
Abstract
Deep vein thrombosis (DVT) is a frequent and potentially life-threatening condition, and acute and late complications are common. The diagnostic approach to DVT needs to be reliable, widely available, and cost-effective. Furthermore, several therapeutic options are available for DVT treatment and the choice of anticoagulant drug, dosage, and treatment duration has to reflect the specific situation of the individual DVT patient. This review was aimed to provide bedside guidance for clinicians faced with common (and less common) clinical scenarios in DVT treatment.
Introduction
Acute or subacute deep vein thrombosis (DVT) usually, but not exclusively, occurs in the legs with an estimated incidence of 1:1000/year.1–4 The most dangerous complication of DVT is pulmonary embolism (PE), which can either be asymptomatic (~30% of DVT patients have silent PE at the time of DVT diagnosis 5 ) or symptomatic (tachycardia, dyspnea, or hypoxemia, which are usually caused by increased right ventricular pressure and/or reduced pulmonary perfusion). DVT and PE are two manifestations of venous thromboembolism (VTE), which may be caused by provoking factors such as major surgery, trauma, immobilization, or hormonal contraceptives, may be associated with cancer or cancer therapy, may be caused by thrombophilia, or may occur spontaneously without any of these factors present. 6 Insufficient diagnostic or therapeutic workup for DVT or PE treatment accounts for a considerable number of fatal complications. 7 In addition to the acute mortality, patients surviving with PE are at a considerable risk of developing chronic thromboembolic pulmonary hypertension, which impacts quality of life, treatment costs, and long-term prognosis. Finally, patients with DVT may develop postthrombotic syndrome (PTS), which constitutes symptoms and organic changes of the leg veins and tissues caused by increased venous pressure, residual vein occlusion, or venous valve damage following the acute thrombotic event.
This review focused on the current standard of DVT diagnosis and therapy, which, to our understanding, is the best approach to prevent potentially fatal complications, such as severe PE, and to prevent long-term health consequences.
Current Standards for Diagnosing DVT – from Symptoms to Diagnostic Reliability
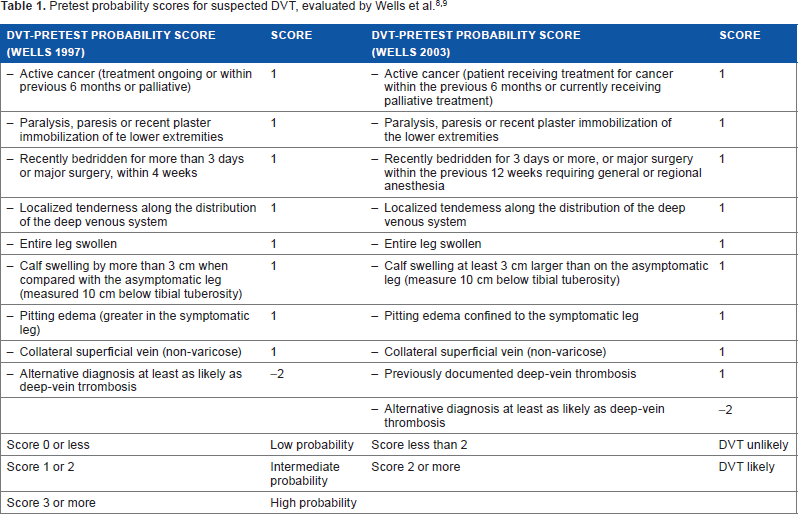
Pain, swelling, and discoloration due to venous stasis are the most common symptoms of DVT patients. However, several other conditions such as infections, hematoma, joint and/or muscle injuries, and chronic joint conditions may present in the same way. As a consequence, clinical examination alone is insufficient to safely establish or rule out DVT. However, if findings from clinical examination are combined with the assessment of DVT triggers in recent history (such as trauma, surgery, immobilization, long-distance travel, cancer, hormone treatment, and pregnancy), preferably with a standardized scoring system such as the Wells score (Table 1),8,9 a much more accurate assessment of DVT probability is possible. The use of the Wells score still does not reliably diagnose or rule out DVT, but it defines the correct diagnostic procedure for patients with different probabilities of having DVT. Patients with a simplified Wells score (2003 version) of ≤2 points have a low probability of having DVT, and in ultrasound examination, only 5% of patients were found to have the disease. 9 If the Wells score is ≤2, ultrasound is needed only in patients who also have elevated d-dimers, a fibrin degradation product that forms during endogenous thrombolysis. Taken together, DVT can be reliably ruled out in all patients who have a low Wells score and negative d-dimers, and ultrasound would be an unnecessary step in the diagnostic workup (Fig. 1).9,10
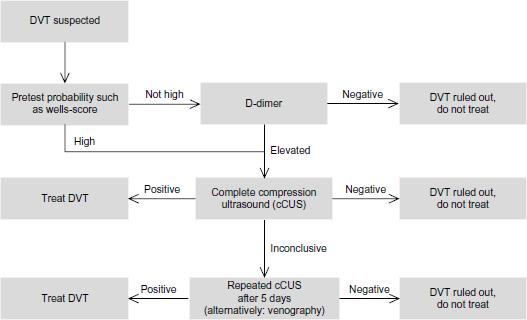
Diagnostic workup of DVT.
