
Abstract
Suppression of the Renin-Angiotensin-Aldosterone system (RAAS) is an established intervention in the management of cardiovascular disease. Large, randomized controlled trials have provided a sound evidence base for the use of mineralocorticoid receptor antagonists to block the end product of the RAAS in the treatment of heart failure. However, the place for mineralocorticoid blockade in the treatment of hypertension is less well defined and lacking a strong evidence base. The main indication for the use of this strategy in hypertension is as a third line agent in the treatment of refractory hypertension. The most widely used mineralocorticoid receptor antagonist, spironolactone, is associated with dose related sexual side effects, limiting its use in clinical practice. Eplerenone, the selective mineralocorticoid receptor antagonist, is a promising cardiovascular drug licensed for the treatment of heart failure in Europe and heart failure and hypertension in the USA. It effectively blocks the mineralocorticoid receptor without the unpleasant sexual side effect profile of spironolactone. We review the use of eplerenone, a selective mineralocorticoid receptor antagonist in the treatment of hypertension; discuss its mechanism of action, safety profile as well as its current place in therapy.
Introduction
The first mineralocorticoid receptor (MR) antagonist spironolactone was patented almost 50 years ago but more recently has re-emerged as a potent tool in the armoury of cardiovascular drugs. There is accumulating evidence of the central role of aldosterone in the pathogenesis of many cardiovascular conditions 1 and an increasing understanding of the detrimental effects of aldosterone on cardiovascular tissues at a cellular and molecular level. 2 In addition, strong clinical evidence for the mortality benefit associated with mineralocorticoid blockade in heart failure patients 3 has fuelled a resurgence in interest in MR blockade. Eplerenone, a selective MR antagonist, is licensed for the treatment of patients with heart failure following myocardial infarction in Europe; in the USA it is also approved for the treatment of hypertension. We will review its use in the management of hypertension and its cardiovascular complications.
Aldosterone and Hypertension
Initially identified in 1953, 4 aldosterone is known to regulate sodium and water homeostasis via activation of apical sodium channels in the renal cortical collecting duct, allowing net movement of sodium and water from the lumen to the interstitium. Na-K ATP-ase channels in the basal membrane are also activated by aldosterone, resulting in a net loss of potassium in to the tubular lumen and thus maintaining electrical neutrality. The presence of mineralocorticoid receptors in other epithelial tissues e.g. the colon 5 and salivary glands has long been recognised. However, it is now understood that MR are present in non-epithelial cells in the vascular system, heart 6 and brain. 7 Activation of the MR in these tissues can result in a range of adverse cardiovascular effects including a rise in cardiac collagen synthesis, 8 enhanced central sympathetic outflow 7 and enhanced pressor response. 9 Thus MR activation has the capacity not only to increase blood pressure but to accelerate the complications of hypertension. In addition there is some evidence for local steroidogenesis outside the adrenal gland although the impact of this on the aetiology of hypertension and cardiovascular disease is unclear. 10 While the conventional ligand of the mineralocorticoid receptor is aldosterone, derived from the adrenal cortex, the principal glucocorticoid, cortisol, has equal affinity for the receptor. Accepted wisdom holds that cortisol (which circulates at around 100 fold higher concentrations than aldosterone) is prevented from illicitly occupying the receptor by the enzyme 11β hydroxy steroid dehydrogenase type 2 (11β HSD2) which converts cortisol to its inactive metabolite cortisone. Inactivation 11β HSD2, either by glycyrrhetinic acid contained in liquorice or in individuals with a genetic disorder, results in mineralocorticoid like hypertension, and this lends weight to this theory. However, it is not well understood how 11β HSD2 can inactivate adequate amounts of cortisol given its overwhelming excess in the tissues. It has been proposed that glucocorticoids may still occupy but not activate the MR, and activation is determined by local intracellular redox state. 11
Once the MR is activated, genomic responses that take place over some hours or days occur, mediated via increased transcription of protein and triggered by translocation of the receptor-ligand complex from the cytosol to the nucleus. For example, binding of aldosterone to the MR induces serum and glucocorticoid-regulated Kinase (sgk) expression which causes an increase in sodium channel availability in the apical surface of the distal nephron. 12 In contrast, rapid effects on the vasculature, heart and kidney occurring over seconds or minutes, and at subnanomolar concentrations, are described as non genomic actions. Some of these effects of aldosterone are mediated via the MR and this can be confirmed by the observation that blocking MR inhibits many of these actions. 13
