
Abstract
Clevidipine is a third generation dihydropyridine calcium channel blocker recently approved by the Food and Drug Administration and is an emerging option for management of perioperative hypertension. This intravenous medication has several properties that may be advantageous when rapid and safe blood pressure control is required, including fast onset, short duration of action and the lack of renal or hepatic metabolism. Clevidipine has been demonstrated to be safe and efficacious for the management of perioperative hypertension in the cardiac surgery population, with minimal excursions outside of the target blood pressure range. Despite the fact that clevidipine does have certain advantages over alternative agents, it has some distinct limitations associated with its use, including higher associated costs and limited data in non-cardiac surgery patients. While clevidipine may serve as an additional option, further research is required to fully establish the role of clevidipine in the management of perioperative hypertension.
Introduction
Hypertension is one of the most common chronic medical conditions, affecting as many as 1 billion people worldwide. 1 The Seventh Report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure (JNC7) defines hypertension as a systolic blood pressure (SBP) of ≥140 mmHg or diastolic blood pressure of ≥90 mmHg. In the United States, approximately 30% of the adult population has been diagnosed with hypertension. Hypertension puts this population at risk for chronic kidney disease, heart failure, myocardial infarction and cerebrovascular incidents and is associated with increased morbidity and mortality. 1
The management of hypertension is of major clinical importance in patients requiring surgical procedures. Perioperative hypertension increases the risk of intraoperative and postoperative complications similar to those associated with chronic hypertension.2,3 Additional consequences of perioperative hypertension include bleeding complications, hypoxia, hypothermia, and end organ failure in the postoperative phase. One quarter of patients with chronic hypertension undergoing surgery will experience elevated blood pressures perioperatively.3,4 Patients with chronic hypertension are often required to refrain from taking oral antihypertensive therapy the morning of surgery, putting them at risk of hypertension in the perioperative setting. 5 Although patients with chronic hypertension are at higher risk of increased blood pressures in the perioperative setting, normotensive patients are also at risk due to factors associated with anesthesia and surgery. Hypertension can be seen with the induction of anesthesia, leading to acute elevation in blood pressure of up to 30 mmHg in normotensive patients and up to 90 mmHg in patients with chronic hypertension. 2 As the stages of anesthesia progress, sympathetic nervous system inhibition and the effects from the anesthetic agents can cause blood pressures to fall. Decreases of up to 30 mmHg can be seen in normotensive patients, with more pronounced reductions in those with preexisting hypertension of up to 60 mmHg. 3 Postoperatively, fluctuations in fluid status, hypothermia, and sympathetic stimulation from pain can all be associated with development of hypertension.
There are many pharmacologic options available for the treatment of perioperative hypertension, including vasodilators, beta-adrenergic blockers, and calcium channel blocking agents. Severe blood pressure elevations (.180/110 mmHg) with evidence of impending or progressive target organ damage are classified as hypertensive emergencies. Examples of target organ damage include hypertensive encephalopathy, intracerebral hemorrhage, acute myocardial infarction, acute heart failure with pulmonary edema, unstable angina, dissecting aortic aneurysm, or eclampsia. 1 Hypertensive emergencies require immediate blood pressure reduction with a goal of no more than 25% reduction within 1 hour, and then to <160/100 within 2–6 hours. Frequently hypertensive emergencies require continuous infusions of intravenous agents such as vasodilators, beta-blockers, or calcium channel blockers. In contrast, hypertensive urgency (blood pressure elevations >180/110 without evidence of target organ damage) can be treated less aggressively with bolus doses of antihypertensives or oral therapies when possible. Ideal agents are easily titrated with rapid onset of action and short duration of action for precise and predictable blood pressure control. Current literature supports the efficacy and safety of many agents including nitroglycerin, sodium nitroprusside, esmolol, labetalol, and nicardipine. 5
Although these agents have been shown to be safe and effective in the treatment of perioperative hypertension, there are some unfavorable characteristics associated with current treatment options. The vasodilator nitroglycerin acts as a venodilator, reducing preload and cardiac output. These reductions are unfavorable in patients with decreased renal and cerebral perfusion. Nitroglycerin has an onset of action of 2–5 minutes and duration of action of up to 20 minutes. Reflex tachycardia is not uncommon with nitroglycerin therapy. Sodium nitroprusside acts as both a venous and arterial dilatory agent, which can cause profound hypotension in some patients. The onset and duration of action of sodium nitroprusside are very rapid, allowing for tight blood pressure control; however, extended therapy can lead to rebound hypertension. 6 Sodium nitroprusside therapy can also lead to cyanide and thiocyanate accumulation and toxicity. While beta-blockers can be especially useful in controlling perioperative hypertension, they can lead to a reduction in heart rate that may be detrimental in patients with existing bradycardia, heart block, or asthma. 7 Dihydropyridine calcium-channel blockers have been used successfully to control blood pressure during surgery.8,9 Although nicardipine has demonstrated adequate control of perioperative hypertension, it delivers a large amount of fluid at typical doses required to control blood pressure.
