
Abstract
Chemotherapy has the potential to deplete and destroy a woman's reproductive potential. Although many oncologists are referring women for fertility preservation before chemotherapy, in many cases there is limited time for fertility preservation. This review provides an overview of the impact of cancer and chemotherapy on the ovarian reserve, a summary of methods of fertility preservation prior to chemotherapy, and current knowledge of fertility preservation techniques after gonadotoxic chemotherapy.
Keywords
Introduction
As survival rates and life expectancy of those with malignancy continue to improve, increasing numbers of young women are referred for fertility preservation. Fertility is indeed a crucial issue for women of reproductive age dealing with cancer, and counseling regarding fertility preservation should be offered routinely. Ideally, fertility preservation should be considered before treatment with chemotherapy or radiation. However, often chemotherapy must be initiated immediately, with no available window of opportunity for fertility considerations. In these cases, fertility preservation can only be considered after the ovaries have already been exposed to chemotherapy.
Chemotherapy and radiotherapy can severely affect a woman's ovarian reserve, damaging the primordial follicles and reducing the follicular pool.1–3 Radiotherapy affects the pelvic organs when there is direct pelvic irradiation (external beam or intracavity). 4 This radiation exposure could be diminished by relocating the ovaries outside the radiation field outside the pelvis (ovarian transposition or oophoropexy).
The choice of fertility preservation technique depends on the patient's age, ovarian reserve, urgency of treatment, and marital status. It should be a joint decision of the reproductive endocrinologist, oncologist, the patient, and her partner.
This review provides an overview of the impact of cancer or chemotherapy on the ovarian reserve, a summary of methods of fertility preservation prior to chemotherapy, and current knowledge of fertility preservation options after gonadotoxic chemotherapy.
Physiology of Ovarian Aging
At birth, the ovaries contain a finite number of primordial follicles (approximately 1-2 million). There is no potential for regeneration of these follicles and most remain in an arrested state. From puberty to menopause, a few primordial follicles are recruited each month, and only one dominant follicle becomes mature and reaches ovulation; the rest are lost to atresia. During physiological reproductive aging, between the mid-thirties and menopause, the primordial follicle count declines rapidly. This is associated with decreased oocyte quality, increased aneuploidy, and reduced fertility and fecundity.5,6
Reduced ovarian reserve and reproductive potential can be quantified by changes in markers including reduced antral follicle count (AFC), increased serum FSH (follicular stimulating hormone), reduced AMH (antimullerian hormone) and reduced inhibin-B. 7 AMH is secreted by the granulosa cells of primary and secondary pre-antral follicles, and inhibin B by small antral follicles, believed to be sensitive to FSH stimulation. 8 AFC appears to represent the recruitable primordial follicle pool.
Impact of Cancer on Ovarian Reserve
It is known that semen quality in males with malignancy, especially in those with testicular cancer and lymphoma, is often poor.9–12 This has been attributed to either the direct effect of the malignancy on testicular function or alteration of immunologic response. In females, the effect of malignancy on ovarian function remains unclear.
Several retrospective studies have addressed the potential impaired ovarian reserve due to malignancy. For example, Pal et al compared the in vitro fertilization (IVF) outcomes of 5 women with malignancy with 12 women with tubal factor infertility 13 and found that cancer was associated with a reduction in oocyte maturity and quality and decreased fertilization rate. The authors postulated a possible detrimental biological effect of the malignancy on the oocytes. In another study, Lawrenz et al compared a group of women with Hodgkin's and non-Hodgkin's lymphoma (pretreatment) with healthy controls. 14 They found lower serum AMH levels as well as decreased response to IVF treatment in those with disease, suggesting that malignancy itself may be deleterious to the ovarian reserve.
Quintero et al compared 50 women with malignancy with predicted good response to ovarian stimulation with 50 age-matched controls that underwent IVF for male factor infertility. 15 The number of oocytes and mature oocytes and the number of fertilized oocytes were comparable between the two groups. However, significant differences were demonstrated in the dose and length of gonadotropin stimulation required, suggesting possible damage of the functional ovarian reserve in women with malignancy.