In contrast, all other patients (namely, those with a Wells score of >2 and those with low Wells score but abnormal d-dimer) must be sent for objective testing, which comprises venous compression ultrasound. This stepwise diagnostic workup is recognized by most current VTE guidelines (Fig. 1).10,11
Important notes for Wells score and d-dimer testing are the following:
Wells score and other DVT probability scores are only useful in outpatients with suspected DVT. Hospitalized patients with DVT symptoms are by definition at high probability to have DVT, and objective testing (usually with ultrasound) is always indicated. Consequently, d-dimer testing is not useful to guide diagnostic decisions in hospitalized patients.
All currently available laboratory-based d-dimer tests have high sensitivity. In contrast, so-called bedside or point-of-care (POC) d-dimer tests vary considerably with regard to sensitivity.12–14 Users of POC are advised to obtain sensitivity data from the manufacturer or from the published literature to interpret the POC results correctly. For all quantitative or semiquantitative d-dimer tests, a cutoff has been defined. It was recently established that the cutoff of “normal” d-dimers is higher in elderly patients, and age-adjustments are now recommended to avoid too many false-positive d-dimer results in elderly patients, 15 which would result in a high number of unnecessary ultrasound examinations.
All d-dimer tests lack specificity. d-Dimer values are often increased in acute infections, cancer, or pregnancy, and from a positive d-dimer test alone, the presence of DVT cannot be concluded. 16 Consequently, the practical value of d-dimer testing derives from the negative predictive value (or high sensitivity). Patients with low Wells score and negative d-dimers do not have DVT.
Negative d-dimer as a stand-alone test is insufficient to rule out DVT, since, without the preselection of patients with low Wells score, the sensitivity of dimers decreases considerably.
Important notes for ultrasound are as follows:
Venous compression ultrasound using B mode and pelvic vein doppler can be safely regarded as the gold standard of DVT imaging, and the additional use of color mode or distal doppler mode is not routinely needed. The concept is simple: if a venous segment is not compressible, something inside has to prevent compressibility and venous thrombosis can be diagnosed.
For compression ultrasound, a single examination of the whole leg vein system (complete compression ultrasound [CCUS] including all below-the-knee or distal veins) has been shown to be accurate and safe both in patients with and without DVT,17,18 but this protocol requires ultrasound experience.