Clevidipine is a third generation dihydropyridine calcium channel blocker recently approved by the Food and Drug Administration and is an emerging option for management of perioperative hypertension. This intravenous medication has several properties that may be advantageous when rapid and safe blood pressure control is required. The lipophilic properties of clevidipine provide rapid onset of action while metabolism by esterases in the blood and tissue impart a short duration of action; both allowing for tight control of blood pressure. Studies have shown rapid achievement of goal blood pressure with limited deviation from target blood pressure ranges. Although these properties are favorable, clevidipine use may be limited by distinct administration requirements and increased cost over other alternative agents.
Pharmacology of Clevidipine
Mechanism of action
Clevidipine butyrate exerts antihypertensive effects by antagonism of the L-type calcium channels. The L-type calcium channels are expressed at low levels in cardiac cells and high levels in vascular cells. 10 These voltage gated channels are responsible for regulation of calcium influx during membrane depolarization. 11 Like other third generation dihydropyridine calcium channel blocking medications, clevidipine prevents calcium influx during depolarization in arterial smooth muscle. 12 From this inhibition, intracellular phosphodiesterase is blocked resulting in an increase in guanosine monophosphate. This is responsible for inhibition of smooth muscle contractility associated with coronary, pulmonary, and systemic arterial vasodilation, as well as inhibition of myocardial contractility and cardiac conduction.13,14
Clevidipine decreases arterial blood pressure by reducing systemic vascular resistance without changes in cardiac filling pressures (preload).15,16 Studies evaluating the safety and efficacy of clevidipine have shown that it produces arterial vasodilation without negative inotropic or chronotropic effects.14,17 Consistent with other dihydropyridine calcium channel blockers, clevidipine may also have diuretic properties due to a direct inhibition of renal tubular reabsorption. 16
Pharmacokinetic and metabolism profile of clevidipine
Clevidipine is formulated as an oil-in-water emulsion made with soy bean oil and egg yolk phospholipids, as it and is nearly insoluble in water with solubility of 0.1 mg/mL. 12 The intravenous product is composed of two enantiomers R- and S-clevidipine. 18 Each enantiomer possesses equipotent antihypertensive activity. Initial pharmacokinetic studies showed a mean blood clearance of 0.14 L/min/kg and a volume of distribution at steady state of 0.6 L/kg. 19 Clevidipine is highly protein-bound in humans (~99.7%). 20
Pharmacokinetic dose-finding studies have demonstrated a linear relationship between dose and arterial blood concentration, with steady-state arterial blood levels seen within 2 minutes. 16 Clevidipine has been shown to produce a decrease in SBP within 2–4 minutes of infusion initiation in healthy volunteers at a dose rate of 1–2 mg/hour. 14 In the ESCAPE-1 study evaluating the efficacy of clevidipine, treated patients had ≥15% lowering of arterial blood pressure at a median time of 6 minutes.14,17
Clevidipine is metabolized in the blood and tissue by esterases to inactive metabolites carboxylic acid metabolite and formaldehyde, and its elimination is therefore unaffected by renal or hepatic dysfunction. 1 Esterase metabolism also gives clevidipine an ultra short elimination half life of less than one minute, lending the medication to rapid and tight blood pressure control. Pharmacokinetic studies have shown a 50% reduction of the concentration of clevidipine 1 minute after infusion termination and 90% reduction 5 minutes after termination. 21 The terminal phase half-life has shown to range from 4–21 minutes, but the aforementioned pharmacokinetic studies suggest that the terminal phase may be of very little importance. 21 Patients treated with a short infusion experienced a return to baseline arterial blood pressure and heart rate within 15 minutes of discontinuation of clevidipine.21,22
Clinical Studies
Cardiac surgery
Patients undergoing cardiac surgery are at increased risk for perioperative blood pressure lability with up to 80% of patients experiencing acute perioperative hypertension and up to half requiring intravenous antihypertensive interventions.23,24 Perioperative blood pressure elevation in this population is a significant clinical problem as it directly and indirectly contributes to increased postoperative morbidity and mortality with elevated risk of myocardial infarction due to increased oxygen demands, as well as higher risk of bleeding and neurologic complications.25–27 Based on these risks, the cardiac surgery population has been a focus of the majority of the data evaluating the use of clevidipine in the perioperative setting.
In a dose finding study conducted by Bailey and colleagues, postoperative cardiac surgery patients were randomized to treatment with clevidipine or placebo. 15 Patients treated with clevidipine were randomized to one of six different doses of clevidipine (0.05, 0.18, 0.32, 1.37, 3.19, or 9.58 mcg/kg/min). In the dose finding phase of treatment, the investigator increased the infusion rate to the randomized dose within 12 minutes. Hemodynamics were observed from 12–22 minutes. During this phase, the dose was increased to the next dose if the mean arterial blood pressure (MAP) exceeded 105 mmHg or decreased if the MAP was less than 65 mmHg. Patients who still met these hemodynamic criteria after the dosing change were removed from the study.
