
Abstract
New therapies are changing the outlook for breast cancer worldwide. Breast cancer is traditionally divided into hormone receptor-positive, HER2-positive, and triple-negative disease. We have seen the development of new drugs targeting each of these breast cancer groups with promising results. In this article, the novel treatments are discussed with reference to recent clinical trial data. In each group, treatments are emerging that have had positive results in clinical trials. We discuss the new therapies aimed at evading hormone resistance in hormone receptor-positive disease, which have substantially increased the disease-free survival of patients with metastatic breast cancer in clinical trials. We have also seen multiple new therapies targeting HER2 receptors, working synergistically with Herceptin leading to dramatic and durable disease responses. Finally, in triple-negative disease, we are starting to see the results of trials using immunotherapy. Across all the treatment groups, we have seen the emergence of new therapies that are specifically designed to target the molecular drivers of an individual's cancer, regardless of hormone or HER2 positivity. This is paving the way for a more personalized approach to breast cancer treatment.
Introduction
New and effective treatments have dramatically changed the prognosis for women with breast cancer in the last 20 years. 1 More women are cured from their early cancer or live longer with metastatic cancer. 2 Inevitably, however, the cancer can become resistant to our current treatments, and much research has focused on identifying the mechanism of this resistance and developing new therapeutic approaches to target the pathways involved. New treatments are now emerging, which will change the way that we treat breast cancer.
Breast cancer is traditionally treated according to its hormone and HER2 positivity. We therefore focus on these overarching classifications to discuss the new treatments in each area.
Hormone Receptor-Positive Disease
Hormone receptor-positive breast cancer, as defined by the presence of estrogren receptors (ER) and progesterone receptors (PR) in tumor cells, is classically sensitive to anti-ER therapy. Durable disease remissions can be achieved with minimal toxicity using hormone therapies such as tamoxifen and aromatase inhibitors. Inevitably, however, the upregulation of alternative signaling pathways in response to the anti-ER therapy leads to resistance to this hormonal therapy. Hormone resistance is a major therapeutic challenge, and recent research efforts have focused on overcoming this barrier. Figure 1 illustrates the signaling pathways that have been targeted in attempts to overcome hormone resistance.
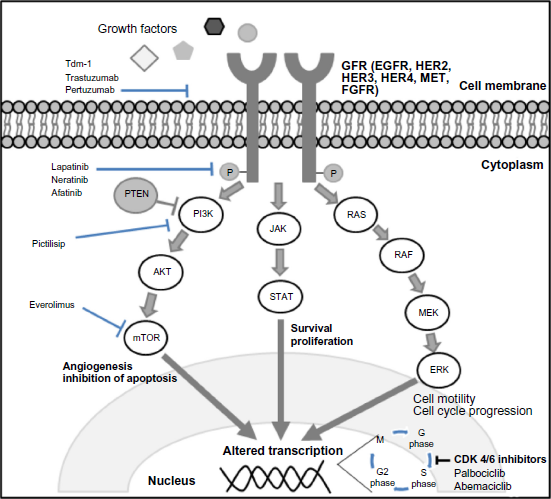
A cell diagram illustrating the signaling pathways thought to be involved in treatment resistance and the areas where novel treatments act.
CDK 4/6 inhibition
Palbociclib is an orally active highly selective inhibitor of CDK4 and CDK6. These kinases activate the d-cyclins and induce the cell to enter the S1 phase of cell replication and thus promote cell proliferation. Upregulation of this pathway is thought to underlie the ability of hormone-positive breast cancers to become resistant to hormone therapy.3,4 By inhibiting these proteins, palbociclib aims to overcome the ability of a cancer cell to become resistant to hormone therapy.
Initial trials of palbociclib have been encouraging. After an initial promising phase II study (PALOMA-1; Table 1) 5 where palbociclib was combined with the aromatase inhibitor letrozole in post-menopausal women with hormone receptor-positive metastatic breast cancer (MBC), two further randomized phase III trials have been conducted in either second- or first-line settings in advanced hormone receptor-positive breast cancer. Turner et al. 6 carried out a double-blind, phase III trial of palbociclib in combination with fulvestrant (PALOMA-3). The trial included both pre- and post-menopausal women with hormone-positive breast cancer that had progressed or recurred after hormonal treatment. The women could have received up to one line of chemotherapy in the advanced breast cancer setting. The participating 521 women were randomized 2:1 to palbociclib with fulvestrant or placebo with fulvestrant. The primary end point was progression-free survival (PFS) according to the RECIST version 1.1 criteria. The median PFS in the palbociclib/fulvestrant group was 9.2 months, compared to 3.8 months in the placebo/fulvestrant group (hazard ratio [HR] for disease progression or death, 0.42; 95% confidence interval [CI], 0.32–0.56; P < 0.001). 6 The main toxicities in the palbociclib arm were neutropenia, leukopenia, fatigue, and nausea (Table 1). The hematological toxicity was significant but without major clinical sequelae, with 78.8% of individuals in the palbociclib arm experiencing neutropenia of any grade versus 3.5% of individuals in the placebo group. The incidence of grade 3/4 neutropenia was 62%, and there was a low incidence of febrile neutropenia (0.6%).