A limited compression ultrasound (LCUS) with examination of the groin and popliteal fossa is rapid and easy to learn. This simple protocol is able to detect ascending clots that involve these regions. As a consequence, LCUS seems ideal for emergency situations (emergency room and intensive care unit), where a rapid assessment is needed and dedicated venous ultrasound experience may be limited. If no DVT is found in the groin and popliteal fossa, the examination should either be continued toward a single complete compression ultrasound or the patient should be reexamined within the next five days. The concept behind this is the fact that an ascending DVT becomes visible in the groin or popliteal fossa, if progression toward these segments is allowed. Physicians may be concerned about leaving patients with suspected DVT untreated for five days, which is why the authors prefer CCUS, but this repeated LCUS strategy with examination of the groin and popliteal fossa only has been shown to be feasible and safe. 19
The authors are well aware that ultrasound examination may not be possible in all patients or may not result in a definite diagnosis. In such cases, repeat ultrasound after five days or venography (rarely used in today's clinical practice) would be the options. We are also aware that CT and MRI protocols exist to visualize leg veins and leg DVT, but we regard such examinations as mainly of scientific value and little clinical usefulness because of the limitations of contrast media side effects, relevant radiation exposure with CT, lack of 24/7 availability, and costs. However, patients with iliac or cava vein thrombosis are usually diagnosed by CT scan, since ultrasound is of limited value in these situations.18,20
Patients with suspected or confirmed DVT and chest symptoms, such as pain, dry cough episodes, pleuritic, pneumonia refractory to antibiotics, dyspnea, tachycardia, or syncopes, need to be evaluated for the presence of PE. This is not within the focus of this review, but ECG, Echo, and lung CT angiography are the appropriate routine examinations for such patients. 21
Anticoagulation in DVT treatment
Today, the necessity of immediate and adequately dosed anticoagulation for acute DVT is undisputed, since anticoagulation has been shown to effectively reduce thrombus progression, mortality, and the risk of severe PTS.22–24
In contrast to anticoagulation, the role of thrombolysis25,26 and the relevance of compression therapy in acute and chronic DVT are still matters of debate.27–30
Before the different anticoagulation options are discussed, it is essential to understand the four different treatment phases that need to be discussed for every DVT (or PE) patient.
Pretherapy: This treatment phase starts with the suspicion of DVT, in many cases hours or days before the diagnosis is established, until the diagnosis is made or ruled out.
Initial therapy: This treatment phase starts with the established diagnosis and lasts for ~5–10 days post diagnosis.
Maintenance therapy (or early secondary prevention): This treatment phase follows the initial therapy and lasts for three months.
Extended secondary prevention: This treatment phase starts three months after DVT diagnosis and is highly variable across the DVT population.
For a number of reasons, the differentiation of these four phases is important.
The risk of major and potentially fatal complications from DVT changes over time and is the highest in the first one to four weeks after diagnosis.
Different treatment options exist for each treatment phase, and the correct choice of drug and dosing regimen depends on the knowledge of these treatment phases.
The long-term risk of recurrent VTE is the main factor for deciding for or against long-term or indefinite anticoagulant treatment. The understanding of the concept of treatment phases is essential for the correct timing of this decision, for thrombophilia testing, and for the choice of drug and dosage, if long-term treatment is warranted.
The risk of bleeding needs to be included in all treatment decisions. However, bleeding risk needs to be assessed at regular intervals, which need to be defined.
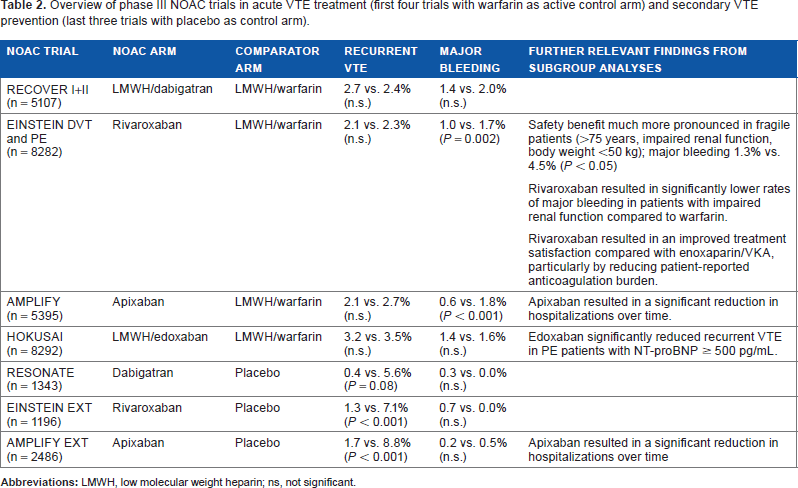
For acute DVT treatment, a number of options exist for each respective treatment phase. Together with unfractionated heparin (UFH), low-molecular weight heparin (LMWH), fondaparinux and vitamin K antagonists (VKA) we discuss all approved non-vitamin K oral anticoagulants (NOACs), which will be addressed in alphabetical order, which does not indicate a grading. Of note, although NOACs are commonly discussed as a specific class of direct anticoagulant drugs, they demonstrate relevant differences in their pharmacological profile. Dabigatran is a direct thrombin inhibitor with a high degree of renal elimination, whereas apixaban, edoxaban, and rivaroxaban are direct factor Xa inhibitors with considerably lower renal clearance. For a more detailed information, the reader should refer to a dedicated NOAC review. 31 Table 2 provides an overview of phase III NOAC VTE treatment programs. These trials mainly differed with regard to the management of NOAC patients in the pretherapy and initial therapy phases; as a result, there are now different recommendations for each NOAC in these treatment phases.