After the initial dose finding phase, the patients received the dose of clevidipine for the next 100 minutes. If the MAP was not maintained between 75–95 mmHg, the patient was removed from the study. Arterial blood samples were taken at points throughout the infusion and after clevidipine discontinuation. Hemodynamic data was then compared to arterial blood concentrations of clevidipine. Results of this analysis suggested an appropriate starting dose of clevidipine may be between 0.32 and 1.37 mcg/kg/min.
The efficacy and safety of clevidipine was assessed in two multicenter, double blind, placebo-controlled studies in cardiac surgery patients; in the preoperative setting in ESCAPE-1 (n = 105) and the postoperative period in ESCAPE-2 (n = 110).14,17 In both studies, patients were eligible for inclusion if they were undergoing coronary artery bypass grafting, with or without valve replacement.
In ESCAPE-1, patients received either clevidipine 0.5 mg/mL (n = 53) or placebo of 20% lipid emulsion (n = 52) for at least 30 minutes pre-operatively. The infusion was initiated at a rate of 0.4 mcg/kg/min (approximately 2 mg/hr in an 80 kg patient) and titrated to effect as tolerated by doubling the dose every 90 seconds up to a rate of 3.2 mcg/kg/min. Above this rate, clevidipine was titrated in increments of 1.5 mcg/kg/min up to a maximum rate of 8 mcg/kg/min. The study drug was infused for at least 30 minutes. Goal blood pressure was defined as a reduction of at least 15% from a baseline SBP of at least 160 mmHg. Treatment failure was defined as premature or permanent discontinuation of study drug for any reason or failure to decrease blood pressure to target within 30 minutes. Patients in the clevidipine group experienced a significantly lower treatment failure rate as compared to those treated with placebo (7.5% vs. 82.7%, P < 0.0001). In the ESCAPE-1 trial, target blood pressure in the clevidipine group was achieved at a median time of 6 minutes (95% confidence interval 6–8 minutes). 14
Sixty percent of patients in the clevidipine group attained their target blood pressure with infusion rates of less than 3.2 mcg/kg/min. It is important to mention that 26 (24.8%) patients in this trial received preoperative beta-blockers or vasodilators prior to clevidipine initiation; however this was well balanced between the treatment (14 patients) and placebo (12 patients) groups. Only 2 (3.8%) patients received concomitant beta-blockers or vasodilators during clevidipine administration compared to 10 (19.2%) in the placebo group.
The ESCAPE-2 trial evaluated the use of clevidipine in cardiac surgery patients postoperatively. 17 Definitions for target blood pressure range and treatment failure were identical to those used in the ESCAPE-1 trial. Of the 110 patients who qualified for treatment, 61 patients received clevidipine and 49 received placebo (20% lipid emulsion). The dosing regimen for clevidipine treatment was also the same as described in the ESCAPE-1 trial. Consistent with ESCAPE-1, there was a significantly lower treatment failure rate with clevidipine (8.2%) as compared to the placebo group (79.6%, P < 0.0001). The median time to goal blood pressure in the clevidipine group was 5.3 minutes (95% confidence interval, 4–7 minutes). Of those treated, 94.7% of patients achieved target SBP at an infusion rate of ≤3.2 mcg/kg/min. However, concomitant vasodilators were required in 41% of patients in the clevidipine group within the first 30 minutes of clevidipine infusion.
While ESCAPE-1 and ESCAPE-2 trials compared the efficacy and safety of clevidipine to placebo, the first evidence comparing clevidipine to other antihypertensives came from a small prospective trial of patients undergoing elective coronary artery bypass grafting. 28 In a multicenter, double blind-double dummy study, Powroznyk and colleagues randomized 30 patients with MAP greater than 90 mmHg for at least 10 minutes postoperatively to either clevidipine or sodium nitroprusside. Clevidipine was initiated at 0.3 mcg/kg/min and sodium nitroprusside at 0.5 mcg/kg/min and were titrated to maintain a MAP of 70–80 mmHg for the duration of the 3 hour infusion. Patients who maintained a MAP > 150 mmHg despite maximized infusion rates of 8 mcg/kg/min were terminated from the study and open treatment was initiated. This comparison found that there was no difference in the efficacy in controlling MAP, and the two agents had similar excursions outside of the target pressure goal. There were also no differences in the number of rate adjustments required during the first 30 minutes or the last 150 minutes of infusion. However, study infusion was discontinued in one patient in the clevidipine group due to inadequate blood pressure control. While efficacy in blood pressure management was similar between clevidipine and sodium nitroprusside, other hemodynamic changes including tachycardia and decreases in stroke volume were less significant with clevidipine.
