
Abstract
Background:
During the menopause transition, one in three women experiences abnormal uterine bleeding. Few studies have evaluated the probability of hysterectomy associated with abnormal uterine bleeding during the menopause transition.
Objectives:
To estimate the risk of hysterectomy associated with abnormal uterine bleeding, specifically prolonged or heavy menstrual bleeding, during the menopause transition.
Design:
Prospective cohort study
Methods:
We used data collected in the Study of Women’s Health Across the Nation, a community-based, longitudinal cohort that followed women from pre- to post-menopause. It includes 1200 White (45.4%), Black (15.4%), Japanese (20.8%), and Chinese (18.4%) women, from three study sites that participated in a sub-study and provided at least 1 year of prospectively recorded menstrual calendars. Calendars ascertained bleeding days, menstrual interference with life in four domains (work, daily life, sexual life, and relationships), menopausal hormone therapy, and smoking. At baseline and 12 annual follow-up visits, information on surgeries, body mass index, pelvic pain, and socio-demographic characteristics was obtained. Multivariable Cox proportional hazard models were used to assess the relationships of hysterectomy with prolonged menstrual bleeding, heavy menstrual bleeding, and covariates.
Results:
Women who reported prolonged menstrual bleeding had an elevated hazard of hysterectomy (hazard ratio = 2.35, 95% confidence interval = 1.20–4.61), adjusting for pelvic pain, hormone use, and race/ethnicity; hazard ratios were attenuated after adjusting for life interference. The association of heavy menstrual bleeding with hysterectomy was not statistically significant (hazard ratio = 1.34, 95% confidence interval = 0.42–4.30). The adjusted hazard ratio for hysterectomy increased 1.5-fold for each domain in which bleeding interfered with a woman’s life. Pelvic pain, hormone therapy, and Black race were also significant predictors of hysterectomy risk.
Conclusion:
Prolonged menstrual bleeding during the menopause transition, particularly when accompanied by interference in one or more domains of a woman’s life, increased the risk of hysterectomy. Counseling women about non-surgical therapeutic options, and estimating the proximity of menopause, may mitigate against this increased risk.
Plain language summary
As women approach the menopause, they are likely to experience episodes of prolonged or heavy menstrual bleeding. We found that frequent episodes of prolonged menstrual bleeding were associated with an increased risk of hysterectomy particularly when bleeding interfered with women’s lives.
Introduction
During the menopause transition (MT), declining ovarian function and increased probability of anovulation can alter menstrual timing, duration, and flow; one in three women experiences abnormal uterine bleeding (AUB).1,2 AUB is an abnormality in bleeding duration, amount, or frequency lasting at least 6 months. 3 Prolonged menstrual bleeding (PMB) is defined as >8 days of flow, and heavy menstrual bleeding (HMB) is defined as menstrual blood loss sufficient to interfere with women’s physical, social, emotional, or material quality of life.4 –6
AUB during the MT has several underlying causes, including hormonal changes and increasing probability of anovulatory cycles that accompany the MT, an increase in structural causes (e.g. polyps, fibroids) with age, uterine or cervical neoplasia, and coagulation disorders.1,3,4,7 The standard first-line treatment approach is medical therapy, including nonsteroidal anti-inflammatory drugs, transexamic acid, gonadotropin releasing hormone (GNRH) agonists, anti-fibrinolytic drugs, and levonorgestrel-releasing intrauterine system.1,7 Surgical options include endometrial ablation, hysteroscopic resection of polyps and myomas, and myolysis.1,7,8 However, repeated treatment is often needed due to unsatisfactory outcomes. 7 Hysterectomy definitively ends AUB but is more expensive and carries greater adverse event risk than medical therapies and minimally invasive surgeries.8,9 Women who are proximal to menopause may elect to “wait it out,” or onset of AUB during the MT may lead them to elect hysterectomy.
Few studies have evaluated the probability of hysterectomy associated with AUB during the MT. Having previously reported on AUB prevalence during the MT in the Study of Women’s Health Across the Nation (SWAN), 2 the current study aimed to assess the probability of and risk factors for hysterectomy associated with AUB during the MT. We hypothesized that women with AUB would be more likely to have a hysterectomy than women without this condition, and that risk would be greater when bleeding interfered with women’s life.