The capacity for aldosterone excess to cause hypertension has been undisputed since Jerome Conn's first description of an aldosterone secreting adrenal adenoma in a patient with hypokalaemia and hypertension. 14 Although aldosterone secreting adenomas are a relatively rare cause of hypertension, there is evidence that relative aldosterone excess (either as a consequence of adenoma or bilateral adrenal hyperplasia) as determined by an elevated aldosterone to renin ratio, contributes to up to 10% of so called essential hypertension.15,16 In addition, data from the Framingham cohort suggests that increasing aldosterone, even within the normal range, increases future blood pressure progression 17 while a similar association between plasma aldosterone and blood pressure has recently been reported in a late middle aged cohort in the UK. 18
Aldosterone may contribute to the development of hypertension but additionally, there is evidence that aldosterone itself (or at least MR activation) can induce pathophysiological changes. Animal studies have confirmed that in the presence of a high salt diet, aldosterone excess produces vascular inflammation and stiffness, 19 myocardial ischemia and fibrosis and endothelial dysfunction. 20 In addition, renovascular damage is also observed with aldosterone infusions and reversed with the addition of MR blockade. 21 Some evidence exits that aldosterone has similar detrimental effects in human hypertension; patients with hypertension and aldosterone excess develop more cardiovascular events than matched controls with essential hypertension. 22
Eplerenone; Mechanism of Action, Metabolism and Pharmacokinetic Profile
Following on from the identification of aldosterone, the first mineralocorticoid antagonists were developed in the early 1960s. Spironolactone was only one of a number of products initially screened and although structures with more potent anti-mineralocorticoid action than spironolactone, (the most promising of which was prorenone, administered as the potassium salt in the form of prorenoate potassium), 23 were evaluated in man, none entered large-scale clinical development. Spironolactone was originally licensed for the treatment of primary aldosteronism, peripheral odema, and hypokalemia and it was shown to be an effective antihypertensive; Wolf et al 24 demonstrated a drop in blood pressure of around 10/5 mmHg with 25 mg spironolactone, rising to around 20/10 mmHg with 100 mg spironolactone. However, its widespread use has been limited by unpleasant side effects including gynecomastia, reduced libido and menstrual disturbance, predominantly due to its lack of specificity for the mineralocorticoid receptor. Because of these difficulties, it has until recently, played a minor role in clinical practice.
These problems with spironolactone led to a search for a mineralocorticoid antagonist with a greater degree of specificity. Thus, the addition of a 9, 11 epoxy group to the lactone ring structure of the basic compounds (Fig. 1) was recognized to reduce the affinity for the progesterone and dihydrotestosterone receptors 25 while maintaining an anti-mineralocorticoid effect. 26 This structure has a 500 fold less affinity for these receptors. However, it is a less potent inhibitor of the mineralocorticoid receptor (Table 1). Although in vitro studies suggest that this is around 10-20 fold less than spironolactone, in vivo, it appears to be around 50% as potent. 25 Clinical studies were undertaken with these compounds but it was 15 years later before eplerenone (epoxymexrenone) gained its license. 27
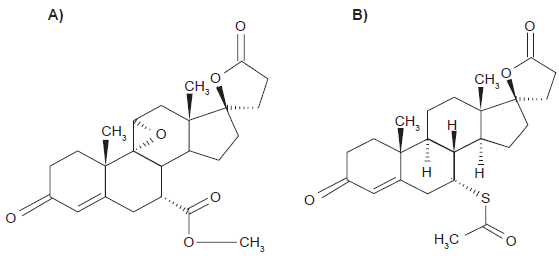
Structure of A) Eplerenone and B) Spironolactone.
Relative binding affinities for spironolactone and eplerenone.

Eplerenone is absorbed from the gastrointestinal tract with a maximum concentration of 1.3 hours and is moderately protein bound, in a concentration dependant manner. 28 There are few data to ascertain whether once daily or twice daily dosing of eplerenone is optimal; certainly its half life is shorter that spironolactone and with no active metabolites, 29 it would seem plausible that a twice daily regime would be required. One study examined the antihypertensive effect of 50 mg, 100 mg and 400 mg of eplerenone and demonstrated no greater blood pressure effect with twice daily dosing except at the 100 mg dose. At this dose the blood pressure reduction was an additional 3.4 mmHg less with a 50 mg bd regime as opposed to 100 mg daily. 30
Spironolactone use is associated with histological change in the adrenal gland in the form of spironolactone bodies 31 and there is evidence that it has the potential to reduce adrenal steroid production by inhibiting steroidogenic cytochrome P450 enzymes as well as blocking their effects at the receptor. The concentrations of spironolactone required to reduce steroid production are much higher that those needed to block the mineralocorticoid receptor and it has been proposed that this occurs via a non-genomic mechanism. In contrast, recent evidence using in vitro models suggests that these effects are not seen with eplerenone, even at doses in excess of the in vivo equivalent. 32 It may be that some of the “off target” effects associated with spironolactone's less selective mode of action are, in fact, beneficial.