ECLIPSE was the first large study to evaluate the efficacy of clevidipine as compared to other antihypertensive agents (nitroglycerin, sodium nitroprusside and nicardipine) in the perioperative period. 9 ECLIPSE consisted of three parallel multicenter open label studies in which adult patients undergoing cardiac surgery were randomized in a 1:1 fashion to clevidipine or one of the comparator agents. For the comparison of clevidipine vs. nitroglycerin and clevidipine vs. sodium nitroprusside, study drug was initiated in either the preoperative or intraoperative setting; while for clevidipine vs. nicardipine, study drug was initiated during the postoperative period only. For all three study arms, clevidipine was initiated at 0.4 mcg/kg/min and was titrated by doubling the infusion rate every 90 seconds up to a rate of 3.2 mcg/kg/min. Infusion rates beyond 3.2 mcg/kg/min were titrated based on patient response in increments of 1.5 mcg/kg/min to a maximum rate of 8 mcg/kg/min. Dosing and titration of the comparator agents was performed at the discretion of the investigator based on standard practice. Efficacy of blood pressure control was assessed using the area under the curve analysis of blood pressure excursions normalized per hour (AUCSBP-D). Baseline characteristics were similar among all groups with a high percentage of patients with pre-existing hypertension and cardiac disease. The median infusion rate for clevidipine was 3.1 mg/hr [interquartile range 2.2–5.1] with a median duration of 6.4 hours [interquartile range 6.3–74.2]. When the pooled data from the entire clevidipine cohort (n = 751) were compared to the pooled comparator group (n = 756), clevidipine was significantly more efficacious at maintaining SBP within the predetermined ranges of 75 to 145 mmHg pre- and postoperatively and 65–135 intraoperatively (median AUCSBP-D 3.79 vs. 7.79, P = 0.0004). When these target ranges were tightened to 105 to 145 mmHg pre- and postoperatively and 95 to 135 mmHg intraoperatively in a post hoc analysis, clevidipine still maintained more time within the specified range as compared to the other pooled agents (median AUCSBP-D 87.7 vs. 111.5, P = 0.002). In the analysis of the individual comparator agents, both sodium nitroprusside and nitroglycerin resulted in significantly more excursions outside of the target range as compared to clevidipine (median AUCSBP-D 8.87 vs. 4.41, P = 0.0006 and 10.5 vs. 4.37, 0.0027 respectively). For sodium nitroprusside the excursions occurred both above and below the target range while nitroglycerin specifically had more excursions above the range. Unlike the other two comparator agents, nicardipine resulted in similar efficacy in maintaining target blood pressure to clevidipine (median AUCSBP-D 1.8 vs. 1.7, P = 0.8508). However, when the target range was narrowed in the post hoc analysis, clevidipine had fewer excursions than nicardipine outside of the range of 105 to 145 mmHg postoperatively (median AUCSBP-D 77.0 vs. 101.6, P = 0.0231). Assessment of time to reaching target blood pressure range, treatment failure and requirement for additional agents were not reported in the ECLIPSE trial.
These studies demonstrate that clevidipine is effective in the cardiac surgery population. In addition, when compared to current agents used for the management of perioperative hypertension, clevidipine may have distinct advantages with fewer excursions outside of a targeted blood pressure range.
Neurosurgery
Clevidipine has also been shown to be safe and effective in neurosurgical procedures wherein rapid control of blood pressure is essential to avoid perioperative complications such as hemorrhage or ischemia. The effects of the calcium-channel blocker were first evaluated in intracranial surgery patients in a single center, prospective trial. 29 The primary endpoint of this trial was the proportion of patients in whom the target SBP of <130 mmHg could be achieved using clevidipine as the sole antihypertensive agent. The secondary endpoints included the amount of time required to achieve the target blood pressure and documentation of other antihypertensives used to control blood pressure perioperatively. Blood pressures and heart rate were monitored perioperatively via an arterial line and recorded every 5 minutes intraoperatively and every 15 minutes postoperatively. Patients were premedicated with 2 mg of midazolam preoperatively. Anesthesia was induced with propofol (1.5–2 mg/kg), lidocaine (0.5–1 mg/kg) and fentanyl (≤5 mcg/kg) and maintained with propofol (17 cases) or sevoflurane and remifentanil (4 cases, rate not reported) and titrated to a Bispectral Index of 50. Additional doses of fentanyl were also administered intermittently during surgery.