Methods
SWAN is a longitudinal cohort study of midlife women. Enrolled in 1996 when they were pre- or early-perimenopausal and assessed again at 13 follow-up visits on an approximate annual basis as they transitioned through menopause, 10 women were eligible for the cohort if they were aged 42–52 years, not pregnant or lactating, had had a menstrual cycle in the previous 3 months, had a uterus and at least one ovary intact, and were not taking exogenous hormones affecting ovarian function at the time of enrollment. At baseline and each follow-up visit, women completed questionnaires about their menstrual, gynecological, and medical history, including information on surgeries and exogenous hormone use, and were asked to maintain a monthly record of their menstrual bleeding from enrollment until 2 years after their final menstrual period (FMP) or for up to 10 years, through 2006. The present analyses included women from the three SWAN sites (Michigan, Los Angeles, and Northern California) who participated in a sub-study with supplemental calendar questions about whether bleeding interfered with quality of life. In addition to White women, the Michigan site enrolled Black women, the Los Angeles site enrolled Japanese women, and the Northern California site enrolled Chinese women.
A total of 1498 women were enrolled at these three sites of whom 1320 (92.8%) completed monthly menstrual calendars. We excluded six women because they experienced their FMP prior to their first completed calendar and 114 who provided <1 year of bleeding data, leaving a total of 1200 women eligible for our primary analysis (Figure 1).
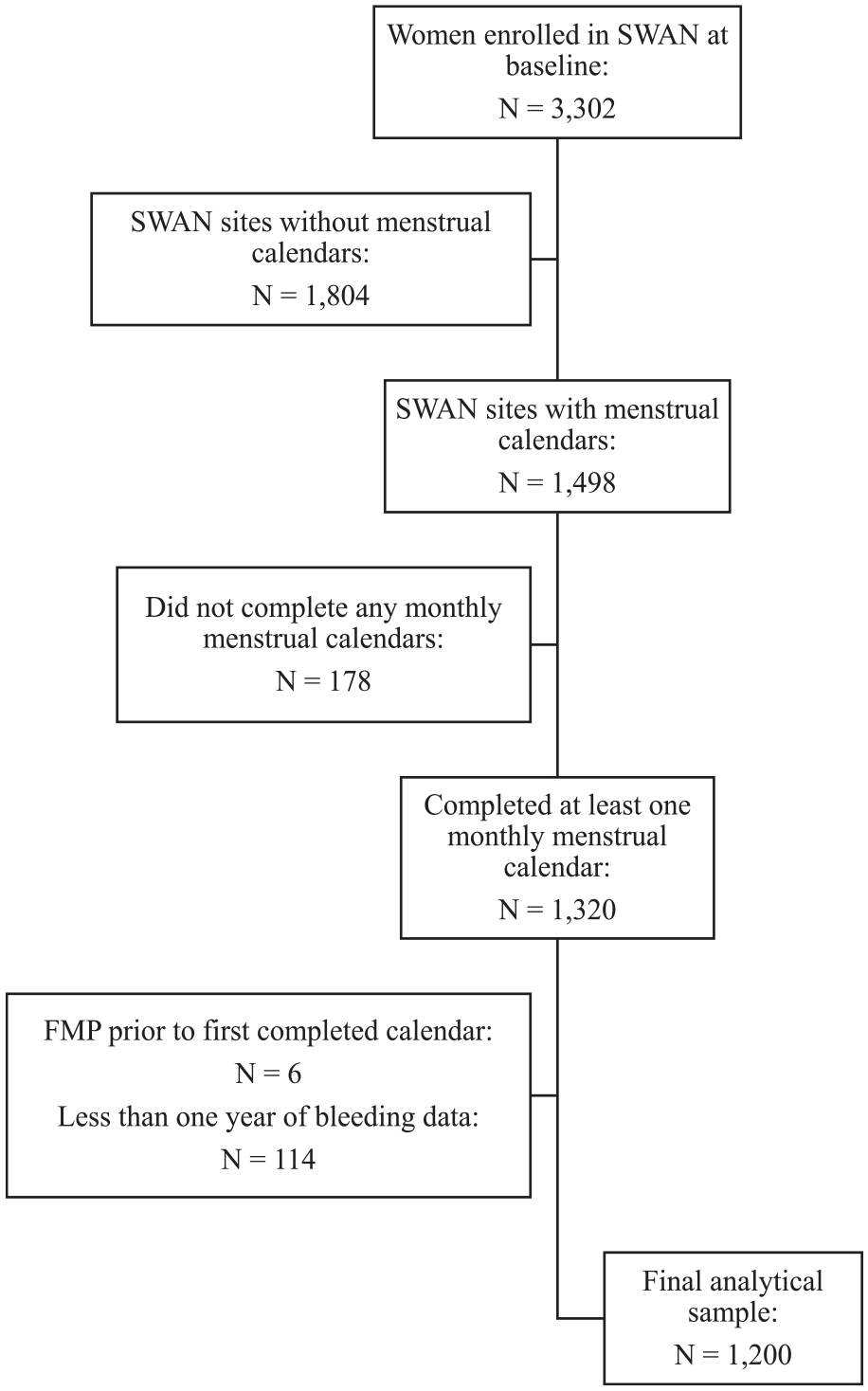
Derivation of the study population sample.
