
Abstract
Vigabatrin (Sabril®) has recently been granted approval in the Unites States for the adjunctive treatment of complex-partial seizures in adults. The drug was first evaluated as a potential therapy for this population decades ago, and it has been available in other parts of the world for some time. Well controlled studies demonstrate that at doses up to 3 g/day, the drug is efficacious as add-on therapy for treatment resistant seizures. However, vigabatrin has been associated with significant side-effects limiting its use, and relegating it to a late therapeutic alternative. Specifically, vigabatrin has been implicated in the development of irreversible peripheral vision loss in a significant number of patients. For this reason, the approval of the drug in the United States was contingent upon the introduction of a rigorous monitoring protocol that must accompany its use. Additionally, the drug has been associated with a relatively high incidence of psychiatric disturbances, although there is disagreement about a direct correlation of these symptoms to the drug. Still, the drug remains a viable alternative for patients who have failed therapy with traditional anti-seizure medications.
Introduction
Vigabatrin has been available in Europe since the late 1980's, and was approved for use in Australia and Canada in the early part of the 1990's, but only recently gained Food and Drug Administration (FDA) approval for use in the United States for the treatment of complex-partial (CP) seizures that have been proven refractory to standard therapies. Initially developed as an analog to γ-aminobutyric acid (GABA), the compound (γ-vinyl-GABA) was intended to bind irreversibly to GABA-transaminase (GABA-T) in an effort to limit the conversion of GABA to succinic semialdehyde, thus increasing GABA levels in the brain.1,2 This is significant in the realm of anti-epileptic medication in that GABA is the major inhibitory neurotransmitter in the human brain, and reductions have been associated with an increase in seizure potential.
CP seizures are among those most likely to be resistant to treatment, including multi-drug therapy. Vigabatrin represents an alternative add-on therapy for use in conjunction with traditional first-line agents such as carbamazepine, phenytoin and valproic acid to treat CP seizures that are unresponsive. Studies have shown that the drug is effective for many persons with refractory seizures, but the use of vigabatrin is not without its drawbacks.
Clinical Efficacy
Studies demonstrating the efficacy of vigabatrin for treatment-resistant CP seizures are plentiful. We conducted a Medline search limiting the results to prospective, double-blind, placebo controlled trials of vigabatrin in refractory CP seizures published since 1980. Eleven such trials were identified (Table 1).
Summary of studies evaluating vigabatrin efficacy in patients with refractory complex-partial seizures.
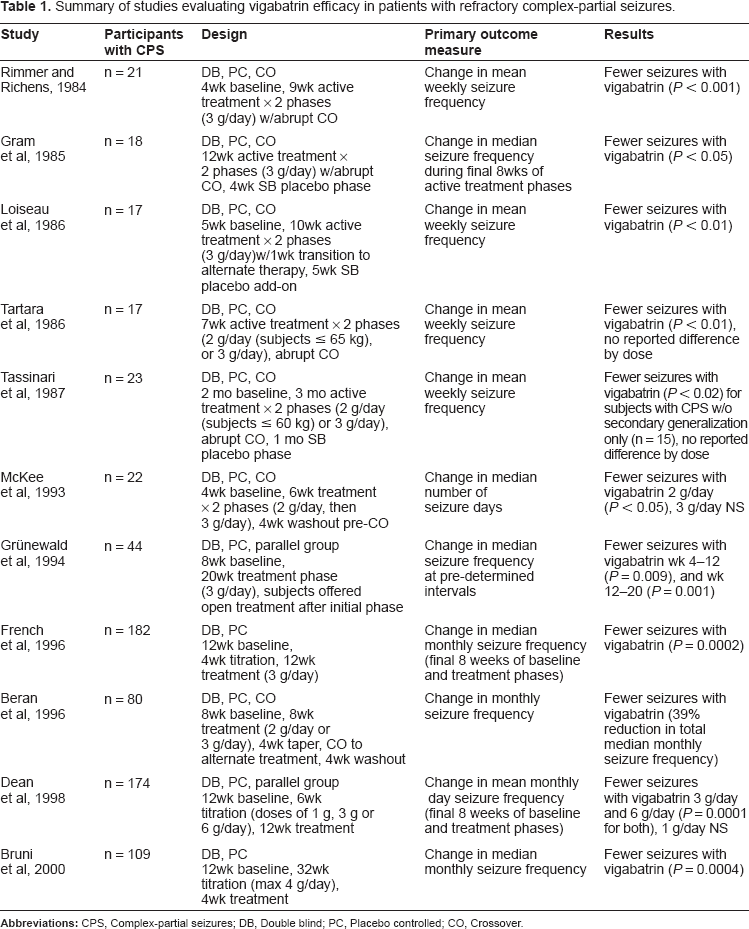