Overview of phase III NOAC trials in acute VTE treatment (first four trials with warfarin as active control arm) and secondary VTE prevention (last three trials with placebo as control arm).
Pretherapy
The risk of developing potentially fatal DVT complications such as severe PE is highest at the very beginning of the disease and treatment. While ultrasound should be performed as soon as possible, it may not be available within the first few hours. As a consequence, guidelines recommend to start anticoagulant therapy even before the diagnosis of DVT is established. 32 However, not all the available anticoagulants can be used in this situation.
UFH, LMWH, 32 fondaparinux, and two of the NOACs, namely, apixaban 33 and rivaroxaban, 34 can be used, since they are specifically approved for the initial treatment phase. All these drugs demonstrate an immediate onset of action and offer sufficient protection within two to four hours after initiation. Fondaparinux is a parenteral indirect factor Xa inhibitor, which is handled similar to LMWH. However, it is a pentasaccharide, not a protein like heparin, and, therefore, demonstrates a lower risk of heparin-induced thrombocytopenia or skin allergies, which makes it an option for patients with heparin allergies. In contrast, UFH should only be used as a first-line option for patients with severe renal impairment or those in need of thrombolytic therapy.
VKA are not suitable for initial treatment, since they exhibit a slow onset of action (days) and increase the risk of thromboembolic complication in the first few days because of their inhibition of endogenous proteins C and S.
The other two NOACs, dabigatran 35 and edoxaban, 36 also have a rapid onset of action but they are only approved for being started after an initial LMWH therapy of at least five days. Consequently, they should not be used for pretreatment.
Since ultrasound is usually performed within 24 to 48 hours of DVT suspicion, most patients in daily care receive one or two injections of a parenteral drug or rivaroxaban or apixaban at a therapeutic dosage in the pretreatment phase.
Initial therapy
As soon as the diagnosis of DVT is established, therapeutic anticoagulation is even more important. The risk of DVT complication is high for the first four weeks and highest in the first week after diagnosis. 37 Consequently, the initial therapy phase is characterized by intensified anticoagulation. The choice of drugs follows the same considerations as for pretreatment but also includes the consideration of the planned therapy for the maintenance phase, since the choice of drug and regimen in the initial phase is routinely driven by the treatment plan for the next three months:
If the maintenance phase is planned with apixaban of 5 mg BID, treatment in the initial phase should consist of apixaban of 10 mg BID for the first seven days.
If the maintenance phase is planned with rivaroxaban of 20 mg BID, treatment in the initial phase should consist of rivaroxaban of 15 mg BID for the first 21 days.
In these two scenarios, a pretreatment with LMWH or fondaparinux is not necessary but, if given, would not be problematic. Parenteral therapy can simply be stopped, and the oral drug can be started at the time the next injection would be due. The difference between apixaban (intensified treatment of seven days) and rivaroxaban (21 days) reflects the regimen used in the respective phase III trials, which were successful for both treatments.38–40 However, it is important to know that initial regimens are quite different for different anticoagulants.
