production of ovarian steroids with the exogenous estroprogestogen administration in the first month of treatment. 70 A practical method to get this condition is to wait for the next spontaneous mentrual flow before starting the HT. When abnormal bleeding occurs during this regimen the following crucial points should be considered to assure a correct management: (1) whether the ocurrence of bleeding is in the estrogen or progesterone phase, (2) the duration and volume of the bleeding, (3) whether there is a prolonged period of amenorrhea after starting the HT and before the occurrence of the abnormal bleeding, and (4) the possibility of interference of concomitant medication.7,75
Unpredictable bleeding in the initial estrogen phase may be a consequence of an insufficient estrogen dose, error in taking the hormone, deficient absorption, accumulation of estrogen, or even an unbalanced or unsuitable type of progestogen being administered.14,16 The bleeding in the initial estrogen phase has the characteristic of prolonging the bleeding initiated after stopping the progestogen sequence. Clinical recommendations in this case consist of verifying any alteration in absorption to assure greater rigor in the regularity of taking doses, adjust the estrogen or progestogen dose, and reassess the condition of the endometrium.7,9 A commonly recommended procedure is to increase the estrogen dose or reduce the progestogen, or, even if the progestogen is norethisterone, change it to a progestogen with a lower inhibitory impact on the endometrium.13,40,46 There have been no robust clinical trials that have addressed these issues yet, and sometimes interventions may be unsuccessful.
In around 36% to 50% of users of this regimen, unexpected bleeding occurs in the progestogen phase before the end of the progestogen tablets.15,50,76 For practical purposes, this bleeding can indicate insufficient estrogen/progestogen absorption, failure to have taken the doses correctly, insufficient estrogen dose, or more likely, insufficient progestogen dose, particularly if the endometrial biopsy reveals the presence of mitoses.29,68 Usually the users of this regimen with full secretory transformation of the endometrium present normal cycle length and scheduled bleeding after stopping the tablets containing the progestogen. 15 Those with shorter cycle length, in whom the bleeding starts while the women is still taking the progestogen tablets, may present endometrium with different histological aspects.15,68,76 The current recommendations to correct the bleeding consist of increasing the progestogen dose and reviewing the patient three months later.60,70,77 If the bleeding was not resolved, another progestogen with greater endometrium atrophic effect should be introduced.26,46,57,78 In case of spotting before the 10th day of the progestogen sequence, the progestogen/estrogen ratio may be to high, and increasing the estrogen dose seems to be the most appropriate measure. 8 If this measure is unsuccessful, a reassessment of the endometrium should be scheduled. Bleeding occurring after the 10th tablet containing progestogen suggests both an excess of estrogen or low progestogen dose.9,37,77 Increasing the progestogen dose is recommended as an initial measure.46,79 Failing this measure, the dose should be balanced by lowering the estrogen.31,39 If none of these measures are successful, a change of HT regimen should be considered. 6 Even though data are still limited, switching the sequential composition to a combined continuous regimen at around two years after the mean age of menopause is recommended, with the purpose of reducing irregular bleeding.8,80
Management of abnormal bleeding in combined continuous hormone therapy
Adequate management of abnormal bleeding in users of this regimen must consider that the abnormal bleeding may occur due to greater endometrial sensitivity to the estrogen or progestogen, endometrial atrophy, endometrial decidualization, insufficient formation of estrogenic receptors, vascular abnormalities, or fibrous endometrial atrophy.20,21 The occurrence of bleeding depends on the type, dose, and balance of the proportions of estrogen and progestogen.57,81 The most common preparations used are shown in Table 4. The main form of presentation of bleeding in this regimen is the appearance of unscheduled spotting rather than bleeding. 82 Unfortunately, the pattern of bleeding seems to show no distinction between types and doses of the sex steroids used. 32 In clinical settings, due to different bioavailability and potency, the type of progestogen should be taken into consideration. 83