Abnormal uterine bleeding
PMB was defined as experience of three or more episodes of bleeding that lasted more than 8 days within the past 6 months. 5 Heaviness of flow was recorded using the following pre-specified categories: spotting (bleeding not requiring the use of a sanitary product or not filling a regular-sized sanitary product); light to moderate bleeding (sanitary protection was required but only needed change a few times per day or every 3–4 h); or very heavy bleeding (needing to change sanitary product every 1–2 h for more than 4 h during the day). HMB was defined as experience of three or more episodes of very heavy bleeding lasting 3 or more days in the past 6 months. 2 PMB and HMB were modeled as time-varying covariates, beginning once 6 months of the calendar data had been collected and then varying by 1-month intervals, ending with hysterectomy (n = 75), FMP (n = 563), or when a woman stopped providing menstrual calendar information (n = 562).
Menopause
MT stage was assessed at each study visit based on women’s self-reported menstrual characteristics and classified as premenopausal if they reported no change in menstrual regularity, early peri-menopausal if they had had a menstrual period in the previous 3 months but decreased regularity in the past 12 months, late peri-menopausal if they had a menses in the prior 11 months but no menses in the prior 3 months, and postmenopausal if they had had no menses for the past 12 or more months. 11 At each follow-up, women indicated whether they had had a hysterectomy since their last visit and the month and year of their surgery.
Covariates
Covariates were selected based on factors previously associated with experience of HMB or PMB in the SWAN cohort 2 and included time-varying hormone use (yes/no) and smoking status (yes/no) reported on the monthly calendar within each 6-month window, time-varying pelvic pain and obesity measured at each annual follow-up, and time-invariant sociodemographic characteristics. Obesity (body mass index < or ⩾30.0 kg/m2) was based on measured weight and height. Reported pelvic pain was coded positive at the first reported instance of experiencing pelvic pain within the past year. Age, self-reported race, and ethnicity (Black versus White, Chinese, or Japanese), education (high school graduate or less than high school versus at least some college), and difficulty of paying for basics (very hard, somewhat hard, or not hard) were obtained at baseline. The menstrual calendar asked each month whether bleeding had interfered with one’s life in four domains (work, daily life, sexual life, and relationships). Interference was defined as the number of different types of interference a woman reported due to bleeding within each 6-month window. We did not adjust for reported fibroids as they are associated with hysterectomy through their impact on bleeding and/or pelvic pain. These analyses aimed to understand the association between these symptoms and the risk of hysterectomy.
Statistical analysis
Frequencies, means, and standard deviations were calculated for categorical and continuous variables, respectively. All reported hysterectomies are included in these analyses. Frequency differences, between women who had had a hysterectomy and women who had not, were tested using chi-square tests. Cox proportional hazard models were fit to assess the relationship of hysterectomy risk with PMB and HMB, and each covariate. Bivariable and multivariable models were fit, and respective crude and adjusted hazard ratios (HRs) and their 95% confidence intervals (CIs) were calculated. Race/ethnicity was modeled as Black women versus all other groups (White, Chinese, and Japanese combined), as only Black women had an elevated risk. For the multivariable models, the Akaike Information Criteria were calculated beginning with each bleeding variable and adding variables associated in unadjusted analyses with hysterectomy risk and compared to assess model fits, leading smoking and obesity status to be dropped from the multivariable models. Women were censored at their FMP or at 3 years after their last calendar observation if they had not yet reached their FMP. Women who reported a hysterectomy at an interview 2 or more years after their FMP were censored at their FMP. To explore potential mediation of the relationship between AUB and hysterectomy by life interference, we used the R dpasurv package (https://cran.r-project.org/web/packages/dpasurv/index.html) to run a dynamic path analysis, 12 which allows for both time-varying exposures and time-varying mediators with a time-to-event outcome. The time-to-event outcome was modeled using Aalen’s additive model to estimate cumulative effects over time. As the package does not allow for time-varying confounders we adjusted only for Black race in the dynamic path analysis. In sensitivity analyses, we limited the analysis to the 1016 women who provided at least 1 year of data during the early MT (i.e. excluding women who were enrolled in the late perimenopause or who dropped out before providing 1 year of calendars during the early MT). In another analysis, we excluded four women who either had known cancer/suspicious mass as the primary indication for hysterectomy or a cancer/suspicious mass listed on the hysterectomy abstraction form. Statistical analyses were performed using R statistical software, version 3.1.0 (www.R-project.org). The reporting of this study conforms to the STROBE statement. 13
Results
Participating women had a mean age of 46.3 years (standard deviation = 2.7) at baseline. During the study period, 29.8% of women ever reported menses >8 days at least three times within 6 months, and 17.3% ever reported heavy bleeding of 3 or more days at least three times within 6 months, while 65.5% ever reported that their menstrual period interfered with at least one aspect of their life (Table 1). During the study period, 29.9% of women ever reported pelvic pain, and 31.7% ever reported the use of hormones.