If the maintenance phase is planned with dabigatran of 150 mg BID or edoxaban of 60 or 30 mg OD, treatment in the initial therapy should also be done with LMWH for at least five days, and the oral drug should only be started afterward at a time when the next LMWH injection would be due.
If the maintenance phase is planned with LMWH (in cases of cancer-associated DVT), then initial therapy will also be done with LMWH approved for cancer-associated DVT.
If the maintenance phase is planned with VKA, treatment in the initial therapy needs to be done with a parenteral anticoagulant, usually LMWH or fondaparinux, and VKA started in parallel because of the slow onset of action. As soon as VKA is sufficiently protective (international normalized ratio [INR] > 2), the parenteral drug can be stopped.
Maintenance treatment
As stated earlier, the initial phase lasts for approximately one week, although rivaroxaban should be given in an intensified dosage until day 21. Initial treatment is followed by a phase of secondary VTE prevention. All the aforementioned treatment options are approved for this phase, which ends approximately three months after DVT diagnosis. Treatment options for this phase are as follows:
Apixaban of 5 mg BID, dabigatran of 150 mg BID, edoxaban of 60 mg OD, and rivaroxaban of 20 mg OD;
LMWH or fondaparinux; and
VKA (target INR 2–3), requiring INR measurement and dose adjustment at regular intervals (at least monthly). Furthermore, frequent interactions with many drugs and food limit the use of VKA, given the availability of more convenient NOACs.
Figure 2 is a flowchart of treatment considerations in patients with suspected or confirmed DVT.
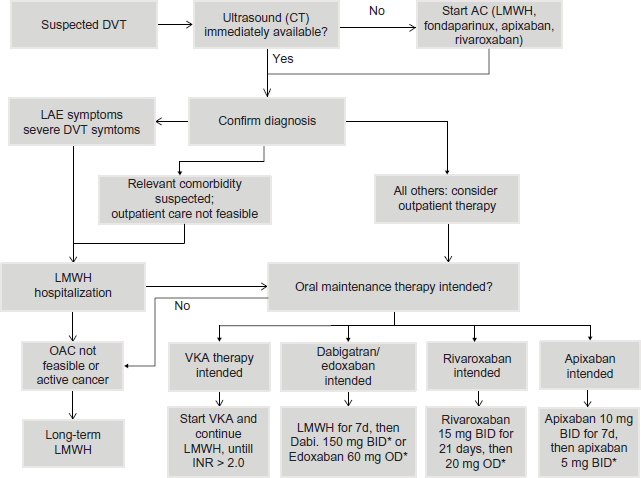
Flowchart of treatment decisions in the management of patients with DVT.
Of note, especially high-risk patients may benefit from NOAC treatment in the initial and maintenance phases of DVT treatment. In daily care, many patients with VTE are elderly and demonstrate significant comorbidities, which contribute to high rates of VTE and bleeding complications, especially in the early treatment phases. Such patients are often referred to as being frail or fragile, which can be defined as older than 65 years, renal impairment (creatinine clearance <50 mL/minute), or low body weight (<50 kg). 41 Due to the partial renal elimination of the NOACs, there is potential for accumulation of the anticoagulant in patients with renal impairment. Of note, all NOACs demonstrate different proportions of renal excretion, which results in different label recommendations for patients with renal impairment. 34 Detailed data for more than 1500 fragile patients are available from a subgroup analysis of the pooled EINSTEIN DVT and PE results. 41 Rates of recurrent VTE were numerically higher in fragile patients than in nonfragile patients (rivaroxaban 2.7% vs 1.9%; standard therapy 3.8% vs 1.9%). Within the group of fragile patients, treatment with rivaroxaban was associated with a similar risk of VTE recurrence compared to VKA with a trend toward risk reduction (2.7% vs 3.8%; hazard ratio [HR] 0.68; 95% confidence interval [CI] 0.39–1.18), but major bleeding was drastically reduced by rivaroxaban therapy (1.3% vs 4.5%; HR 0.27; 95% CI 0.13–0.54). 41 Rivaroxaban also resulted in a significant net clinical benefit over warfarin in fragile patients, with an HR of 0.51 (0.34–0.77) for the combined endpoint of symptomatic recurrent VTE and major bleeding.