Summary of recent trials of novel agents within hormone receptor positive breast cancer.

In the first-line metastatic setting, palbociclib demonstrated impressive results. The PALOMA-2 7 trial randomized 666 women with previously untreated MBC to palbociclib with letrozole or placebo with letrozole. The palbociclib arm was found to have a median PFS of 24.8 months versus 14.5 months in the placebo arm. Again, neutropenia occurred with a common finding, with 56.1% of individuals on palbociclib experiencing this at grade 3. The rate of febrile neutropenia was low, however, with just one (2.5%) patient experiencing this.
Both of the PALOMA trials have demonstrated the efficacy of palbociclib in the advanced breast cancer setting in both hormone-sensitive and hormone-resistant diseases. As a consequence of this, the US Food and Drug Administration (FDA) approved palbociclib in combination with fulvestrant in the second-line setting and in combination with letrozole in the first-line setting (Fig. 2). The activity of palbociclib in early breast cancer has yet to be established, but several adjuvant and neo-adjuvant trials are ongoing. Trials of two other CDK4/6 inhibitors (abemaciclib and ribociclib) in MBC are also underway (NCT02246621 and NCT01958021).
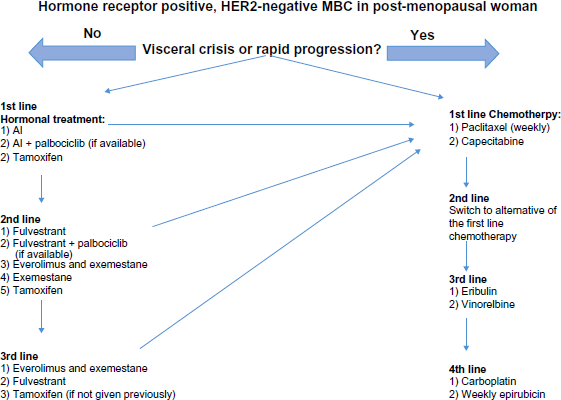
A diagram illustrating the lines of treatment in metastatic hormone receptor-positive, HER2-negative breast cancer. If at any time point, there is visceral crisis or rapid progression, a physician should move to treatments on the right side of the algorithm with chemotherapy-based treatment. This treatment algorithm assumes that a patient received an anthracycline in the adjuvant setting.
Inhibition of the PI3K/AKT/mTOR pathway
The PI3K/AKT/mTOR pathway (Fig. 1) is a downstream signaling pathway from the cell-surface tyrosine kinase receptors. Aberrant activation of this pathway is thought to underlie resistance to hormonal therapy. 8 Thus, inhibition of this pathway is an attractive therapeutic target aimed at overcoming endocrine resistance. The first drug to be licensed in this area was everolimus, the mTOR pathway inhibitor, which is now a standard second-line therapy in combination with exemestane after progression on hormonal treatment. Other promising drugs inhibiting PI3K and AKT function are still in clinical trial.
Everolimus
In the phase III BOLERO-2 trial (Table 1),9,10 post-menopausal patients with hormone receptor-positive MBC who had progressed on a non-steroidal aromatase inhibitor were randomized to everolimus with exemestane or placebo with exemestane. The trial demonstrated that the everolimus group had significantly longer PFS than the placebo group, at 11.0 months versus 4.1 months, respectively. The most common toxicities of grade ≥3 observed in the exemestane group were stomatitis (8% vs. 1%), fatigue (4% vs. 1%), and pneumonitis (3% vs. 0%). The positive results from this trial lead to the licensing of everolimus as a standard second-line therapy in both the USA and the EU in 2012–2013 for hormone-positive MBC that has progressed on hormonal therapy (Fig. 2).
PI3K inhibitors
Pictilisib is a pan-PI3K inhibitor (Fig. 1) that was recently investigated in a pre-operative window study of post-menopausal women with hormone receptor-positive, HER2-negative early breast cancer. 11 Women were randomized to pictilisib with anastrozole or anastrozole alone for two weeks prior to surgery. The primary outcome was suppression of Ki67. The group found that Ki67 was suppressed significantly more in the pictilisib arm, at 83.8% and 66.0%, respectively. Interestingly, the highest antiproliferation response was found in the luminal B cancer, but there was no benefit when pictilisib was added in luminal A cancer. There was no significant difference found in the groups that expressed a PI3K mutation.