Clinical Studies
Efficacy of eplerenone in hypertension
In the Randomised Aldactone in Heart failure (RALES) study 3 patients with chronic, stable heart failure, NYHA class III/IV, benefitted from a mean dose of 26 mg spironolactone with a 30% reduction in relative risk of death. Patients with mild- moderate heart failure following a myocardial infarction were examined in the Eplerenone Post Myocardial Infarction Heart Failure Efficacy and Survival study (EPHESUS); 33 a 15% risk reduction of all cause mortality was associated with eplerenone use (mean dose 43 mg). Thus, MR blockade would appear to be a useful therapeutic strategy for reducing mortality in the context of chronic, severe heart failure (spironolactone) or mild-moderate heart failure post MI (eplerenone) based on robust and consistent results from these large clinical studies with hard clinical end points. In contrast however, treatment of hypertension with mineralocorticoid blockade is not based on such conclusive evidence.
It might be anticipated that the development of eplerenone would offer the potential for anti-mineralocorticoid actions, effective blood pressure control and a reduction in adverse effects. Initial early studies demonstrated that eplerenone could be used as monotherapy to control mild hypertension (mean baseline BP 149/96 mmHg) in patients with essential hypertension. 34 However, in terms of efficacy of antihypertensive action, eplerenone has been demonstrated to have equivalency but not superiority of antihypertensive effect as compared with monotherapy using a calcium channel blocker, 35 an ACE inhibitor 36 or an angiotensin-II-receptor blocker.37,38 It has been suggested that eplerenone has greater efficacy than ACE inhibition in hypertensive patients with low renin levels,37,39 a phenotype more common in black 38 and Asian hypertensive patients. 39 However, this has not been a consistent finding. 40
The role of MR blockade in resistant hypertension has a greater weight of evidence behind it; the ASCOT study recently provided evidence of the clinical utility of MR blockade in resistant hypertension, demonstrating mean blood pressure reduction of 21.9/9.5 mmHg (95% CI: 20.8 to 23.0/9.0 to 10.1 mmHg; P < 0.001) with the addition of 25 mg spironolactone as a fourth line agent for the control of blood pressure. 41 Similarly the addition of eplerenone to an ACE inhibitor or an angiotensin II antagonist has been shown to provide added antihypertensive benefit in patients who were not controlled on monotherapy. 42
There is limited evidence to suggest that the dose required for eplerenone is higher that that necessary for the same blood pressure reduction with spironolactone. The only published study that directly compares eplerenone to spironolactone was designed to demonstrate safety and efficacy of eplerenone as an antihypertensive, with spironolactone being used as a mineralocorticoid antagonist positive control. Although formal comparison of both MR antagonists was not performed, spironolactone 50 mg b.d. achieved greater blood pressure reduction than equivalent doses of eplerenone. These data demonstrated that eplerenone has approximately 75% of the blood pressure reduction seen in spironolactone. 30
Additional cardiovascular protection?
Clearly one of the key questions with MR blockade in hypertension is whether it provides additional cardiovascular protection, over and above blood pressure control. Experimental data with animal models demonstrating the deleterious effects of aldosterone, and its reversal with blockade of the MR raised hopes that similar benefits would be observed in clinical studies. Thus, the 4E trial 43 provided some clinical data to support the hypothesis that suppression of the RAAS using eplerenone offered an effective method of reducing end organ damage independent of blood pressure reduction. This study was a 9 month randomized double blind trial of enalapril or eplerenone or a combination of both in patients with hypertension and left ventricular hypertrophy (LVH). MRI was used to assess LVH and 202 patients were enrolled in the study.