As with continued use of HT, the cumulative rate of amenorrhea is increased; in the first six months, the woman should only be followed, giving her confidence while waiting for the complete cessation of bleeding over time of usage.16,31,32 As a general recommendation, when bleeding persists for more than 12 months, a reassessment of the endometrium should be carried out. If the endometrium is normal at his point, the estrogen dose should be decreased,57,84,85 but if the endometrium is underdeveloped, the estrogen dose should initially be increased. 7 There is no proof that these interventions are particularly effective, however.8,35 If these procedures are not successful, changing the progestogen to norethisterone acetate, which has a more intense atrophic effect, could be tried. 19 Attempts to increase the progestogen dose are generally ineffective, 86 but this can also be tested.40,55,60,80 In the last decade, a reduction of 50% in the occurrence of abnormal bleeding has been observed by reducing the estrogen dose or even by decreasing doses of both components.31,39,58,59,87,88
Adjuvant measures and future directions for research
The ultimate cause of abnormal endometrial bleeding during HT treatment is capilar disfunction, so this review points out that an adequate approach should aim to (1) increase vascular stability, (2) reduce proteolysis of the vascular wall and extracellular matrix, and (3) maintain epithelial integrity and normal endothelial formation.
Taking into account a possible excess in vasodilatating prostaglandin production with any HT regimen, the use of nonsteroidal anti-inflammatory drugs could be considered as an adjuvant measure in the management of women with excessive bleeding during HT.89,90 The administration of doxycycline as an MMP inhibitor may inhibit proteolysis and degradation of the extracellular matrix and reduce inflammatory cytokines in endometrium, 89 but its clinical use is still controversial in treating abnormal bleeding in women using oral hormonal contraceptions.91,92 Its use to decrease bleeding in HT needs to be determined in future studies. As antioxidants (vitamin E) and flavonoides (vitamin B complex) have been shown to be effective in correcting vascular fragility and stabilizing the vessels, the therapeutic effect of these preparations as adjuvant measures in HT abnormal bleeding could be tested.93,94 Vitamin E has been useful in reducing abnormal bleeding in users of low-dose progestogen alone but not in HT users. 94 In case of an excessive progestogen effect with reduced estrogen receptor density and increased vascular fragility, the intermittent use of low-dose antiprogestogen to correct abnormal bleeding in HT may also be investigated.95,96
Conclusion
Even though the recommendations presented in this review are essentially based on the pathophysiological effects of sex steroids on the endometrium, growing knowledge of the newer intimate paracrine and intracrine mechanisms involved in endometrial bleeding have supported testing new agents for the management of uterine abnormal bleeding.89–91 Literature supporting the effectiveness of the different interventions for controlling abnormal bleeding during HT is still limited. More controlled studies are needed to examine the importance of the physical aspects and timing of bleeding in determining the best clinical procedure. In the same way, research to adequate a particular combination of estrogen, progestogen for an individual woman's characteristics is still needed. As general guidance, it is important to ensure that both the myometrium and endometrium are normal before starting any HT regimen. Once structural pelvic conditions have been ascertained, any subsequent bleeding may be controlled or corrected by appropriate adjustment of doses and types of sex steroids or even by changing the regimen. If these measures are unsuccessful, the use of new agents such as metalloproteinase inhibitors, VEGF inhibitor, or progesterone antagonists could be considered as adjuvant therapy.
Footnotes
Acknowledgements
The authors thank Biomed Proofreading for English copyediting of the manuscript.
Author Contributions
Conceived and designed the experiments: SFM. Analysed the data: SFM, MMWY, JSB. Wrote the first draft of the manuscript: SFM. Contributed to the writing of the manuscript: MMWY, JSB. Agree with manuscript results and conclusions: SFM, MMWY, JSB. Jointly developed the structure and arguments for the paper: MMWY, JSB. Made critical revisions and approved final version: SFM. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. The paper was approved by the ethical committee of the Federal University of Mato Grosso.