In the metastatic setting, the FERGI trial (Table 1) 12 randomized women with MBC who had progressed on an aromatase inhibitor to receive pictilisib with fulvestrant versus fulvestrant alone. The pictilisib did not have a significantly longer PFS than the control group, and the drug was associated with more toxicities.
Further trials involving PI3K inhibitors taselisib (NCT02273973, NCT02389842, NCT02340221, NCT-02457910) and buparlisib are underway, which will clarify the role of these drugs in hormone-positive breast cancer. In the BELLE-2 trial (Table 1), women with MBC who had previously progressed on an aromatase inhibitor were randomized to either fulvestrant plus buparlisib or fulvestrant plus placebo. The overall results showed only a modest improvement in PFS of 6.9 months compared to five months with the addition of buparlisib, but with much greater toxicity, including transaminitis, hyperglycemia, rash, and neurological mood disorders. 13 Of interest, in the 31% of patients in whom archival primary tissue has an activating mutation of PI3KCA (the target of buparlisib), there was a significant improvement in PFS. However, by using a more reliable assay to measure PI3CA mutation status in circulating tumor DNA (ctDNA) at the time of the study entry in the metastatic setting, the investigators were able to demonstrate a significant improvement in PFS (3.2–7.0 months, HR 0.56, P < 0.001) in those with PIK3CA mutant ctDNA, with no improvement in those without a mutation. Thus, for the first time, a liquid biopsy from metastatic disease has identified a biomarker that might select those who could benefit from this specific targeted therapy. However, the toxicity from the drug means that it will not be developed in the future.
Similarly, the BELLE-3 trial (NCT01633060) is randomizing women to the same arms, but specifies that the women have previously progressed on mTOR inhibitors. The results of these trials will establish whether there is a role for PI3K inhibitors in the second- or third-line treatment in the hormone-positive MBC setting.
TKI inhibitors of HER2/EGFR
The development of resistance to endocrine treatment in hormone receptor-positive MBC has proved a major barrier ensuring a maintained response to treatment. One mechanism of resistance is thought to be underpinned by the interaction between receptors of the epidermal growth factor family (EGFR) and ErbB2 (HER2) with the ER receptor. 14 Overexpression of the HER2 receptor is thought to confer resistance to hormonal therapy. 15 Therefore, several attempts to overcoming this resistance have focused on inhibiting this interaction by duel targeting of the hormone receptor and the EGFR/HER2 family.
Lapatinib, a tyrosine kinase inhibitor that is active against both EGFR and ERB receptors (Fig. 1), has been licensed for use in HER2-positive disease. Its role in hormone receptor-positive disease was investigated in the EGF30008 phase III trial (Table 1). 16 The combination of lapatinib and letrozole was compared with letrozole and placebo in 1286 patients with hormone receptor-positive disease who had not yet received treatment in the metastatic setting (Fig. 3). The group found that the median PFS in hormone receptor-positive, HER2-positive individuals in the lapatinib/letrozole arm was longer than that of the letrozole/placebo arm, at 8.2 months versus three months, respectively, demonstrating a reduced risk of progression (HR 0.71; 95% CI, 0.53–0.96; P = 0.019). By contrast, the group found that in patients with MBC who had originally hormone receptor-positive and HER2-negative diseases (many of whom had presented with de novo MBC), there was no benefit in the addition of lapatinib (HR 0.90; 95% CI, 0.77–1.05; P = 0.188). In hormone receptor-positive, HER2-negative disease that progressed during or shortly after tamoxifen, there was a trend toward benefit in PFS that did not reach significance. This suggested that the role for EGFR blockers remains in the disease that is both ER and HER2 positive.
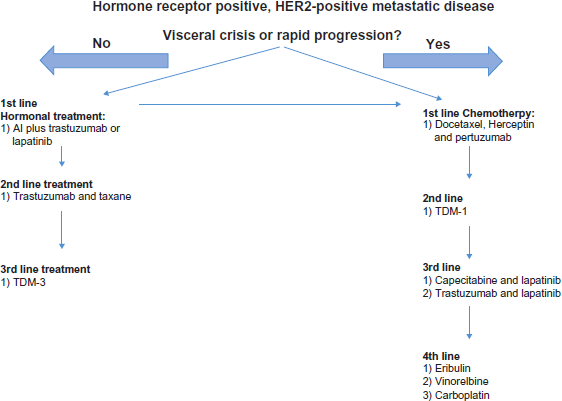
A suggested treatment algorithm for treatment of HER2-positive MBC. Disease progression should prompt movement to the next line of treatment. if there is rapid progression or visceral crisis, movement toward the right side of the algorithm and chemotherapy-based treatment is suggested.