The investigators of the HOKUSAI trial also published the results of treated subgroups in the supplementary material of their publication. 42 In fragile patients, edoxaban showed a significantly lower rate of VTE recurrence than warfarin (2.5% vs 4.8%; P = 0.0408), whereas the rate for major and clinically relevant nonmajor bleeding was comparable (11.0% vs 13.7%; P = 0.8759).
Finally, a meta-analysis of elderly patients treated in phase III NOAC trials demonstrated that the beneficial effects of NOAC (compared to VKA) are especially pronounced in elderly patients. 43
Extended secondary prevention
While all DVT patients undergo at least initial and maintenance therapies, treatment during the extended phase is based on individualized risk assessment, and only patients at increased risk of VTE recurrence are in need of extended anticoagulation. However, the balancing of prolongation or discontinuation of therapy against the VTE recurrence risk is complicated in daily care and predictive VTE recurrence scores are of limited value.
First, the decision of whether to apply extended anticoagulation is simplest for the group of patients who have developed DVT after a relevant but transient trigger situation, such as trauma, major surgery, immobilization for acute illness, or pregnancy. These so-called provoked DVT patients are at low risk to develop recurrent DVT (~1.8% per year).44,45 Consequently, they do not need to receive extended secondary prevention and should stop anticoagulant treatment at three months. This also applies to patients with recurrent provoked DVT.
A second patient group is less well defined, but still easy to counsel: patients with recurrent unprovoked DVT and those with high-risk thrombophilia (such as antiphospholipid syndrome, established antithrombin or protein C deficiency, and homozygous factor V mutation) are known to be at high risk of recurrent DVT, PE, or even arterial thromboembolism. For these patients, life-long anticoagulation is indicated and, in most cases, therapeutic dosages should be used (at least until clear evidence suggests otherwise). 46
The remaining patients comprise the largest group, which, unfortunately, is the most difficult to counsel.47,48 They include
patients after a first episode of unprovoked DVT;
patients who developed DVT after “mild” provocation, such as long-distance travel, oral contraceptive, or mild leg trauma. In these situations, the trigger may also be regarded as “transient,” but certainly not comparable to a major surgical procedure. Such mild triggers are much more likely to reoccur;
patients with recurrent distal DVT and mild thrombophilia; and
cancer patients who have developed DVT and have recently completed cancer therapy and are currently in remission.
Do these patients need to continue DVT therapy for longer than three months? For six months, for a year, or forever? Which drug should be used, and at which dosage? Given the heterogeneity of this group, a simple and clear answer to these questions is lacking. However, for several scenarios, recommendations can be made as follows:
Patients with a first episode of proximal (ie, involving iliac, thigh, or popliteal vein segments) unprovoked DVT should continue with treatment provided the bleeding risk is low.
Patients with “mild” triggers that may have contributed to the DVT occurrence, such as hormone treatment, long-distance travel, or nonfracture trauma, may discontinue anticoagulation, provided that they stop taking hormonal contraceptives, consider thromboprophylaxis in recurrent trigger situations, and are reliable to return for objective testing in the case of symptoms of recurrent VTE.
Patients with recurrent unprovoked distal DVT, with or without mild thrombophilia, may stop anticoagulation, but this decision requires a detailed patient information and consent. While current guidelines recommend to treat every distal DVT only for three months, 46 the risk of a recurrence, which may well be a proximal DVT or PE, is still relevant. If the patient is not willing to take that risk, long-term treatment should be discussed with the patient.
The same holds true for patients with cancer-associated DVT who are in the early phase after curative cancer treatment. Guidelines recommend the continuation of anticoagulation for as long as the patient has “active cancer,” 46 but there is an ongoing debate as to how long a nonmetastatic cancer is “active” and what impact long-term antihormone or antiangiogenetic cancer therapies have on VTE recurrence and, consequently, duration or intensity of anticoagulation therapy.