Other studies have failed to demonstrate the differences in the response to gonadotropin between women with malignancy and the control group. Knopman et al reported comparable serum estradiol (E2) and number of oocytes retrieved in women with malignancy and in healthy controls stratified by age. 16 Das et al showed no difference in ovarian reserve (AFC and FSH) and response to treatment (total treatment dose and number of oocytes retrieved) among women with malignancy undergoing prechemotherapy fertility preservation and age-matched controls. 17 Michaan et al compared women undergoing “emergency” IVF prior to commencing chemotherapy with a control group of women with mechanical factor infertility. 18 They did not find any difference in the total gonadotropin dosage, number of retrieved oocytes, fertilization rate, and clinical pregnancy rate. Robertson et al compared women with malignancy undergoing embryo banking with healthy controls undergoing IVF for male factor infertility. 19 No difference in gonadotropin dose, number of oocytes retrieved, and number of embryos were found.
A recent meta-analysis of 7 studies evaluated ovarian response to controlled ovarian hyperstimulation (COH) in women with malignancy undergoing fertility preservation prior to treatment and age-matched controls. 20 The mean number of oocytes in cancer patients (11.7 ± 7.5) was significantly lower than in the control group (13.5 ± 8.4; P = 0.002; 95% Confidence Interval [CI], -2.98 to -0.62). The number of mature oocytes in the control group (13.5 ± 8.4) was also lower in the cancer patients (11.7 ± 7.5; P = 0.02; 95% CI, -2.94 to 0.62). The incidence of poor responders in the cancer group (7.69%) was comparable to that in the control group (5.88%). The relative risk was 1.32 (95% CI, 0.78-2.2).
Moria et al evaluated 129 women with malignancy who underwent in vitro maturation treatment (IVM) for fertility preservation with 100 control women. 21 They found that women with breast cancer had fewer retrieved oocytes than the control group (P < 0.05; 95% CI, 0-5), but ovarian reserve and oocyte maturity in other types of malignancy were similar. This study suggests that women with breast cancer may have a malignancy-mediated reduced ovarian reserve, reflected in fewer retrieved oocytes. Studying women with BRCA mutations, Oktay et al reported that women with BRCA1 mutation yielded fewer oocytes and demonstrated reduced response to gonadotropin stimulation compared to women with no mutation. 22 This may imply a specific effect of breast malignancy on ovarian reserve.
Impact of Chemotherapy on Ovarian Reserve
Chemotherapy has varying effects on ovarian function (Table 1). The most gonadotoxic chemotherapeutic agents are alkylating agents such as cyclophosphamide. 23 Chemotherapy induces apoptosis of the primordial follicle pool, damage to the ovarian cortex, ovarian atresia and reduced ovarian blood flow. 1 Since chemotherapy affects proliferating cells, primordial follicles at rest during treatment may be protected. In animal models, depletion in primordial follicles correlates with increasing doses of chemotherapy. 24
Chemotherapy and ovarian toxicity.
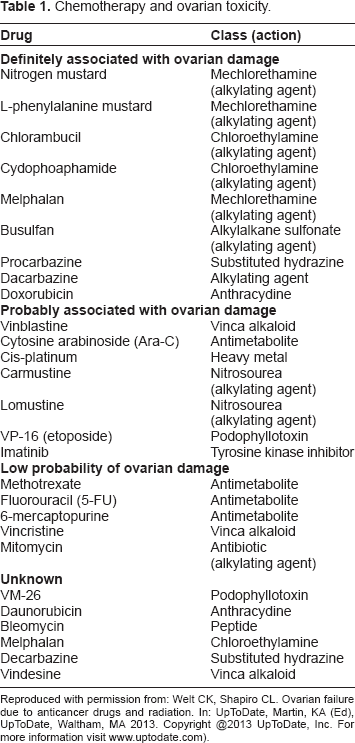
Reproduced with permission from: Welt CK, Shapiro CL. Ovarian failure due to anticancer drugs and radiation. In: UpToDate, Martin, KA (Ed), UpToDate, Waltham, MA 2013. Copyright @2013 UpToDate, Inc. For more information visit www.uptodate.com).