Clevidipine was initiated at a rate of 10 mg/hour and was continued for a minimum of 90 minutes in the post anesthesia recovery unit (PACU). Titration occurred for SBP > 130 mmHg or <90 mmHg, or heart rate < 40 beats per minute (bpm) or >90 bpm. Increases in blood pressure attributed to painful stimuli were treated by increasing the rate of remifentanil infusion or administration of bolus doses of fentanyl. Of the 22 patients enrolled, 21 patients required treatment with clevidipine and 7 of these patients had a history of chronic hypertension. Of the patients treated with clevidipine, 1 patient required clevidipine prior to induction, 19 required initiation of treatment intraoperatively, and one patient only required clevidipine post-operatively. Clevidipine alone achieved target systolic blood pressure < 130 mmHg in 17 of the 21 patients treated (81%). During clevidipine infusion, 28 hypertensive episodes were identified. In episodes that necessitated supplemental antihypertensive agents, three patients received labetalol and 1 received the combination of labetalol and hydralazine. Doses of these additional antihypertensive medications were not reported. Sixteen patients received concomitant metoprolol for instances of tachycardia that was not necessarily related to inadequate blood pressure control. In 50% of hypertensive episodes, target SBP was attained within 5 minutes, with 78.6% reaching target within 15 minutes. The total amount of clevidipine required to achieve target SBP was 7.6 ± 10.1 mg intraoperatively and 15.3 ± 18.8 mg postoperatively in PACU. Mean rates of infusion were not reported for the intraoperative period. The mean rate of infusion during the 90 minute interval in the PACU was 10.2 mg/hr.
Clevidipine has also been evaluated for perioperative blood pressure management in adolescents undergoing spinal fusion surgery. 30 A retrospective cohort analysis included 20 children ranging in age from 14–18 years old and from 46–96 kilograms. The goal MAP was 50–65 mmHg during the cases. Anesthesia was induced using either sevoflurane or propofol (3–4 mg/kg) and was maintained using continuous infusions of propofol (initial doses ranging from 100–120 mcg/kg/hr), remifentanil (0.1–0.3 mcg/kg/min titrated to goal MAP of 50–65), and dexmedetomidine (starting dose of 0.5 mcg/kg/hr). Each patient also received 500 mL of hydroxyethyl starch prior to the procedure and lactated ringer's fluid throughout at varying rates.
Clevidipine was initiated if remifentanil titration alone did not achieve the goal MAP of 50–65 mmHg. Infusion of the antihypertensive was started at 0.5 mcg/kg/min in 4 patients and at 1 mcg/kg/min in the remaining 16 patients. Clevidipine was titrated by increasing the rate of infusion by 0.5–1 mcg/kg/min every 2–3 minutes to achieve the goal pressure. Goal MAP was achieved in all patients in less than 10 minutes (mean 4.75 minutes) with rates ranging from 1–5 mcg/kg/min (mean 2.9 mcg/kg/min). MAP returned to baseline in ≤5 minutes in 16 patients and in ≤10 minutes in all patients. Three patients were treated with a beta-blocker to control heart rate during clevidipine infusion. Four adolescents included in the cohort experienced an increase in heart rate of greater than 20 bpm. It was not reported if other anti-hypertensive agents were used to control blood pressure or heart rate, nor was it reported if clevidipine was continued post-operatively. Two studies reported similar infusion rates of clevidipine to control blood pressure in pediatric aged patients.30,31
While there are currently no published studies evaluating the efficacy and/or safety of clevidipine for management of perioperative blood pressure in patients with cerebral artery aneurysms, Meyer and Tobias reported on their preliminary experience with clevidipine in three patients undergoing coiling for cerebral aneurysms in the interventional radiology suite. 32 Two cases involved initiation of clevidipine during anesthetic emergence and the third case describe initiation intraoperatively. In all three cases, initiation of clevidipine infusion at rates from 2–8 mg/hr resulted in blood pressure control within 2–7 minutes. In addition, minimal reflex tachycardia was observed with increases in heart rate of approximately 8–10 bpm after infusion initiation.
Although neurosurgical procedures frequently call for rapid and tight blood pressure control to minimize hemorrhagic and ischemic complications, more data is needed to support the use of clevidipine in this population. Currently the data has demonstrated that clevidipine is safe to use in select neurosurgical populations, however no studies have been published to date to compare efficacy to current standards of practice.