A smaller phase III trial assessed the PFS in 291 postmenopausal patients randomized to fulvestrant with lapatinib or placebo. 17 The patients could have had up to two hormonal treatments in the adjuvant or metastatic setting, having demonstrated PFS for at least three months and up to one line of chemotherapy in the metastatic setting. The group found that there was no difference in the PFS between the lapatinib and placebo arms, with an HR of 1.04 (95% CI, 0.82–1.33; P = 0.37). Furthermore, there was no evidence for an interaction between treatment arm and HER2-positive status. The authors postulated that the low number of patients with HER2 overexpressing tumors (18%) may have meant that this trial did not have the power to demonstrate efficacy in this group, as Johnston's group had demonstrated. 16
Lapatinib has been licensed for use in hormone receptor-positive, HER2-positive MBC and can be used as an adjunct to both hormonal therapy and chemotherapy (Fig. 3).
HER2-Positive Disease
The human epidermal growth factor gene (HER2) encodes a tyrosine kinase transmembrane receptor of the EGFR family that is overexpressed in ~22% of breast cancers. 18 This receptor binds to extracellular ligands and subsequently alters downstream signaling and control of the cell cycle (Fig. 1). Its presence is known to cause the breast cancer to be more aggressive and is associated with a poorer prognosis. 18 The HER-2 receptor is therefore an attractive therapeutic target, with several new therapies being licensed in this area in recent years, which build upon the use of the anti-HER2 monoclonal antibody trastuzumab (Herceptin). Herceptin revolutionized treatment of HER2-positive disease in the adjuvant and metastatic setting. 19 New targeted therapies in this area have added further treatment lines, meaning that women can achieve durable disease control.
Anti-HER2 monoclonal antibody
Pertuzumab is a humanized anti-HER2 monoclonal antibody that acts by preventing dimerization of the HER-2 receptor with other EGFR receptors and HER-3, thereby reducing activation by ligand binding.20,21 It is known in vitro to work synergistically when given with trastuzumab in preventing cell signaling and thus promoting breast cancer cell death. 22 The CLEOPATRA trial investigated the combination of Herceptin and pertuzumab alongside chemotherapy (docetaxel) as the first-line therapy in the metastatic setting (Table 2).23,24 This randomized, double-blind, placebo-controlled trial enrolled 808 women >18 years of age with HER2-positive disease, locally advanced unresectable disease, or MBC. They could have received a maximum of one line of endocrine treatment but no chemotherapy in the metastatic setting. Women were randomized to placebo, trastuzumab and docetaxel or pertuzumab, trastuzumab, and docetaxel. The pertuzumab group showed a significantly improved overall survival compared to the placebo group, with a median overall survival of 56.5 months (95% CI, 49.3 to not reached) versus 40.8 months (95% CI, 35.8–45.3%), respectively. There was a ≥5% increased rate of (any grade) diarrhea, rash, mucosal inflammation, and febrile neutropenia in the pertuzumab group. There was also a higher rate of grade 3 febrile neutropenia in the pertuzumab group compared to the controls, at 13.8% versus 7.6%, respectively. There was no increase in the rate of left ventricular dysfunction in the pertuzumab group.
Summary trials of novel agents within HER2 positive breast cancer.

In early breast cancer, pertuzumab has also been shown to be effective in the neoadjuvant setting when given in conjunction with standard taxane-based chemotherapy, trastuzumab, and surgery. The NeoSphere study 25 randomized 417 women with early operable HER2-positive disease to docetaxel plus trastuzumab, docetaxel plus pertuzumab, docetaxel plus pertuzumab and trastuzumab, and pertuzumab with trastuzumab alone. The highest rate of pathological complete response was found in the chemotherapy in the dual antibody group at 49%, compared to 31% in the chemotherapy/trastuzumab group, 23% in the chemotherapy/pertuzumab group, and 18% in the antibody group. There were fewer pathological complete responses in the hormone-positive, HER2-positive tumors compared with hormone receptor-negative, HER2-positive tumors. The toxicity profile was similar across all chemotherapy-containing arms. The most common toxicity at grade ≥3 was febrile neutropenia, at 7–8% in the arms including chemotherapy.
In the adjuvant setting, the role of pertuzumab is being assessed in the large, international APHINITY trial. This trial is a randomized, double-blind, controlled study comparing the outcomes of adjuvant trastuzumab, pertuzumab, and chemotherapy with trastuzumab, placebo, and chemotherapy. The results are expected in late 2017/2018.
Antibody–drug conjugate
TDM-1 is an antibody-drug conjugate combining trastuzumab with the microtubule-inhibitory cytotoxic agent DM-1 (a derivative of maytansine). The combination allows the drug to effectively target and attach to the HER-2 overexpressing cells, leading to the intracellular delivery of the chemotherapy agent to tumor cells rather than the normal tissue.