Frequency of PMB and HMB and characteristics of the study population by hysterectomy status, the Study of Women’s Health Across the Nation (n = 1200).

HMB: heavy menstrual bleeding; PMB: prolonged menstrual bleeding.
p value is from chi-square test of ever having hysterectomy.
Obesity is defined as body mass index ⩾ 30 kg/m2.
Seventy-five (6.3%) women reported having had a hysterectomy during the follow-up period, with the proportion of women having hysterectomy being higher among those who ever reported PMB (44.0%), HMB (29.3%), and/or any life interference due to bleeding (74.7%), pelvic pain (53.3%), or hormone use (60.0%).
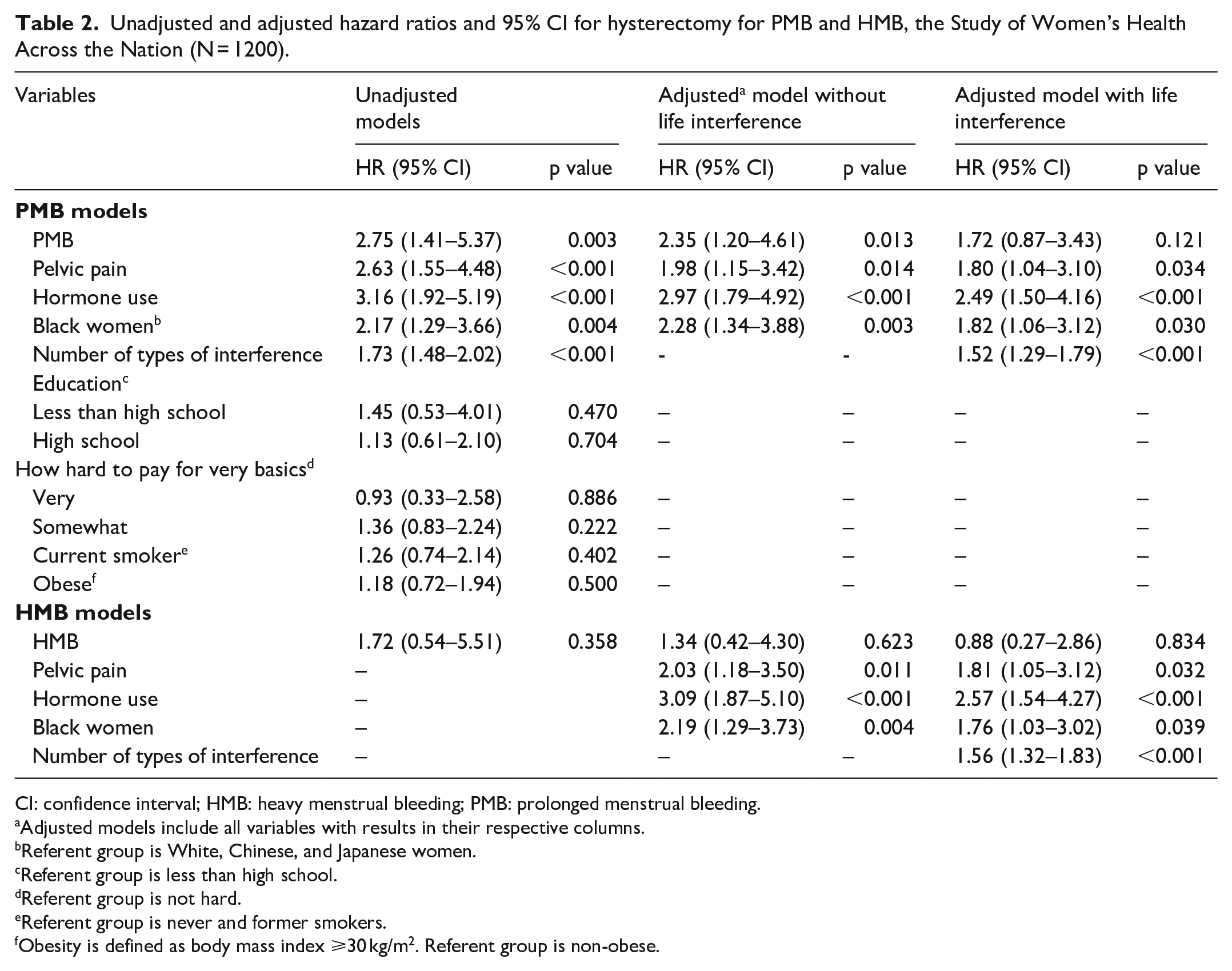
Kaplan–Meier survival curves show the relationship of PMB and HMB with hysterectomy (Figure 2). In unadjusted analyses (Table 2), experience of PMB at least three times within 6 months was associated with a HR of 2.75 for subsequent hysterectomy (95% CI = 1.41–5.37). The hazard of