In daily practice, most scenarios do not result in a clear-cut determination of VTE recurrence risk and continuation or discontinuation of anticoagulation. Consequently, the general risk of DVT recurrence needs to be explained to the patient and a decision involving patient preferences should be made. Commonly, physicians and patients are afraid of the bleeding risks related to long-term anticoagulation, which, together with the impact of taking drugs or injections on quality of life, often drives the wish to discontinue anticoagulation. However, for the NOACs, such as apixaban, dabigatran, and rivaroxaban, placebo-controlled studies have been performed on the efficacy and safety of extended secondary prevention in the large group of patients with uncertain benefits of treatment prolongation (Table 2).49–51 These studies consistently demonstrated the following:
a high rate of recurrent VTE (~8% in the year following maintenance therapy) in the placebo arms;
an impressive relative risk reduction of ~80% with an extended NOAC treatment; and
a very low risk of major bleeding (<1%).
A pooled analysis of the respective trials with apixaban (AMPLIFY-EXT), dabigatran (RE-SONATE), and rivaroxaban (EINSTEIN-EXT) demonstrated a reduction of VTE recurrence (NOAC vs placebo, 1.9% vs 10.9%/year; P < 0.0001) and lower all-cause mortality (NOAC vs placebo, 0.6% vs 1.1%/year; P = 0.1). 52
Although prolonged oral anticoagulation is usually considered expensive, a study from the US demonstrated that prolonged VTE treatment with NOACs results in a significant avoidance in medical costs (-$146, -$482, -$918, and -$344 for VTE patients treated with dabigatran, rivaroxaban, apixaban, and edoxaban, respectively) compared to patients treated with standard therapy. 53 This cost reduction was mainly driven by cost savings in major and clinically relevant nonmajor bleedings (for all NOACs), and also by a reduction of recurrent VTE costs (for apixaban, edoxaban, and rivaroxaban therapies) when compared to long-term VKA therapy. Similarly, a model has demonstrated the cost-effectiveness of extended rivaroxaban therapy in VTE against placebo (or no treatment). 54
Furthermore, in the apixaban study (AMPLIFY-EXT), 55 a prophylactic dose of apixaban of 2.5 mg BID was also tested and resulted in risk reduction as impressive as that of the therapeutic dosage and, at the same time, in bleeding complication rates at the level of placebo. Another study evaluating prophylactic dosages of rivaroxaban in this population is ongoing.
The potential of using prophylactic NOAC dosages of anticoagulants to prevent recurrent VTE may be especially important to patients at high risk of recurrent VTE with concurrent high risk of bleeding complications, such as fragile patients or patients with frequent falls. However, the risk of fatal VTE in elderly patients may be much higher than the risk of fatal bleeding. 56 Consequently, these patients usually need to continue anticoagulation, 52 but the search for the “lowest possible” dosage may improve the risk–benefit ratio of long-term anticoagulation.
Based on these considerations, the introduction of NOACs in daily care will probably shift decisions regarding long-term treatment toward continuation with prophylactic NOAC dosages in many patients.
In contrast, although recent trials indicated that aspirin may be superior over placebo to prevent recurrent VTE in the extended secondary prevention phase (relative risk reduction ~30%), aspirin is less effective than NOACs (relative risk reduction ~80%) and associated with a bleeding risk. Consequently, while aspirin may have been considered an alternative in the VKA era, it seems to have an inferior risk–benefit ratio compared to that of NOAC. The ongoing EINSTEIN CHOICE trial includes aspirin and two doses of rivaroxaban to directly compare aspirin against NOACs in extended secondary prevention.
Cancer-associated DVT
As indicated earlier, initial and maintenance therapies should be performed with LMWH in DVT patients with active cancer. 46 However, we lack evidence that LMWH offers further benefit for cancer patients after three to six months; therefore, a switch to a more convenient oral drug such as an NOAC should be discussed with the patient. The same holds true for patients who are not able or not willing to tolerate LMWH injections throughout the maintenance phase. While no specific NOAC trial for cancer-associated DVT has been performed so far, subgroup analyses of the phase III NOAC trials included several hundred cancer patients and did not indicate a lack of effectiveness.42,57,58 Recently, a randomized controlled trial comparing six months of LMWH against edoxaban in cancer-associated VTE was initiated.