The EMILIA trial (Table 2) 26 was a randomized, open-label phase III study comparing the efficacy and safety of TDM-1 versus the combination of capecitabine and lapatinib in 991 patients with HER2-positive metastatic disease who have previously received trastuzumab and a taxane. The primary end point was PFS, as defined by the RECIST criteria. The TDM-1 arm had significantly improved PFS (median PFS, 9.6 months vs. 6.4 months with lapatinib plus capecitabine; stratified HR for progression or death from any cause 0.65; 95% CI, 0.55–0.77; P < 0.001). In addition, there was a significant improvement in the overall survival (30.9 months vs. 25.1 months). The incidence of grade 3 events was higher in the capecitabine/lapatinib arm than the TDM-1 arm, at 57.0% versus 40.8%, respectively. The most common grade 3 or 4 events in the TDM-1 arm were thrombocytopenia (12.9%) and elevated liver enzymes. On the basis of the positive findings from this trial, the drug was licensed by the FDA in 2013 and is now the standard of care for the second-line treatment of metastatic HER2-positive breast cancer (Fig. 3).
Further evidence for the efficacy of TDM-1 was gained from the TH3RESA trial (Table 2), a randomized, open-label phase III trial comparing TDM-1 to treatment of physician's choice in patients who had previously progressed on two lines of HER2-directed therapy. 27 The patients in the TDM-1 arm were found to have significantly improved PFS at 6.2 months compared to 3.3 months in the comparator arm (stratified HR 0·528, 95% CI, 0·422–0·661, P < 0.0001). There were three deaths attributable to the drug in the TDM-1 arm (<1%, hepatic encephalopathy, subarachnoid hemorrhage, and pneumonitis) and one in the physician's choice arm (<1%, non-cardiogenic pulmonary edema).
The role of TDM-1 as the first-line treatment for metastatic HER2-positive breast cancer was addressed by a randomized phase II trial of 137 patients. 28 The patients who had not received chemotherapy or trastuzumab in the metastatic setting were randomized to TDM-1 or trastuzumab with docetaxel. The TDM-1 had a significant improved PFS compared to the trastuzumab/docetaxel arm (14.2 months vs. 9.2 months, respectively), giving an HR for progression of 0.59 (P = 0.035). In a follow-up phase III trial (MARIANNE), however, TDM-1 did not compete so well against the standard first-line therapy of Herceptin with a taxane, 29 with no PFS benefit. Thus, at present, TDM-1 remains a second-line therapy for HER2-positive metastatic disease.
Further studies are addressing the role of TDM-1 in the adjuvant treatment of breast cancer. The KAITLIN trial (NCT01966471), which is now closed to recruitment, has 1846 randomized women who have reviewed anthracycline to receive TDM-1 with pertuzumab or trastuzumab with pertuzumab and taxol, and the results are expected in a few years’ time.
TKI inhibition
Lapatinib
Lapatinib acts by inhibiting the tyrosine kinases of the EGFR and HER2 receptors, preventing autophosphorylation and thus downstream signaling. In the metastatic setting, a phase III open-label trial enrolled 324 women with MBC who had progressed on trastuzumab and randomized them to capecitabine with lapatinib or capecitabine alone (Fig. 1 and Table 2). 30 The group found that the mean time to progression in the combination arm was 8.4 months compared to 4.4 months in the monotherapy group. This indicated a role for the combination therapy in metastatic HER2-positive cancer that had previously progressed on trastuzumab, and the combination became a licensed second/third-line option in the EU and the USA (Fig. 3).
In the early breast cancer setting, lapatinib has been investigated in combination with trastuzumab rather than with chemotherapy. This is because it works synergistically with trastuzumab in blocking phosphorylation and dimerization of the HER receptors. The efficacy of lapatinib in combination with trastuzumab in the neo-adjuvant setting is supported by trials.31,32 The NeoALTTO trial 32 randomized 455 women with early breast cancer to receive oral lapatinib or IV trastuzumab or combination treatment for six weeks, followed by an ongoing therapy for 12 weeks given alongside weekly paclitaxel. The group found that the combination therapy arm experienced significantly higher pathological complete response rates compared to the monotherapy arms (51.3% compared to 29.5% in the trastuzumab group and 24.7% in the lapatinib group). The group given lapatinib had a higher rate of grade 3 and 4 events compared to the trastuzumab alone arm. The most common grade 3 toxicity was diarrhea, at 23.4% in the lapatinib arm, 21.1% in the combination arm, and 2% in the trastuzumab arm. The incidence of neutropenia, liver enzyme derangement, and diarrhea increased when paclitaxel was added to the regimen after six weeks.
The case for combination therapy of lapatinib with trastuzumab in the adjuvant setting is less compelling. A large randomized phase III trial in 4000 patients (ALTTO 33 ) found that the HR for disease-free survival in the superiority comparison of lapatinib and trastuzumab versus trastuzumab alone was only 0.96 (97.5% CI, 0.80–1.15; P = 0.61). Thus, there is no role for lapatinib in early breast cancer.