hysterectomy following the experience of HMB at least three times within 6 months, although elevated (HR = 1.72), was not statistically significant. Each additional type of interference due to bleeding (work, daily activities, sexual life, or social relationships) was associated with a 1.73 increase in the hazard of hysterectomy. Women who reported pelvic pain also had more than a two-fold increased hazard of hysterectomy (HR = 2.63, 95% CI = 1.55–4.48). Women who reported hormone use had a three-fold increased hazard of hysterectomy (HR = 3.16, 95% CI = 1.92–5.19). Compared to White, Chinese, and Japanese women, Black women had nearly a two-fold increased hazard of hysterectomy (HR = 1.95, 95% CI = 1.11–3.42). Educational level, economic strain, smoking, and obesity were not associated with hysterectomy risk.
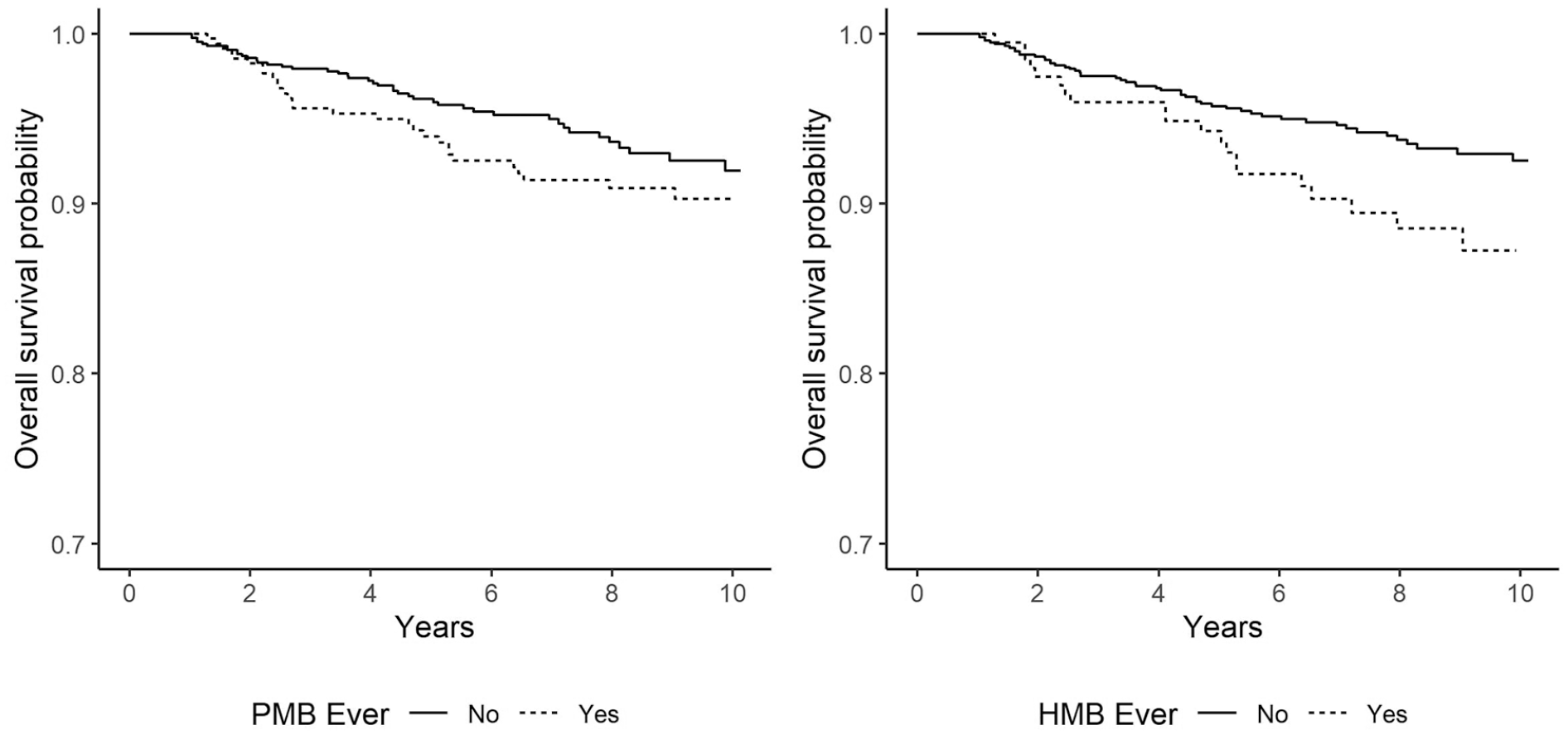
Unadjusted Kaplan–Meier survival curves for having a hysterectomy associated with PMB and HMB.