Dosing
Based upon the pharmacokinetic properties of clevidipine, the intravenous anti-hypertensive is useful in achieving target blood pressure goals quickly. The recommended rate of initiating clevidipine infusion is 1–2 mg/hr. The dose may be quickly titrated by doubling of infusion rate at 90 second intervals until the patient's blood pressure nears the target range. As the blood pressure approaches the goal, titration of clevidipine should be approached more conservatively with smaller infusion rate increases every 5–10 minutes. Desired therapeutic response is typically achieved in patients at infusion rates ranging from 4–6 mg/hr. The maximum dose of clevidipine was less than 16 mg/hr in most clinical trials; however, doses were escalated to 32 mg/hr in some patients with severe hypertension.14,17
Administration of Clevidipine
Aseptic technique should be maintained while handling clevidipine. The vial of clevidipine should be gently inverted prior to use to ensure uniformity of the emulsion and inspected for particulate matter and discoloration. Due to the lipid emulsion composition of clevidipine, concern for microbial growth exists. Once punctured, it is recommended that the vial be discarded every 12 hours to prevent bacterial growth. The infusion tubing should also be changed every 12 hours if it contains medication that has been infusing within that 12 hour time interval. Clevidipine can be infused via peripheral or central line. 12
Clevidipine is photosensitive and should be stored in a dark refrigerated environment of 2 °C–8° C (36 °F–46 °F). Vials can be transferred to USP controlled room temperature for a period not exceeding 2 months. 1 Once removed from refrigeration, the vials should remain at room temperature. 12
Due to the lack of compatibility data, the manufacturer of clevidipine recommends that the medication should not be administered in the same line as other medications. Although clevidipine should not be diluted, it can be administered with sterile water for injection, 0.9% sodium chloride, 5% dextrose, lactated ringers solution, and 10% amino acids. 12
Precautions and Contraindications
Clevidipine is poorly water soluble and is therefore formulated as a 20% lipid emulsion with the same constituents as intravenous fat emulsion (Intralipid) used in total parenteral nutrition.12,22,33 The lipid emulsion formulation presents additional challenges. Disadvantages of the lipid emulsion include risks of hypertriglyceridemia and pancreatitis, emulsion instability, and the inherent risks for contamination and infection. Clevidipine is contraindicated in patients with defective lipid metabolisms including lipid nephrosis, pathologic hyperlipidemia or acute pancreatitis secondary to hypertriglyceridemia. Concomitant lipid containing products including propofol and intravenous fat emulsion should be minimized to limit risk. Although clevidipine was found to have no effect of lipid levels in the VELOCITY and ECLIPSE trials, monitoring of triglycerides may be warranted, particularly in patients at increased risk for hypertriglyceridemia.34,35 Product labeling recommends that no more than 1 liter of clevidipine be infused per 24 hour period, due to the fact that each milliliter of the medication contains 0.2 grams (2 kcal) of lipid. 12 Due to the lipid emulsion, clevidipine is also contraindicated in patients with allergies to soybeans, soy products, eggs, or egg products.
Patients with aortic stenosis should not receive clevidipine due to the risk of reduced myocardial oxygen delivery from afterload reduction. 12 Similarly, caution should be used in patients with heart failure due to the negative inotropic effects associated with dihydropyridine calcium channel blockers. 12 However, a small subgroup analysis of 19 patients with acute heart failure from the VELOCITY trial appeared to safely decrease blood pressure without unexpected hypotension. 36
Clevidipine is pregnancy category C and in animal studies was linked to increased maternal and fetal mortality. Clevidipine has not been adequately evaluated in children (<18 years of age). 12 Rebound hypertension may occur after discontinuation, especially after prolonged infusions and in patients who are not transitioned to other antihypertensive agents. Therefore, patients should be closely monitored for at least 8 hours after clevidipine is discontinued. 12
Adverse Effects
Overall, clevidipine has been reportedly well tolerated. In healthy volunteers, the most commonly reported adverse effects (AE) were headache and feeling of warmth/flushing of mild to moderate severity.16,37 These effects occurred during the infusion and dissipated quickly once the infusion was discontinued. 37
The majority of safety data for clevidipine has been from the acute use of clevidipine in perioperative hypertension management in patients undergoing cardiac surgery. This population has inherent surgical risks that make it difficult to differentiate surgery related outcomes/complications from drug associated events.
As a potent vasodilator, clevidipine has the potential to cause systemic hypotension with reflex tachycardia. In two pharmacodynamic evaluations in healthy volunteers, clevidipine resulted in increases in heart rate by approximately 40% (from 59 to 82 bpm and from 53 to 75 bpm).19,21 In both studies, heart rate returned to baseline values within 10 to 15 minutes after discontinuation of the infusion.19,21 In ESCAPE-1, patients in both the clevidipine and placebo groups experienced increases in heart rate from a baseline of 71 and 76 bpm respectively to a maximum heart rate of 84 bpm in both groups. 14 Changes in heart rate were not observed upon termination of the infusion. No patients in ESCAPE-1 discontinued study medication due to safety concerns. The most common AE reported included fever (18.9% vs. 13.7%), atrial fibrillation (13.2% vs. 11.8%), acute renal failure (9.4% vs. 2.0%) and nausea (5.7% vs. 9.8%) although none of these reached statistical significance. In ESCAPE-2 there was no evidence of reflex tachycardia. 17 However, atrial fibrillation was more frequent in the clevidipine group (21.3% vs. 12.2%) and was the reason for study drug discontinuation in one patient. Two additional patients terminated the clevidipine infusion due to rapid decreases in SBP (from 140 to 100 mmHg in 3 minutes and from 140 to 108 mmHg in 5 minutes). Other common AE observed were nausea (21.3% vs. 12.2%), and insomnia (11.5% vs. 6.1%).14,17 Only one patient experienced a serious adverse event that was attributed to clevidipine (thrombophlebitis reported ~2 days post infusion administration). 17
While ESCAPE-1 and ESCAPE-2 allowed a maximum duration of clevidipine of only 1 hour, the median duration of infusion in ECLIPSE was 6.4 hours (range 2–16 hours). 9 With a longer infusion duration and comparison to nitroglycerin, sodium nitroprusside and nicardipine rather than placebo, the most common AE noted for clevidipine remained atrial fibrillation [33.6% vs. 32% (nitroglycerin), 36.1% vs. 32.2% (sodium nitroprusside), 35.6% vs. 35.2% (nicardipine)]. Other AE reported included renal dysfunction although rates were not significantly different than the comparator agents. Clevidipine was not associated with any increases in more serious outcomes including death, myocardial infarction, or stroke.