Attempts were made to normalize blood pressure with the addition of hydrochlorothiazide or amlodipine. Blood pressure equivalence in each arm was achieved with respect to diastolic blood pressure but not systolic. Patients receiving combination therapy had a small but significant reduction in systolic blood pressure compared to eplerenone or enalapril alone. While LV mass was decreased in the group receiving combination therapy to a greater extent than with eplerenone alone. The smallest difference in left ventricular mass was seen in the enalapril group, although comparison between this and eplerenone alone did not reach statistical significance. Analysis of the data when those requiring add on therapy were removed however, suggested no difference between enalapril and eplerenone in reducing LV mass where blood pressure reduction was equivalent. It appears therefore that eplerenone is as effective as enalapril in reducing the target organ damage associated with hypertension and suggests that more complete suppression of the RAAS with two agents provides more effective protection. It does not, however, suggest that eplerenone has a uniquely beneficial effect on cardiac function. Nevertheless, it must be noted that this was a relatively short term study, and it is possible that longer term therapy might be required to demonstrate specific benefit in from mineralocorticoid receptor blockade.
Measurements of renal microalbumin excretion were made in the 4E study and it was observed that treatment with eplerenone significantly decreased 24-hour urine albumin createnine ratio, as did enalapril but the combination and eplerenone/enalapril had greater benefit. As mentioned above, blood pressure was not equivalent in all arms of this study. However, microalbininuria production and renal protection was further explored by Epstein et al, 44 who demonstrated the superior anti-albuminuric effects of dual therapy with eplerenone and ACE inhibition as compared to ACE inhibition alone in patients with diabetic nephropathy. In contrast with the 4E study, similar blood pressure reductions were obtained in each arm of this study. White et al also provide evidence for the renoprotective effect of eplerenone. They found it reduced the urinary albumin/creatinine ratio by 52% compared with a reduction of 10% by amlodipine (P = 0.04) with equal blood pressure reduction. It could be argued that the choice of amlodipine as a comparator antihypertensive makes it inevitable that a positive result is achieved for reduction in albuminuria with eplerenone. 45 Nevertheless, there is an increasing body of evidence that MR blockade has beneficial effects at the kidney, 46 albeit with a higher risk of side effects (see below).
It has been proposed that MR blockade can improve resistance artery remodeling in hypertensive patients to a greater extent that beta blockade, at similar levels of blood pressure control. A small study in 16 hypertensive patients demonstrated a reduction in small artery stiffness after one year of treatment with eplerenone compared to beta blockade where an increase in stiffness was observed. 47
In summary, it is difficult at present to draw any firm conclusions regarding the benefit of MR blockade in general and the use of eplerenone in particular in the treatment of hypertension. A number of small studies raise the possibility of additive cardiovascular benefit, over and above blood pressure control; however, all use surrogate endpoints, study small numbers of patients and most for a short period of follow-up. No study provides evidence of improved morbidity or mortality and, in contrast to the well recognised therapeutic strategy in heart failure, to date, studies in hypertensive subjects do not provide clear evidence for the use of MR antagonists routinely.
Safety of Eplerenone
Sexual side effects
The first mineralocorticoid receptor antagonist, spironolactone, was limited in its use as an antihypertensive due to the significant risk of sexual side effects. In one large series, 13% of male patients treated with spironolactone reported gynecomastia 48 and rates were similar among participants in the RALES study, 3 although slightly lower (around 6%) when spironolactone was added as a fourth line agent in the ASCOT study. 41 There is a dose response relationship with these side effects and spironolactone, and the risk of gynecomastia rises significantly with doses above 100 mg per day. 28
These unpleasant side effects are due to spironolactone's lacks of specificity for the mineralocorticoid receptor. However in comparison, eplerenone has a markedly reduced affinity for the progesterone and androgen receptors (Table 1). This results in a significantly reduced incidence of sexual side effects.25,49 In clinical trials investigating heart failure, the incidence of gynecomastia resulting from eplerenone use has been small. EPHESUS found only 12 men with gynecomastia randomized to eplerenone rather that the 14 in the placebo group. In addition, there was no increase in the incidence of impotence in participants on eplerenone, nor was there increase in breast pain or menstrual disorders in women. As with spironolactone, the dose of eplerenone may be important in the development of side effects. In EPHESUS, the mean dose was 46 mg per day but at higher doses; sexual side effects may be more common. A number of small clinical trials using higher doses of eplerenone for the treatment of hypertension have observed a non statistically significant increase in gynecomastia. Although clearly the rates of side effects with eplerenone remain lower that the rates associated with spironolactone, larger clinical trials, of a longer duration, with higher doses of eplerenone would be required to observe and quantify these effects.