Unadjusted and adjusted hazard ratios and 95% CI for hysterectomy for PMB and HMB, the Study of Women’s Health Across the Nation (N = 1200).
CI: confidence interval; HMB: heavy menstrual bleeding; PMB: prolonged menstrual bleeding.
Adjusted models include all variables with results in their respective columns.
Referent group is White, Chinese, and Japanese women.
Referent group is less than high school.
Referent group is not hard.
Referent group is never and former smokers.
Obesity is defined as body mass index ⩾30 kg/m2. Referent group is non-obese.
In multivariable models, after adjustment for pelvic pain, hormone use, and Black race, PMB remained associated with more than a two-fold increased hazard of hysterectomy (HR = 2.35, 95% CI = 1.20–4.61, Table 2). This hazard was attenuated (HR = 1.72) and no longer statistically significant when adjusted for life interference. The hazard for HMB associated with hysterectomy was not significant in multivariable models.
Each additional type of life interference due to bleeding was associated with a 50% increase in the hazard of hysterectomy (PMB model: HR = 1.52, 95% CI = 1.29–1.79; HMB model: HR = 1.56, 95% CI = 1.32–1.83). When we assessed potential mediation of the association between PMB and hysterectomy by life interference, the dynamic path analysis showed that the direct effect of PMB (not through life interference) did not reach significance over time (Figure 3, direct), whereas a significant cumulative indirect effect through life interference was observed that increased approximately linearly over time (Figure 3, indirect), indicating that the relationship between PMB and time to hysterectomy is largely and significantly mediated by reported interference of PMB at an approximately constant rate. Notably, even after adjustment for bleeding characteristics, pelvic pain, and hormone use, Black women continued to have an increased risk of hysterectomy. In addition, both pelvic pain and hormone use remained independently associated with the hazard of hysterectomy although the hazards were attenuated. In sensitivity analyses, results were similar when analyses were limited to those women with bleeding data during the early MT and when we excluded four women with cancer/suspicious mass (data not shown).

Results of dynamic path analysis of the association (black line) and 95% confidence interval (gray lines) between PMB and hysterectomy mediated through the level of life interference showing the direct effect of PMB, the indirect effect mediated through life interference and the total effect. The red dashed line is a reference line to better visualize when the confidence interval contains zero.
Discussion
This study assessed hysterectomy risk following PMB or HMB during the MT. Risk of hysterectomy overtime was more than two-fold higher in women who experienced PMB (at least three bleeding episodes lasting at least 8 days within 6 months), independent of pelvic pain, hormone use, and race or ethnicity. Adjustment for life interference attenuated the hysterectomy risk associated with PMB, with level of life interference an important mediator of the PMB-hysterectomy association. Each additional life domain negatively affected by bleeding was associated with a 50% increased hazard of hysterectomy. The hazard for women reporting HMB, although marginally elevated in unadjusted analyses, was not statistically significant.
PMB was more strongly associated with hysterectomy risk than HMB, suggesting that PMB may be a greater incentive for electing hysterectomy. Concordantly, one small cross-sectional study reported that during the MT, women perceived increased duration, but not amount, of menstrual flow as problematic. 14 A large 2-year prospective study of clinical practices reported that HMB resolved spontaneously in 8% of women aged 45–49 years and in up to 35% of women aged 50–54 years, although resolution was less likely in women who reported life interference. 15 Relevant to hysterectomy risk, among women presenting with AUB to an emergency facility PMB, but not HMB, was associated with moderate to severe anemia. 16 In this study, HMB was marginally associated with hysterectomy risk in unadjusted analyses. As women who had had a hysterectomy at the time of enrollment were excluded from the study, and only 6% of women subsequently reported having a hysterectomy, this study may not fully reflect the hysterectomy risk of women experiencing HMB as they transition to postmenopause. Prospective studies of changes in amount and duration of menstrual bleeding in women with fibroids and women who have a lifelong history of HMB as they approach the menopause are warranted.