Neratinib
Neratinib is an irreversible pan-ErbB receptor tyrosine kinase inhibitor of HER-1, HER-2, and HER–4. This new drug showed promising results in a phase II trial within the HER2-positive MBC setting where patients had received up to four lines of chemotherapy in the metastatic setting (Table 2). 34 The median PFS was 39.6 weeks and 22.3 weeks in the trastuzumab-naive and trastuzumab pre-treated groups, respectively. However, in this early phase III study, there was a high rate of diarrhea (21% experienced grade 3–4 diarrhea).
Chan et al. 35 have investigated whether this drug should be used in the early breast cancer setting as an adjunct to trastuzumab. In this phase III trial, the group randomized women with stage 1–3 HER2-positive breast cancer who had completed adjuvant treatment with trastuzumab to neratinib or placebo. The median follow-up time was 24 months. The group found that there was a significant 33% reduced risk of a disease-free survival event in the neratinib group compared to placebo. Disease-free survival was significantly improved in the neratinib compared to the placebo group (93.9% vs. 91.0%; HR 0.63; 95% CI, 0.46–0.84; P = 0.0017). In particular, this benefit was greatest in those with hormone receptor-positive, HER2-positive tumors when neratinib was given concurrently with endocrine therapy, implying potential synergy between these therapies. There was a significantly higher toxicity in the neratinib group, with 40% in the neratinib group experiencing grade 3 diarrhea compared to 2% in the placebo group. This trial suggests that there may be a role of neratinib in the adjuvant setting, and a licensing application has been submitted.
Afatinib
Afatinib, similar to neratinib, acts by irreversibly blocking transmembrane ErbB/HER receptors, preventing downstream signaling. 36 In a single-arm phase II trial, Lin et al. 37 demonstrated that afatinib had activity in metastatic HER2-positive breast cancer that had previously progressed through trastuzumab. The patients had a median value of 3 prior to chemotherapy treatments. Overall, 46% of the patients were classified as having clinical benefit.
In a recent phase III trial, afatinib in combination with vinorelbine was compared to trastuzumab plus vinorelbine (LUX-Breast 1 trial 38 ; Table 2). The patients were eligible if they had progressive disease following adjuvant treatment (progressed within 12 months of completing treatment) or first-line treatment (progressed within six months) for metastatic HER2-positive breast cancer with trastuzumab. Recruitment for this trial was stopped early after by an independent data-monitoring committee after risk–benefit analysis. Overall, afatinib did not improve PFS over trastuzumab, and there was a significantly lower overall survival in the afatinib group (20.5 months versus 28.6 months, respectively; P = 0.0048).
In view of these advances, the management of HER2-positive disease has dramatically changed in the last five years with the licensing of therapies such as pertuzumab and T D M -1 (Fig. 4). The outlook for HER2-positive disease is now much more optimistic, with further lines of therapy with the potential of durable disease control, and many patients with HER2-positive MBC live with stable, well-controlled disease for many years.
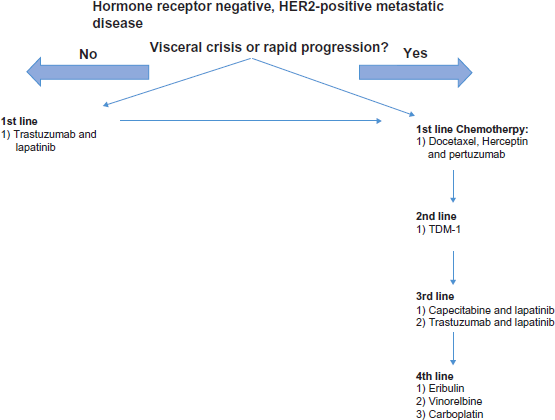
A treatment algorithm for treatment of hormone-negative, HER2-positive MBC. Disease progression should prompt movement to the next line of treatment. If there is rapid progression or visceral crisis, movement toward the right side of the algorithm and chemotherapy-based treatment is suggested.
Triple Receptor-Negative and BRCA Mutation-Related Disease
Triple-negative breast cancer (TNBC), which accounts for ~15–20% of all breast cancers, is tumor that lacks both the ER and PR receptors and does not overexpress the HER2 protein. In fact, there is evidence that these are a more heterogeneous group of disease with seven or more subtypes of TNBC, as defined by gene expression profiling. 39 Until recently, the management of TNBC lacked therapeutic targets, and anthracyclines, taxanes, and platinum-based chemotherapy formed the backbone of treatment. In particular, there has been much interest in the role of platinum-based chemotherapy in TNBC. 40 The TNT trial suggested that while there is no benefit of platinum-based therapy over taxanes in unselected TNBC, BRCA-related TNBC achieves better response rates to platinum-based chemotherapy. 41 This trial has prompted the addition of carboplatin to adjuvant chemotherapy regimens in some centers within this setting.