A 1984 crossover study by Rimmer and Richens was conducted to measure the effect of 3 g of vigabatrin in doses divided twice daily for patients with refractory epilepsy. 3 Twenty-one of 24 subjects, each with complex-partial seizures (with or without tonic-clonic seizures) completed the 22-week study. After a baseline period of four weeks, the patients (age 16–61 years) were given either vigabatrin or placebo for nine weeks before abrupt crossover to the alternate therapy. An average of 5.8 seizures per week was documented during the baseline period. Those individuals receiving the active drug demonstrated a drop in seizure number to 3.3 per week. Individuals in the placebo group showed no meaningful change in seizure frequency. The effect of vigabatrin was significant in comparison to both the baseline period, and the placebo arms (P < 0.001). Fourteen patients experienced a decrease in seizure frequency of at least 50%, and six had a 75% drop in occurrence.
The following year, Gram and colleagues published the findings of another study utilizing crossover design, and again comparing 3 g of vigabatrin to placebo. 4 All patients had complex-partial seizures, and were 17–63 years of age. The treatment phase consisted of 12 weeks of active drug or placebo with abrupt crossover to the alternate arm. However, to avoid the potential for carryover effects from the initial randomization, only seizures occurring in the final eight weeks of the treatment periods were considered in the analysis. The final period of the study was a single-blind placebo phase. Of 18 subjects completing the trial, eight and three experienced a decrease in seizure frequency of at least 50% and 75% respectively. The median number of seizures occurring while on placebo was 16 compared to nine while receiving vigabatrin (P < 0.05).
A study of 3 g per day of vigabatrin in patients 10–60 years of age with drug-resistant epilepsy was completed by Loiseau and colleagues during a four-phase study of cross-over design. 5 Seventeen of the patients completing the study had been diagnosed with CP seizures. After an initial five-week period of observation, the first of two 10-week treatment periods commenced. Crossover was completed utilizing the first week of the second treatment phase as a transition period. The final phase of the trial was a five-week single-blind period during which placebo was administered as add-on therapy to evaluate carryover and withdrawal. The average decrease in mean weekly seizure frequency with vigabatrin was 41% (10.7 for placebo vs. 6.3 for vigabatrin, (P < 0.01)). Nine patients with CP seizures experienced at least a 50% decrease in frequency.
A two-period crossover study utilizing weight-based dosing was completed by Tartara et al. 1 Of 20 patients studied, 14 had been diagnosed with CP seizures. Each of the treatment periods was seven weeks long. Subjects aged 16–65 years weighing 65 kg or less received 2 g vigabatrin per day (n = 15) in divided doses. Those weighing more than 65 kg were given 3 g. Considering the total group of 20 subjects, seizures decreased from 3.8 ± 3.7 per week to 2.2 ± 2.6 per week when comparing placebo to vigabatrin (P < 0.01). Taking into account only those with CP seizures (n = 17), the difference was also significant (2 ± 2.4 vs. 3.7 ± 3.8 for vigabatrin and placebo respectively, (P < 0.01)). Ten subjects with CP seizures experienced a decrease in seizure frequency of at least 50%. Separate analysis of the two doses of vigabatrin was not made available.