Our analyses documented the impact of menstrual bleeding on women’s life during the MT: 65% reported interference with at least one life domain while 17% reported interference in all domains. Hysterectomy risk increased in concert with greater levels of life interference. Adjusting for life interference attenuated the risk for both PMB and HMB, indicating that AUB was associated with women’s decisions to choose hysterectomy based on its level of interference in their lives. This finding supports recommendations to incorporate quality of life evaluations into the definition and assessment of AUB.4,5
Despite being the definitive treatment for AUB, hysterectomy is considered a last resort intervention due to its economic cost and significant risks.17 –20 Medical therapies offer attractive “bridges” for peri-menopausal women who want to avoid hysterectomy. Knowing the amount of time remaining until their FMP would help women who are attempting to temporize with medical therapies until the permanent cessation of menses; new assays for Anti-Mullerian Hormone can help predict time to this event. 21 Although there have been treatment advances since these data were collected, treatments such as tranexamic acid are targeted at heavy bleeding and may increase the duration or frequency of light bleeding. Oral GNRH agonists may be used only for limited periods of time and thus may not resolve AUB permanently. Also, treatments such as uterine artery embolization may not be available in areas or in populations with limited health care access such that hysterectomy may be the only available option to resolve bleeding complaints. This article prospectively documents the presentation of AUB most likely to prompt definitive action in midlife.
Approximately 30% of women reported pelvic pain, which was associated with an 80% increased adjusted hazard of hysterectomy, independent of bleeding characteristics and life interference. Hormone use was associated with a 2.5-fold increase in the adjusted hazard of hysterectomy. This finding may indicate that hormone treatment did not adequately alleviate women’s bleeding problems. Alternatively, although estrogen-based hormone regimens are front-line therapies to alleviate menopausal symptoms, they also carry the potential adverse effect of causing or exacerbating AUB, especially prolonged bleeding.22,23
Independent of bleeding characteristics, pain, and life interference, in this study, Black women had an 80% increased risk of hysterectomy compared to Chinese, Japanese, and White women, consistent with prior literature.24 –26 Black women tend to have larger fibroids and heavier menstrual bleeding than White women and thus may experience worse fibroid-related symptoms (such as pain, bulk, and bleeding) prompting surgery.27 –29 Specifically, Black women are more likely to report higher bleeding severity scores and to have higher fibroid bulk scores than White women. 30 Alternatively, this finding may reflect disparities in care as Black women are less likely to be offered alternatives to hysterectomy,31,32 with evidence suggesting undertreatment of initial symptoms. 30 A study of hysterectomy trends from 2003 to 2010 reported that White women, women in the highest income quartile and women with private insurance were more likely to have laparoscopic hysterectomies than Black women, women in the lowest income quartile, and women on Medicaid, 33 similar to earlier findings from the Healthcare Cost and Utilization Project Nationwide Inpatient Sample. 34 Although racial disparities are not found in all studies, 35 a recent meta-analysis of 13 studies found that Black women were less likely to have minimally invasive surgery compared to White women. 36 Black veterans were less likely to receive any treatment for symptomatic uterine fibroids than White veterans, with the largest percentage differences observed among veterans with anemia. 37 Care-seeking for AUB and decisions about surgery may also be related to cultural factors. 38
Limitation
Age-eligible women who had reached their FMP (surgically or naturally) before recruitment were ineligible for the SWAN cohort. Furthermore, in the populations from which our cohort was recruited, age-eligible Black women were more likely than women in other ethnic/racial groups to have had a hysterectomy at the time of recruitment.39,40 Thus, left truncation may bias our findings resulting in underestimation of the hysterectomy risk associated with HMB. Finally, we did not do a power analysis; these were secondary analyses of cohort data; thus, the sample size was fixed.
Our study also had several strengths. It is one of the first prospective, community-based studies to evaluate hysterectomy risk associated with PMB or HMB during the MT. Inclusion of relatively large samples of multiple racial and ethnic groups enhanced generalizability and statistical power to detect modest but meaningful associations.
In conclusion, PMB during the MT was associated with increased hysterectomy risk; the degree to which PMB interfered with a woman’s life was a key contributor to that risk. These findings suggest several strategies that could reduce the use of hysterectomy during the MT. First, public health outreach to educate women about commonly experienced increases in amount and duration of menstrual flow during the MT, and the range of therapies available for these symptoms, could facilitate knowledgeable interactions with the health care system. Second, health care providers should counsel women experiencing AUB about medical interventions that may permit them to complete the MT without undergoing hysterectomy. More wide-scale dissemination of new clinical tools that help estimate the remaining time until FMP would allow perimenopausal women who are weighing medical versus surgical options for AUB to make more informed decisions.