Recently, increased understanding of the molecular profile of the cancers has prompted trials with more targeted treatments. One subtype of TNBC, which has found to have increased expression of genes relating to T-cell function, the so-called immunomodulatory subtype, has become a target for immunotherapy with the hope that we will see responses as dramatic as those seen in melanoma and renal cell cancer. Another subtype contains the androgen receptor and may benefit from an endocrine approach. A further subtype is thought to be driven by somatic or germline BRCA mutations, and this particular subtype has therefore been hypothesized to be susceptible to poly(ADP-ribose) polymerase (PARP) inhibition.
Immunotherapy
Activated T-lymphocytes express the PD 1 receptor (Fig. 5). Its ligands, PD-L1 and PD-L2, bind and cause an inhibitory effect. In vivo, this feedback mechanism protects from overactivation of the immune system. Some breast cancers, however, are known to express these ligands and in doing so, avoid detection by the immune system.
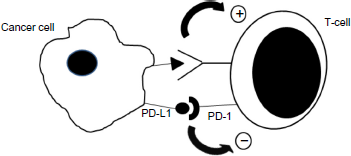
An illustration of the interaction between the PD-1 receptors on T-cells and PD-L1 ligand on cancer cells, causing downregulation of the T-cell response. Immunotherapy blocks either the PD-L1 ligand or the PD-1 receptor, preventing the downregulation of the immune system.
Pembrolizumab
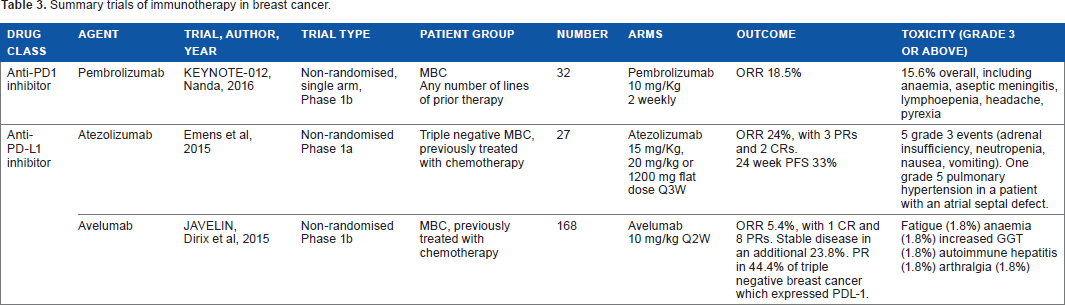
Pembrolizumab is an immunotherapy that acts by blocking PD-1 receptors on T-cells. It has shown promising results with durable antitumor activity in non-small cell lung cancer, advanced melanoma, advanced gastric cancer, urothelial cancer, and head and neck cancer. 42 Several trials are currently recruiting to investigate pembrolizumab in the setting of TNBC, on note, a recent phase Ib single agent study (KEYNOTE-012; Table 3) of pembrolizumab in 111 patients with metastatic TNBC. 43 The patients received 10 mg/kg intravenous pembrolizumab twice weekly. Overall, the group found that 37.5% of patients had a reduction in their tumor burden from baseline. One patient (3.7%) had a complete response, four (14.8%) had a partial response, and seven patients (25.9%) had stable disease. Treatment-related toxicity was prevalent, with 56.3% of patients experiencing at least one toxicity and 15.6% of patients experiencing a toxicity of grade ≥3. The median duration of stable disease was 17 weeks, with some individuals demonstrating stable disease for over 24 weeks. Of note, the patients who demonstrated PDL-1 positivity were more likely to have had a response to treatment.
Summary trials of immunotherapy in breast cancer.
Further, KEYNOTE trials are establishing whether pembrolizumab is competitive against the current standard therapy. KEYNOTE-119 (NCT02555657) is a phase III trial randomizing patients to single-agent pembrolizumab or chemotherapy of the physician's choice. The results from the initial KEYNOTE-012 trial indicate that this treatment may be effective in some patients with TNBC, with potential durable responses.
Atezolizumab
Atezolizumab is an anti-PDL-1 inhibitor that has shown promising results in an initial phase Ia trial in metastatic TNBC (Table 3) 44 with any level of PDL-1 expression. Emens et al found that of 27 heavily pre-treated patients given atezolizumab, nearly one-quarter had an objective response (24%, 95% CI, 8–47%). Overall, there was a 24-week PFS of 33% (95% CI, 12–53%). The common toxicities associated with the treatment were fatigue (22%), pyrexia (15%), neutropenia (15%), and nausea (15%). Overall, 11% of the patients experienced adverse events (adrenal insufficiency, neutropenia, nausea, vomiting) of grade ≥3. As a result of this trial, a phase III trial of atezolizumab alongside Abraxane (selected to avoid steroid use) in the first-line treatment of metastatic TNBC (IMPASSION, NCT02425891) is currently recruiting.