Based on the high rates of atrial fibrillation found in the evaluation of clevidipine in cardiac surgery patients, the manufacturer of clevidipine voluntarily suspended patient enrollment in the two Phase III safety trials in 2005 for an interim review of 880 patients. This more detailed review found similar rates of atrial fibrillation between clevidipine (34%) and comparator groups (31%) with no differences in duration, severity, treatment or outcomes. 38
In ECLIPSE, the primary safety endpoint evaluated was the 30 day incidence of death, stroke, myocardial infarction and renal dysfunction. There were no significant differences between the pooled clevidipine and pooled comparators groups for any of the 30 day safety endpoints. However, when analyzed as individual treatment cohorts, the sodium nitroprusside group had a significantly higher 30 day mortality rate compared to the clevidipine group (4.7% vs. 1.7%, P = 0.04).
While existing data supports the safety of clevidipine, atrial fibrillation rates should be monitored in patients during post-marketing surveillance. In addition, further research is needed to establish safety in non-cardiac surgery patients.
Drug Interactions
No studies have specifically evaluated drug interactions with clevidipine in vivo. In vitro studies have found that at clinically relevant concentrations, clevidipine and its carboxylic acid metabolite do not significantly inhibit or induce any cytochrome P450 enzymes. 39 Pharmacodynamic drug interactions have not yet been reported with clevidipine, although there is the potential for significant hypotension when combined with other vasodilators.
Cost
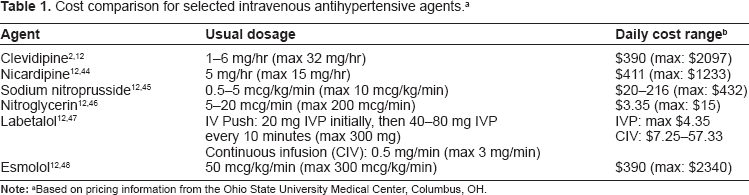
As a new brand name agent, clevidipine in one of the most expensive intravenous options available for the management of acute hypertension. Drug costs associated with clevidipine are similar to that of nicardipine and esmolol, while older agents including sodium nitroprusside, nitroglycerin and labetalol are significantly less expensive (Table 1). A cost-effectiveness evaluation for clevidipine has not yet been performed.
Cost comparison for selected intravenous antihypertensive agents. a
Ongoing Studies
As of September 2011, there are few ongoing studies that will expand the available evidence on the role of clevidipine in the perioperative arena. Currently there are five trials actively recruiting patients to evaluate clevidipine in patients with aneurysmal subarachnoid hemorrhage, acute aortic emergencies, acute heart failure, pulmonary hypertension and patients requiring ventriculostomy. All five are open label studies and four are single group assignment without a comparator group. A phase II single-center study (CLASH) is currently evaluating clevidipine in the management of acute hypertension in non-comatose patients with aneurysmal subarachnoid hemorrhage (Hunt and Hess grade 4 and lower). PRONTO is a phase II randomized trial recruiting a total of 140 patients with acute heart failure. Patients will be randomized to clevidipine or standard of care, and the primary outcome is the median time and percent of patients that attain the target blood pressure range and a 15% reduction in SBP within 30 minutes. One phase IV study is assessing the efficacy and safety of clevidipine for patients with intracerebral or subarachnoid hemorrhage who require ventriculostomy placement and acute hypertension management. A second phase IV trial (PROMPT) is recruiting approximately 30 patients with an acute aortic emergency (aneurysm, dissection or other aortic disease) that require intravenous antihypertensive agents to lower their blood pressure. The final ongoing trial is designed to evaluate the impact of clevidipine on pulmonary vascular resistance during invasive vasoreactivity testing in the cath lab for patients with pulmonary artery hypertension.