Supplemental Material
sj-pdf-1-whe-10.1177_17455057251351418 – Supplemental material for The relation of heavy or prolonged bleeding during the menopause transition to risk of hysterectomy
Supplemental material, sj-pdf-1-whe-10.1177_17455057251351418 for The relation of heavy or prolonged bleeding during the menopause transition to risk of hysterectomy by Siobán D. Harlow, Michelle M. Hood, Alain Mukwege, John F. Randolph, Ellen B. Gold, Michael R. Elliott, Alaina C. White and Gail A. Greendale in Women’s Health
Footnotes
Acknowledgements
Clinical Centers: University of Michigan, Ann Arbor, MI – Carrie Karvonen-Gutierrez, PI 2021–present; Siobán Harlow, PI 2011–2021; MaryFran Sowers, PI 1994–2011; Massachusetts General Hospital, Boston, MA – Sherri-Ann Burnett-Bowie, PI 2020–present; Joel Finkelstein, PI 1999–2020; Robert Neer, PI 1994–1999; Rush University, Rush University Medical Center, Chicago, IL – Imke Janssen, PI 2020–present; Howard Kravitz, PI 2009–2020; Lynda Powell, PI 1994–2009; University of California, Davis/Kaiser, CA – Elaine Waetjen and Monique Hedderson, PIs 2020–present; Ellen Gold, PI 1994–2020; University of California, Los Angeles, CA – Arun Karlamangla, PI 2020–present; Gail Greendale, PI 1994–2020; Albert Einstein College of Medicine, Bronx, NY – Carol Derby, PI 2011–present; Rachel Wildman, PI 2010–2011; Nanette Santoro, PI 2004–2010; New Jersey Medical School, University of Medicine and Dentistry, Newark, NJ – Gerson Weiss, PI 1994–2004; and the University of Pittsburgh, Pittsburgh, PA – Rebecca Thurston, PI 2020–present; Karen Matthews, PI 1994–2020. NIH Program Office: National Institute on Aging, Bethesda, MD – Rosaly Correa-de-Araujo 2020–present; Chhanda Dutta 2016–present; Winifred Rossi 2012–2016; Sherry Sherman 1994–2012; Marcia Ory 1994–2001; National Institute of Nursing Research, Bethesda, MD – Program Officers. Central Laboratory: University of Michigan, Ann Arbor, MI – Daniel McConnell (Central Ligand Assay Satellite Services). Coordinating Center: University of Pittsburgh, Pittsburgh, PA – Maria Mori Brooks, PI 2012–present; Kim Sutton-Tyrrell, PI 2001–2012; New England Research Institutes, Watertown, MA – Sonja McKinlay, PI 1995–2001. Steering Committee: Susan Johnson, Current Chair, Chris Gallagher, Former Chair. We thank the study staff at each site and all the women who participated in SWAN.
Ethical considerations
The protocol of the study received Institutional Review Board approval, and participants provided written, informed consent at each visit. Procedures of this study now receive ethical approval through a single IRB mechanism. The governing sIRB is The University of Pittsburgh Institutional Review Board, and the human subjects protocol number is STUDY21010146. The referring ethical review boards at the additional clinical sites are listed below. Northern California – Institutional Review Board Administration, University of California at Davis and Institutional Review Board for the Protection of Human Subjects, Kaiser Foundation Research Institute. Los Angeles, California – Office of Human Research Protection, University of California at Los Angeles. Michigan – The Health Sciences and Behavioral Sciences Institutional Review Boards, University of Michigan. Boston, Massachusetts – Partners Human Research Committee (PHRC), Partners HealthCare System. New Jersey – Office of Human Research Affairs (OHRA), Albert Einstein College of Medicine. Chicago – Institutional Review Boards, Rush University Medical Center.
Author contributions
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Study of Women’s Health Across the Nation (SWAN) has grant support from the National Institutes of Health (NIH), DHHS, through the National Institute on Aging (NIA), the National Institute of Nursing Research (NINR), and the NIH Office of Research on Women’s Health (ORWH); grants U01NR004061; U01AG012505, U01AG012535, U01AG012531, U01AG012539, U01AG012546, U01AG012553, U01AG012554, U01AG012495, and U19AG063720). The content of this article is solely the responsibility of the authors and does not necessarily represent the official views of the NIA, NINR, ORWH, or the NIH.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Study of Women’s Health Across the Nation data are archived at https://www.icpsr.umich.edu/web/ICPSR/series/00253 and at the National Institute of Aging’s Aging Research Biobank at ![]() .
.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.