Avelumab
Avelumab is an IgGl antibody that acts by inhibiting tumor cell-expressed PDL-1. In a phase lb trial (Table 4), 45 168 patients with MBC, which could be any hormone receptor or HER2 status. While the overall objective response rate (ORR) was 5.4% (95% CI, 2.5–9.9%) in the entire cohort, one-third of patients with PD-L1 expressing tumors had a partial response. In patients with TNBC that expressed PDL-1, 44.4% had PRs. Overall, 14.3% patients experienced toxicities of grade ≥3, which were fatigue (1.8%), anemia (1.8%), increased gamma-glutamyl transferase (1.8%), autoimmune hepatitis (1.8%), and arthralgia (1.8%). There were two treatment-related deaths (acute liver failure and respiratory distress).
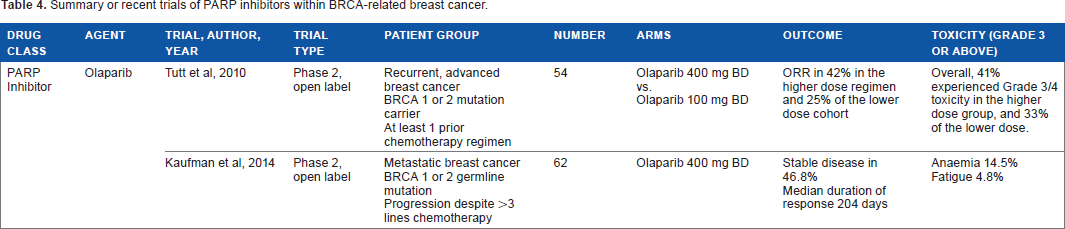
Summary or recent trials of PARP inhibitors within BRCA-related breast cancer.
PARP inhibitors
BRCA-related cancers, which comprise ~70% of TNBCs, are known to have a defect in the homologous recombination DNA repair pathway. PARPs are enzymes involved in DNA repair in a second, base excision pathway. PARP inhibitors mediate cell death by preventing DNA repair in the base excision pathway, while the homologous recombinant DNA pathway is also defective.
To date there have been a number of phase I and II trials (Table 4) investigating the role of olaparib and niraparib in BRCA-associated breast cancers. Tutt et al performed a proof-of-concept phase II open-label trial of olaparib in BRCA-1-and -2-related advanced breast cancer. 46 The patients had received at least one line of chemotherapy in the metastatic setting. It should be noted that only between 50% and 64% of the patients were triple negative. The group found that the patients given the higher dose of olaparib 27 had a PFS of 5.7 months (95% CI, 4.6–7.4) and an ORR of 41% in the group given the higher dose.
A further phase II study basket study of olaparib included 62 patients with a BRCA mutation. 47 In this group, the progression-free survival was 3.7 months. Tumor response was similar in both the hormone receptor-positive and -negative breast cancers (12.5% vs. 13.3%) respectively. These results may reflect the fact that, compared to the participants in the study of Tutt et al, these patients were more heavily pre-treated. The drug was generally well tolerated, with the most common toxicity of grade ≥3 being anemia, at 14.5%.
Phase III trials are currently undergoing in the metastatic (BRAVO, NCT01905592; OlympiAD, NCT02000622; Brocade 3, NCT02163694; ABRAZO, NCT02034916) and adjuvant (OlympiA, NCT02032823) settings. Overall, PARP inhibitors are in the early stages of development, but results in other tumor types such as ovarian cancer provide optimism that PARP inhibitors will be an effective treatment in BRCA-related breast cancer.
Conclusion
In the last decade, there has been an increased understanding of the pathophysiology of cancer and its ability to become resistant to cancer and evade the immune system. This has allowed us to develop novel treatments that can target the specific molecular pathways. For instance, we have seen that the upregulation of the PI3K/AKT/mTOR pathway underlies the resistance to hormonal treatment. Inhibition of this pathway with the mTOR inhibitor everolimus has seen improvement in PFS in previously hormone-resistant disease from 4.1 months to 11 months. A second example is in immunotherapy, where we are beginning to see that the patients with the best chance of response are those who have tumors that display PDL-1. Thus, again we are able to target our treatment to those who are more likely to respond. In the coming years, we are likely to see the results of trials validating this approach, prompting paradigm shift in our approach to breast cancer management.
Author Contributions
Conceived and designed the experiments: BK, SJ. Analyzed the data: BK, SJ. Wrote the first draft of the manuscript: BK. Contributed to the writing of the manuscript: BK, SJ. Agree with manuscript results and conclusions: BK, SJ. Jointly developed the structure and arguments for the paper: BK, SJ. Made critical revisions and approved final version: BK, SJ. Both authors reviewed and approved of the final manuscript.