Two studies evaluating clevidipine have been completed and have not yet been published (SPRINT and ACCELERATE trials). A phase II study (SPRINT) evaluated the safety and efficacy of clevidipine bolus in patients undergoing cardiac surgery involving the use of cardiopulmonary bypass at two academic institutions. Enrollment was estimated to be 40 patients total allocated across three dosing cohorts from 125 to 500 mcg. The primary efficacy outcome for this study was the mean maximum absolute and percent change in SBP from baseline within 15 minutes of the clevidipine bolus. This study was completed in 2009 and the results of this analysis have not been published to date. The ACCELERATE trial is a multicenter, single-arm, phase II trial completed in 2010 that evaluated the safety and efficacy of clevidipine in patients with acute hypertension and intracerebral hemorrhage. An estimate of 40 patients were planned to be enrolled to receive clevidipine infusion starting at 2 mg/hour and then titrated by doubling the dose every 1.5 minutes to a maximum of 32 mg/hour to achieve a SBP between 140–160 mmHg. The primary outcome for this study is the median time to achieve the target SBP within 30 minutes of initiation of clevidipine.
Place in Therapy
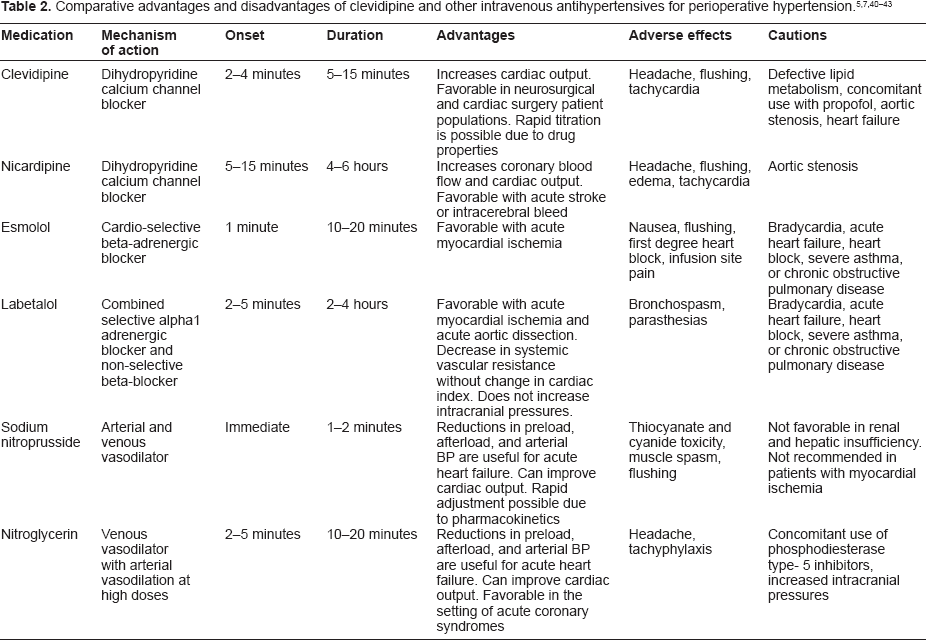
The ideal antihypertensive agent for perioperative hypertension should have a rapid onset, short duration of action, predictable effects, be cost effective, and be easily titrated. Currently there are many intravenous antihypertensive agents that can be used in the perioperative setting, each with advantages and disadvantages. Historically, preferred agents have included labetalol, esmolol, sodium nitroprusside and nicardipine. While there is a great deal of data and experience with these agents, clevidipine has certain advantages that make it an ideal agent for perioperative use including its pharmacokinetic profile with rapid onset and short duration of action, efficacy data demonstrating limited excursions outside of target blood pressure range, as well as the lack of renal and hepatic metabolism (Table 2). Despite the fact that clevidipine does have certain advantages over alternative agents, it does have some distinct limitations associated with its use. As a new agent, the primary shortcoming of clevidipine is the lack of data and experience in many non-cardiac surgery populations (ie, major vascular surgery, major trauma, renal transplantation, thoracic surgery, head and neck surgery, etc.). In addition, while data is available in neurosurgery patients as presented above, there is no data demonstrating superiority over other currently available agents such as nicardipine. Also, both the direct and indirect costs associated with clevidipine administration (drug cost, nursing costs, risks associated with lipid administration, etc.) put it at a marked disadvantage compared to other agents.
Conclusion
Clevidipine, a third generation intravenous dihydropyridine calcium channel blocker has demonstrated safety and efficacy in the preoperative, perioperative and postoperative setting in cardiac surgery patients and in select neurosurgical populations. Based on the need to balance the risks associated with uncontrolled perioperative hypertension and hypoperfusion secondary to medication related hypotension, clevidipine has the potential to play a significant role perioperatively with its unique pharmacokinetic profile and capability of stringent blood pressure control with minimal excursions. While the fast onset and short duration of activity make clevidipine an appealing option for perioperative use, further research is warranted regarding its efficacy and safety compared to other antihypertensives in other surgical populations. In addition, due to the higher costs associated with clevidipine, cost efficacy data is also needed in order to further assess its role within perioperative hypertension management.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.