Thirty-one subjects (30 with partial seizures and one with myoclonic seizures) were enrolled in a study by Tassinari and colleagues that evaluated two doses of vigabatrin versus placebo. 6 Patients ranging in age from 10–58 years, 23 of whom had CP seizures with or without secondary generalization, or in conjunction with atonic seizures, underwent a two month run-in period followed by three months on vigabatrin or placebo with immediate crossover to the opposite therapy for an additional three months. Placebo was given to all subjects during the final month of the study in single-blind fashion. Weight based dosing was employed with patients stratified into groups receiving 2 g (those weighing up to 60 kg), or 3 g. The baseline seizure rate for the entire study population was 12.2 ± 17.8 per week. When analyzing all patients in the study, there was no significant change in seizure frequency when taking vigabatrin. However, a minimum 50% decrease in seizures was noted in 10 subjects, and a 25% decrease in frequency was experienced by an additional six. Of those subjects diagnosed with CP seizures without secondary generalization (n = 15), the decrease in seizures was significant (P < 0.02), and a full 40% were experiencing fewer than half as many seizures as they were at baseline.
A 1993 study conducted by McKee et al looked at two consecutive doses of vigabatrin in subjects aged 17–53 years to determine if a ceiling effect could be identified. 7 After a four-week run in period, each subject was given either placebo or 2 g of vigabatrin for six weeks. A four-week washout period was employed, and then subjects were randomized for a second six week treatment period with either placebo or 3 g of vigabatrin daily. There was an overall decrease in the number of days subjects experienced seizures with vigabatrin therapy (P < 0.05). However, when considering those patients with CP seizures, only the 2 g dose resulted in a significant change from baseline (10 days for placebo vs. 16 days for vigabatrin, P < 0.05). The 3 g dose failed to show a statistically significant change, with 20 and 24 days of demonstrated seizure activity for placebo and vigabatrin respectively. Of those with CP seizures 47% had their seizure frequency decrease by at least half. This is the sole study of vigabatrin 3 g that resulted in a non-significant change in seizure frequency. One possible explanation for the lack of efficacy of the 3 g dose includes decreased compliance on the higher dose, but pill counts did not support that theory.
Grünewald and colleagues published a study that evaluated 44 subjects between the ages of 15 and 61 years who had been diagnosed with CP seizures in a parallel-group, add-on fashion. 8 Either vigabatrin 3 g daily or placebo was given for 20 weeks during the initial double blind phase which was preceded by an eight-week baseline assessment period. During the final phase, all subjects were offered vigabatrin. The reduction in median seizure frequency was 66% through week 12 (P = 0.009), and 69% through week 20 (P = 0.001). Ten of 22 participants experienced a minimum 50% seizure reduction during the 20-week phase. Sustained improvement was demonstrated by six of seven subjects still undergoing active treatment at 44 weeks.
In a large multi-center study completed in the United States and submitted to the FDA as evidence of vigabatrin's efficacy in CP seizures, French et al examined the use of the drug in subjects 18–60 years of age. 9 The study was divided into three segments, the first of which was a 12 week run-in (the final eight weeks considered the baseline period). After randomization and a four-week titration period, subjects were exposed to 12 weeks of vigabatrin 3 g daily or placebo. The monthly frequency of seizures occurring during the final eight weeks of the active treatment period was recorded and analyzed. The median frequency was reduced by three seizures in the vigabatrin group compared to 0.8 seizures in the group receiving placebo (P = 0.0002), with 43% of subjects in the vigabatrin group experiencing a 50% or greater frequency reduction (P < 0.001).
A 1996 study conducted by Beran and colleagues was designed to characterize the vigabatrin dose best suited for CP seizure control. 10 Subjects age 16–65 years were enrolled in a five-phase trial. A screening and eight-week observation period comprised the first phase. Next, subjects were randomized to receive vigabatrin 2 g or 3 g daily, or placebo for eight weeks. Vigabatrin was then tapered over a four-week timeframe, and subjects were crossed over to active treatment or placebo as applicable. The final study phase was an additional four-week washout period. The median monthly reduction in seizure frequency with the active therapy was 39%. There was no difference in seizure rate between the two doses. The median number of seizure-free days was 22 with vigabatrin vs. 19 with placebo (P < 0.001). This study also considered seizure severity and duration during weeks five through eight of active drug administration, and this difference was also significant in favor of vigabatrin (P < 0.01).