DVT in pregnancy
Since VKA are associated with an unacceptable risk of embryopathy and NOACS are contraindicated in pregnancy because of their placental passage, the standard of care in pregnant DVT patients is LMWH or, if LMWH is not tolerated, fondaparinux. 59
Massive DVT in need for thrombolysis
Patients with acute iliac or caval thrombosis, such as cases of phlegmasia, may in some cases require immediate revascularization, which today is predominantly performed with catheter-directed thrombolysis. Patients considered to be candidates for thrombolysis should be treated with LMWH or intravenous UFH. 46 A switch from parenteral to oral anticoagulation postlysis is possible but, without supporting evidence, the authors recommend continuing LMWH until the end of initial therapy (seven days postthrombolysis) before oral drugs are started.
Role of immobilization or hospitalization in DVT treatment
The concept of immobilizing DVT patients is outdated, since early mobilization has been demonstrated not to increase the risk of embolization, 60 and large cohort studies have clearly proven that outpatient DVT treatment is feasible and safe for the majority of patients being diagnosed with DVT outside of hospitals. 61 Furthermore, it is also reasonable to state that patients developing DVT while in hospital may be safely mobilized, provided that adequate anticoagulation is immediately initiated.
Similarly, patients with acute DVT and extensive leg swelling, suspected malignancy, or other acute conditions that may have caused the DVT or may complicate VTE treatment should be admitted, since surveillance, intensified treatment, pain management, and discovery of underlying acute conditions may be more feasible in hospital.
Role of compression therapy in DVT
A detailed discussion of the pros and cons of compression therapy in acute and chronic DVT within the limits of this review is impossible, and the readers are advised to refer to the current literature.27–30 However, the following statements may help for orientation:
The more a DVT patient is affected by pain and leg swelling, the more likely he/she will benefit from a compression therapy (stocking or bandages), provided that the compression device is fitted correctly.
In contrast, the usefulness of compression in asymptomatic DVT-affected legs is at least debatable.
Patients receiving compression therapy need to be educated on proper use and the risk of developing pressure ulcers, which is a significant risk especially in paralytic or hemiplegic patients or patients with severe neuropathy. Daily skin inspections are necessary during compression therapy.
The concept of long-term compression to prevent PTS has been accepted for decades but a recent trial indicated that the effect of compression stockings on PTS is questionable. 62
In light of the current uncertainties, the authors recommend the routine use of compression stockings in the initial and maintenance phases (for approximately three to six months post-DVT diagnosis). At this timepoint, ultrasound assessment of residual venous obstruction and reflux in common femoral and popliteal veins should be performed, as well as a clinical assessment for symptoms of PTS. We would then recommend discontinuation of compression therapy in patients without clinical signs of PTS, recanalized veins, and absence of relevant deep vein reflux. All other patients should be instructed to either continue compression (if accepted) or to temporarily interrupt compression and restart, if signs or symptoms of PTS develop.
Conclusion
Although some readers may have had the impression that DVT therapy has become more complicated in the past few years, in fact, it has become better. Many well-performed studies have clarified a number of issues over the past 15 years, and with this improved understanding of DVT and the characteristics and problems of DVT patients, better treatment strategies have been developed. These new strategies allow for a much more tailored therapy of a frequent and potentially life-threatening condition. The last development at present, namely, the introduction of NOACs, has the potential to increase compliance, quality of life, and safety of DVT treatment for millions of patients worldwide. 63 The authors strongly believe that this will also improve the effectiveness of DVT therapy. However, to gain the best effectiveness and safety benefit from NOACs, we all need to make sure that physicians and patients develop an understanding of the different treatment phases of DVT, the available treatment options and their respective dosing regimens, and the need to adapt DVT treatment standards on an individualized basis.
Author Contributions
Wrote the first draft of the manuscript: HE. Contributed to the writing of the manuscript: HE, FM, JB-W. Agree with manuscript results and conclusions: HE, FM, JB-W. Jointly developed the structure and arguments for the paper: HE, JB-W. Made critical revisions and approved final version: HE, FM, JB-W. All authors reviewed and approved of the final manuscript.