Hyperkalemia
Mineralocorticoid blockade is associated with a risk of hyperkalemia and this has been well described with spironolactone. 48 Similarly, potassium is seen to rise in individuals treated with eplerenone in a dose related manner. 50 What is not clear is whether eplerenone has less capacity to provoke hyperkalemia than spironolactone. It has been proposed that due to its shorted half life and lack of active metabolites, 28 this may indeed be the case. However, data from hypertension studies using eplerenone are inconsistent. One study comparing 50 mg spironolactone with various doses of eplerenone (50-400 mg), 30 found the mean potassium rise associated with spironolactone 50 mg was greater that that associated with eplerenone 50 mg and in fact was equivalent to eplerenone 400 mg.
In the controlled environment of clinical trials, the risk of significant hyperkalemia associated with MR blockade in hypertension is low. The ASCOT trial used spironolactone 25 mg as a fourth line agent in blood pressure control and in this study, serum potassium increased by mean 0.41 meq/l (95% CI: 0.37 to 0.44 meq/l). 41 Serum potassium levels were found to be >5.5 meq/l in 4% of participants on spironolactone, and 2% had levels >6.0 meq/l. The percentage with hyperkalemia was identical among participants randomly assigned to the atenolol-based and amlodipine-based regimens. In the majority of clinical investigations for eplerenone in the treatment of hypertension, the rates of hyperkalemia are between 1 and 3% and were not statistically different from placebo or comparator antihypertensive. However, subjects with significant renal impairment were excluded and this is likely to account for the low incidence of hyperkalemia.
It is interesting to note that in the investigations by Epstein et al 44 examining the effect of eplerenone on diabetic nephropathy, similarly low rates of hyperkalemia were observed (6.2% in eplerenone treated individuals vs. 3.4% placebo). Indeed, these patients appeared to achieve greater benefit with a reduction in microalbuminuria associated with eplerenone, independent of blood pressure reduction. It should be highlighted that despite their microalbuminuria, the patients included in this study nevertheless had eGFR > 70.
The 4E study 43 had a slightly higher reported rate of hyperkalemia with 7 (11%) patients on eplerenone and 3 (4.5%) on combined eplerenone/enalapril reaching potassium levels of >5.5 meq/l. This compares to 2 (2.8%) on placebo alone. The reason for this higher rate is not clear; patients with creatinine greater than 1.5 mg/dl (around 150 meq/l) were excluded from this study. Participants did have LVH at baseline and it is possible that their more developed cardio-renal phenotype made them more susceptible to the adverse effects of MR blockade.
Hyperkalemia has been described more commonly in MR antagonist therapy associated with heart failure trials. In the EPHESUS 33 study, 5.5 percent of patients in the eplerenone group, as compared with 3.9 percent of those in the placebo group (P = 0.002) experienced serious hyperkalemia (K > 6 meq/l). The risk of hyperkalemia rose with declining renal function; patients with an initial creatinine clearance of less than 50 ml per minute had an incidence of serious hyperkalemia of 10.1 percent in the eplerenone group and in contrast this was 5.9 percent in the placebo group (P = 0.006).
Nevertheless, the risk of hyperkalemia out with the clinical trial setting is certainly higher that the above quoted values. This was reflected in the rise in rates of admissions with hyperkalemia in heart failure patients following the publication of the RALES trial. 51 The majority of adverse incidents occur in patients who would not have met the criteria for entry to the initial trial. Careful consideration should be given before commencing individuals on eplerenone where baseline serum potassium is greater than 5.0 meq/l or an estimated glomerular filtration rate is less than 30 ml/min. In addition, it is known that in elderly patients (>65 years) the maximum plasma concentration achieved by administration of 100 mg of eplerenone is 22% greater than subjects aged 14-45 years. 28 This is not sufficient to warrant a dose adjustment but, should be borne in mind in terms of indicating a greater propensity for toxicity and side effects in these individuals.
Other safety considerations
It has been noted that at higher doses eplerenone is associated with a small increase in thyroid stimulating hormone. This is not likely to be clinically significant as it has only been observed at higher than recommended doses (up to 400 mg daily) and has been asymptomatic. In addition, monitoring this possible adverse effect would not be problematic and the biochemical phenomenon appears to be reversible. 30
It should be remembered that eplerenone is eliminated via the cytochrome P450 3A4 system and as such should not be co administered with agents that inhibit these enzymes. For example, ketoconazole (and itraconazole), increases the area under the curve (AUC) of eplerenone 5-fold when they are coadministered. 28 Other less potent inhibitors of the cytochrome P450 3A4 system (e.g. Clarithromycin, erythromycin, verapamil, diltiazem, fluconazole and others), have the potential to increase the AUC for eplerenone to a lesser extent and may theoretically, increase the risk of hyperkalemia.