The second of the two studies submitted to the FDA was another dose-response study, this time with exposure as high as 6 g of vigabatrin daily. 11 Dean et al enrolled 174 subjects 18–60 years of age. A twelve-week pre-treatment period ensued, followed by a six-week titration period to 1 g, 3 g or 6 g of vigabatrin per day, or placebo. Subjects then entered a maintenance period of 12 weeks. The seizure frequency during the final eight weeks of the pre-treatment and active-treatment periods were compared, and analyzed as 28-day segments. The 1 g dose did not result in a significant change compared to placebo. However, the 3 g and 6 g doses decreased seizure frequency (P = 0.0001 for both), though there was no difference between the two doses. All three doses of vigabatrin resulted in a significantly higher number of subjects experience at minimum 50% decrease in seizure frequency (placebo = 7%, 1 g = 24%, 3 g = 51% and 6 g = 54% (P < 0.0001 for all)).
The final study, conducted at ten Canadian locations evaluating vigabatrin use in subjects 16–50 years of age, was conducted by Bruni et al. 12 Subjects enrolled in a 12-week open baseline phase followed by a 32 week titration phase. Increases in vigabatrin dose maxed out at 4 g daily. Subjects not receiving placebo and experiencing no seizures on a given dose were increased to the next higher whole-gram dose. The maintenance phase lasted for an additional four weeks (for a total treatment period of 36 weeks). Median seizure frequency per 28 days decreased by 3.5 and 1 for vigabatrin and placebo respectively (P = 0.0004). The change in seizure-free days also favored vigabatrin (P = 0.0004). Almost half of those taking active drug demonstrated a minimum 50% decrease in seizure frequency.
Due to differences in study design, and because study participants with isolated CP seizures were not always evaluated separately, it is difficult to draw conclusions specific to that patient group. Pooling of data from the above studies using a random-effects model demonstrated that a 50% or greater decrease in the frequency of CP seizures was more likely in those receiving vigabatrin (relative risk estimated to be 2.58, 95% CI 1.87–3.57, intention to treat analysis). 13
Tolerability
When assessing a drug's therapeutic value, efficacy is not the only measure that need be considered. A patient's ability to tolerate the medication must also be taken into account as therapeutic success is only achievable with adherence to the prescribed regimen.
The majority of side-effects associated with the use of vigabatrin are very much in line with those reported by users of other anti-epileptic agents and centrally acting drugs. By far the most common side-effect reported in studies utilizing adult subjects is drowsiness. Other side-effects frequently reported include irritability, dizziness, headache and fatigue. Some also experienced weight gain.7,10–12 Tolerability of vigabatrin as reported in the previously summarized studies was generally high with few treatment withdrawals due to adverse events. Central nervous system side-effects were by and large transient.
Psychiatric disturbances with antiepileptic agents have recently been at the forefront of discussions about drug therapy for seizure control. Specifically, in 2008 the FDA issued a warning about an increase in suicidal ideation with antiepileptic drugs as a class. Four subjects in the summarized studies withdrew due to symptoms of depression.8,10 Two attempted suicides were also reported,9,11 though one of the subjects had a previous attempt prior to study participation. It should be noted that patients with seizure disorders report an increased rate of depression as a whole. 14 Recent studies have called the FDA findings into question, and it remains to be determined if the observed increase in suicidality is due to anti-epileptic drug therapy directly, or to an underlying depressive disorder.15,16 There does appear to be some evidence that a subset of the newer antiepileptic agents, of which vigabatrin is a member, is more likely to be associated with depression than are other drugs used to treat seizures. 16 In addition, vigabatrin has been linked to symptoms of psychosis. Two patients in the CP seizure studies were reported to have withdrawn due to the development of delusions, one due to paranoia and grandiose thinking, and one noted to have had symptoms consistent with schizophrenia.7,9,11,12 The prevalence of psychiatric disorders in patients taking vigabatrin has been previously evaluated. 14 True psychosis was noted in less than 5% of a sample of 1942 persons. The number was significant compared to those who had been given placebo during clinical trials (P = 0.028), though 40% of those subjects presenting with symptoms of psychosis had a clinical history consistent with that diagnosis. Theories as to why the incidence of psychotic symptoms is higher in persons using vigabatrin include the abrupt cessation of seizure activity (forced normalization), and excess neuronal excitatory effects experienced by vigabatrin users. 17 Due to the subjective nature of many psychiatric symptoms, and the lack of standardization for categorizing and reporting such symptoms, the actual incidence of vigabatrin-associated psychiatric side-effects is difficult to establish.
