
Abstract
Migraine is a neurovascular disease, which pathogenesis is still unclear. It causes a severe headache and a substantial financial loss due to absenteeism, therefore, its effective treatment is particularly valuable. Triptans, selective 5HT1B and D receptor agonists, are effective treatment choices of acute migraine attacks. Migraine patients, who bear special conditions such as hypertension, hepatic or renal impairment, constitute a special subgroup of patients whose treatment with triptans has to be individually arranged. The review of Kalanuria and Peterlin, regarding the metabolism and efficacy of zolmitriptan in the abortive treatment of migraine, highlights many details of the use of zolmitriptan in migraine patients.
Keywords
Migraine, one of the most encountered primary headaches, has an one-year prevalence of 5%-5.7% in men and 12%-17.7% in women.1–4 Its lifetime incidence has been reported to be as high as 43% in women and 18% in men. 5 A lower prevalence (8.6%) has been reported in the childhood period; however, a higher percentage is actually possible due to misdiagnosis because of patterns of childhood migraine that are distinct from the adult type as well as the probably inadequate explanation of migraine symptoms by children. 6 Migraine is most frequent in the third decade and mostly affects the working individuals of the population. Financial loss resulting from absenteeism due to migraine headaches is estimated to be approximately $13.3 billion in the USA and this financial load is much more substantial than the cost of the treatment. 7
The etiopathogenesis of migraine has not yet been clearly delineated. Despite the well-known familial predisposition, the genetic basis of migraine has not been identified except for the hemiplegic migraine variant. However, some environmental factors such as stress, bright light, odors, etc., can trigger migraine headache in individuals who are genetically prone to migraine. The ophthalmic branch of the trigeminal nerve innervates the proximal segments of the cerebral arteries and the vasculature in pia, arachnoid and duramater, which are sensitive to pain perception. Locus cereleus and Raphe nucleus are generally regarded as pain regulating centers in the brainstem. The activation of the locus cereleus and Raphe nucleus by an unknown mechanism probably activates the trigeminovascular system, causing the release of neurotransmitters such as CGRP and substance P, the vasodilation, the increase in cerebral blood flow and the protein extravasation, and ultimately resulting in sterile neurogenic inflammation and pain. The 5HT-1BD receptors are located centrally within the trigeminocervical complex in the brainstem and upper spinal cord and peripherally on the trigeminal axonal endings.8,9 The ergot alkaloids and triptans, which are effective treatment options of migraine headache, activate the 5HT-1BD receptors resulting in the inhibition of the trigeminal activation and, indirectly, the neuropeptide release and neurogenic inflammation. 10
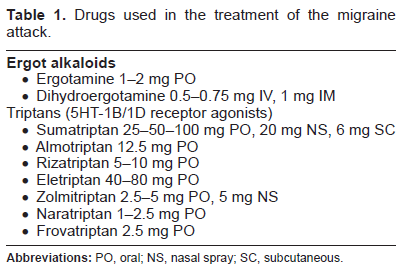
The aim in migraine treatment is to decrease the severity, duration, and frequency of the headache, to minimize the losses due to migraine, and to increase the life quality of the patient. The treatment is composed of two steps; namely, the cessation of the acute migraine headache and the prophylaxis. The prophylactic treatment aims to decrease the frequency of migraine attacks. Non-selective drugs (paracetamol, metamizole and NSAI drugs) and selective drugs (ergot alkaloids and triptans) are used in the acute attack treatment (Table 1). A new oral antagonist of CGRP receptor has recently been reported to be as effective as triptans, but to have fewer associated adverse effects. 11
Drugs used in the treatment of the migraine attack.
The expected properties from the migraine drugs are their rapid and sustained efficacy, prolonged wellness in the ictal phase of migraine, the gain of the functionality of the patient after an acute attack, the reduction of the need for recurrent drug use, minimal adverse effects, and cost effectiveness. Triptans seem to be one of the most effective choices of migraine treatment available in the last decade, and many studies have been carried out to ascertain the above mentioned properties. Careful reviews are needed to analyze their results. In this aspect, the detailed review of Kalanuria and Peterlin 12 , which brings numerous data of many studies about zolmitriptan together, is particularly valuable.
In daily praxis of migraine treatment, many migraine patients with concomitant systemic diseases such as hypertension, hepatic, and renal failure and in different aged populations, seek consultation in clinics. The efficacy and adverse effects of triptans vary in these distinct subgroups of patients. In the review of Kalanuria and Peterlin, the pharmacodynamics of 3 formulations of zolmitriptan (tablet, orally disintegrating tablet, nasal spray) is explained, and the nasal spray form appears as the more rapidly absorbable form. Zolmitriptan, of which 1/3 of elimination is renal and the remaining 2/3 is non-renal, can be used without dose adjustment in renal and hepatic impairment, unless patients are not on hemodialysis or do not have severe hepatic insufficiency. Similarly, it can be administered for migraine treatment in patients with controlled hypertension, without dose adjustment. In the comparison of a zolmitriptan 2.5 mg tablet with other triptans, similar efficacy was reported with sumatriptan 50 mg, rizatriptan 10 mg, or eletriptan 40 mg in the 2 hour headache response rate. The efficacies of eletriptan 80 mg and zolmitriptan 5 mg nasal form were found superior to zolmitriptan 2.5 mg. Additionally, zolmatriptan is effective in the suppression of migraine associated symptoms and disability. Although zolmitriptan is not approved by FDA for the treatment of migraine attacks in children, adolescents, or the elderly, data obtained from limited studies are presented in the review. Zolmitriptan also appears effective in menstruation-related migraine in spite of the lack of FDA approval. Regarding the long term efficacy, zolmitriptan maintains its efficacy in the treatment of multiple migraine attacks over a year's duration.
The review of Kalanuria and Peterlin, regarding the metabolism and efficacy of zolmitriptan in acute abortive treatment of migraine, highlights many details for use of zolmitriptan in migraine patients.
Disclosure
The author reports no conflicts of interest.