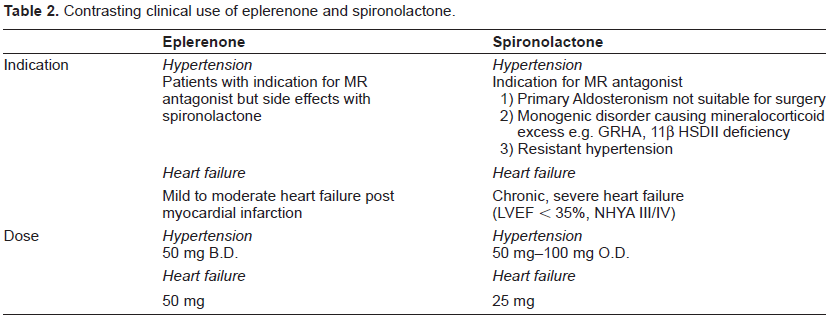
Contrasting clinical use of eplerenone and spironolactone.
Patient Preference
There are no formal studies examining patient preference for either spironolactone or eplerenone. Clearly, the lower rates of gynecomastia, menstrual irregularities, breast pain and sexual dysfunction would make eplerenone more attractive and are a maj or reason for non compliance with spironolactone. However, Eplerenone remains expensive apart from in Japan, and this may also have an impact on patient choice. In addition, a once daily regime for spironolactone may also be more palatable for patients than a twice daily regime for eplerenone. Certainly, guidelines such as the European Society Guidelines for the Management of Arterial Hypertension 52 would suggest that a once daily regime should be preferred. It should also be born in mind that eplerenone remains unlicensed for the treatment of hypertension in Europe.
Place in Therapy
The place of MR antagonists in the treatment of heart failure is clear and based on sound clinical evidence. There are sufficient data to suggest that chronic heart failure patients who meet the criteria for spironolactone, and heart failure patients following myocardial infarction, meeting the criteria for eplerenone, would benefit from the addition of these drugs. However, in the treatment of hypertension there are less clear conclusions to be drawn. Indeed, to date, there are no controlled clinical trials evaluating the safety and efficacy of eplerenone in hypertensive subjects and therefore, decisions regarding its place in therapy must be made in the absence of sound evidence.
Individuals with aldosterone excess as a result of an autonomous adenoma not suitable for surgery or patients with bilateral adrenal hyperplasia are likely to benefit from the action of an MR antagonist. A small number of individuals with rare genetic defects of aldosterone and MR regulation (11 beta HSD2 deficiency, Glucocorticoid remedial hyperaldosteronism) will also clearly benefit from blockade of the receptor. In addition, there is good evidence that the addition of spironolactone will produce better blood pressure control for the treatment of resistant hypertension. In those individuals where the development of sexual side effects results in an inability to tolerate spironolactone, altering the regime to eplerenone is reasonable although it should be borne in mind that the dose required is likely to be higher and twice daily dosing may be necessary. While there is a large body of preclinical data to suggest that eplerenone and spironolactone may confer end organ protection over and above blood pressure control, clinical evidence to support the use of MR blockade in routine treatment of hypertension remains lacking. In addition, there is a large amount of uncertainty regarding the differences in action of spironolactone and eplerenone and further comparisons both at preclinical and clinical trial level are required.
Conclusions
The use of mineralocorticoid receptor blockers is an exciting advance in cardiovascular medicine and is no less so because the therapies have been available for a number of years. MR antagonism in pre clinical animal studies demonstrate impressive benefit to a range of end organs, and the evidence from heart failure cohorts provides some support to the idea that this translates to clinical practice. However, eplerenone remains unlicensed for the treatment of hypertension in Europe and there are no convincing data to support its use as a first line antihypertensive. Further data are required to demonstrate the utility of MR blockade in general and selective MR blockade in particular in a hypertensive cohort. In the meantime, the main indication for the use of MR blockade in hypertensive subjects is in the management of refractory hypertension, and in these circumstances, eplerenone may be useful in those individuals who develop sexual side effects.
Disclosure
The authors report no conflicts of interest.