Of all the reported adverse events linked to vigabatrin use, none have received as much attention as have vigabatrin-induced visual field defects (VFD). The discovery of these visual abnormalities led to a significant delay in the approval of the drug for use in the United States. 18 The majority of patients experiencing VFD have no symptoms, which may explain why there was a time gap between the drug's approval overseas and the discovery of the problem. In addition, compensatory eye movements and head turning may go undetected for a time.
Currently, the underlying pathology of VFD is under investigation. The retinal ganglia are noted to undergo gradual changes ultimately leading to bilateral concentric constriction of the peripheral visual field. 19 The central visual field is unaffected. Though there has been some debate, vigabatrin-induced VFD are generally believed to be irreversible.
Estimates of VFD prevalence from efficacy trials range from one-in-four to half of all adults exposed to the drug for extended treatment. 20 Though some patients have had changes detected during their first year of use, most have been on the drug for several years before VFD are identified. For this reason, trial therapy with vigabatrin is felt to be safe when limited to a 12 week timeframe to determine efficacy. Those patients who are placed on vigabatrin as adjunctive therapy are carefully monitored through the utilization of a risk evaluation and mitigation strategy (REMS) that includes baseline vision testing and re-testing at three-month intervals during therapy. The patient must consent in writing when therapy is initiated, and again if the decision to continue therapy beyond the trial period is made after a demonstration of effectiveness.
Another concern with vigabatrin has been the fact that a small number of abnormal MRI findings suggestive of cytotoxic edema in patients exposed to the medication have been previously reported, (though all patients were receiving treatment for infantile spasms as opposed to CP seizures).21–23 No changes in MRI believed to be related to study drug were reported in the CP seizure studies previously summarized when such evaluations were part of the protocol.9,11,12 However, ruling out vigabatrin as a cause of unexpected MRI changes remains prudent.
Effect on other Anti-seizure Medications
Anti-seizure agents can be difficult to manage, especially when given in combination with other drugs from the class due to drug interactions and subsequent alterations in serum levels. Vigabatrin itself is not monitored using the measurement of levels and none of the investigators reported a correlation between vigabatrin levels and ultimate seizure control.
Many of the older agents are potent enzyme inhibitors or inducers, and the addition or subtraction of a drug can wreak havoc on drug levels and seizure control. Several investigators evaluated concomitant anticonvulsant plasma levels during the treatment phases of their respective trials. In the cases for which alterations in levels were statistically evaluated, it was common to see a significant drop in phenytoin concentrations.3,9,11,12 Other investigators also reported decreases in phenytoin levels of 2.7–6.6 mg/L.5,6 Additional significant changes in antiepileptic drug concentrations reported in the CP seizure trials include a decrease in phenobarbital9,11 and valproic acid, 9 however only phenytoin was consistently affected. Still, evaluations from other trials revealed no change in any concomitant anti-epileptic medication, including phenytoin.5,7 More importantly, regardless of the presence of a significant change in anti-epileptic serum levels, a correlation with loss of seizure control was never demonstrated. Because of the resistant nature of the seizures in question, and because the contribution of concomitant drugs to an individual subject's seizure control was never investigated, it is not possible to determine if the lack of change in seizure frequency associated with decreasing levels was due to the minimal roles those drugs may have played in terms of efficacy.
Conclusion
Efficacy of vigabatrin at the maximum recommended dose of 3 g/day appears well-established, save the single study by McKee and colleagues. Though tolerance has been reported in some patients after several years,24,25 it is unlikely that a total of 12 weeks of exposure with a drug-free period of four weeks at midpoint allowed for the development of therapeutic resistance in that study.
Vigabatrin, through multiple studies and over a significant timeframe, has proven to be a viable alternative therapy for adults with resistant CP seizures. Because of its side-effect profile, particularly as it relates to VFD, it remains a drug firmly ensconced in its place as adjunctive therapy.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.