The worst reproductive consequence of chemotherapy is irreversible ovarian failure leading to permanent sterility and early menopause. Many women have transient amenorrhea. However, even in those who resume menstruation, the primordial follicle pool may be diminished.25,26 Following chemotherapy, women may have early menopause with a period of reduced fertility and then premature ovarian failure. This may occur several years after the completion of chemotherapy.27,28
Several studies have assessed markers of ovarian reserve and treatment outcome in women after chemotherapy. Bath et al analyzed biochemical markers (FSH, E2, inhibin A, inhibin B, pro-αc-inhibin, and AMH) and ultrasound markers (AFC and ovarian volume) in young survivors of childhood cancer with regular menstrual cycles. 26 The results were compared with healthy controls with regular menstrual cycles. They also compared cancer survivors taking the oral contraceptive pill (OCP) with healthy OCP users. Compared with the control group, cancer survivors demonstrated higher serum FSH and lower AMH levels. This indicates partial loss of ovarian reserve despite normal regular menses. Similarly, Larsen et al reported reduced ovarian reserve despite normal menses and serum FSH of <10 IU/L in childhood cancer survivors. 25 These women demonstrated diminished ovarian volume and AFC and decreased cycle length.
In a study of 50 premenopausal women with early breast cancer, Anderson et al compared hormonal and ultrasound markers of ovarian reserve before treatment and at 3-month intervals up to a year postchemotherapy. 29 Before treatment, the first marker affected was serum AMH concentration. Compared with serum Inhibin B (modest reduction) and estradiol (maintained), AMH was also the marker that decreased most rapidly after treatment. Lutchmann Singh et al assessed biochemical markers (FSH, luteininzing hormone [LH], E2, Activin, Inhibin A, Inhibin B, and AMH) and biophysical markers (AFC, ovarian volume, pulsatility index, peak systolic velocity, and endometrial thickness) of ovarian reserve in women with breast cancer compared with age matched controls. 30 They measured markers before and after IVF and after chemotherapy. Before chemotherapy, no significant differences were noted between the groups. After chemotherapy, women with breast cancer showed significantly lower basal AMH, inhibin B and AFC, and higher basal FSH. This suggests that both mature primordial follicles and early antral follicles are influenced by chemotherapy.
Studies reporting ovarian reserve and IVF outcome in women with malignancy after chemotherapy indicate reduced ovarian reserve as expressed by decreased IVF outcome. One study compared women 12 to 24 months after chemotherapy with an age-matched control group of healthy women undergoing IVF for male infertility. 31 Compared with the control group, the cancer group had lower AFC, lower peak estradiol, and fewer oocytes retrieved. Dolmans et al compared women with malignancy undergoing IVF before and during chemotherapy. They found less favorable outcomes in the women who had already undergone one cycle of chemotherapy (higher doses of gonadotropin required and fewer oocytes retrieved). 32
It seems that chemotherapy has a negative impact on ovarian reserve and actual IVF outcome. It accelerates the process of ovarian aging and shortens the window of fertility prior to ovarian failure. Adjuvant treatment, such as tamoxifen for estrogen-receptor sensitive breast cancer may also shorten the window of fertility. Although it has no effect on ovarian reserve, the time required to complete and recover from treatment delays fertility for a few years.
Determinants of Impact of Chemotherapy on Ovarian Reserve
Reduced ovarian reserve after chemotherapy depends on many factors including age, cancer type and severity, baseline ovarian reserve prior to chemotherapy, and the actual treatment regime. As women age and ovarian reserve declines, the remaining follicular pool is more sensitive to depletion and damage, and there is an increased risk of premature ovarian failure following chemotherapy.4,23,27 The drug, dose, duration of treatment, and method of administration influence the degree of insult to the ovarian reserve. 33
Gonadotoxicity of Radiotherapy
The gonadotoxic effects of radiotherapy also vary with age and dose. Radiotherapy depletes the already diminished primordial follicle pool in older women. Compared with the risk to young girls, the same dose of radiation carries a higher risk of radiotoxicity to the adults. Besides ovarian failure, 34 pelvic radiation can also damage the uterus. It may lead to increased spontaneous abortion, preterm labor, and low birth-weight infants.4,33,35
Options for Fertility Preservation Prior to Chemotherapy
The choice of fertility preservation technique depends on the patient's age, ovarian reserve, urgency of treatment, marital status, and disease prognosis. It requires careful counseling and guidance combined with realistic expectations of treatment success. Options for fertility preservation after chemotherapy are demonstrated in Figure 1.

Embryo Cryopreservation
The technique which seems to offer the most promise is in vitro fertilization (IVF) with embryo cryopreservation by vitrification.18,36,37 In fact, embryo cryopreservation is the only well-established method of fertility preservation. Ovarian stimulation depends on the time available before the commencement of cancer treatment. If time permits, IVF with gonadotropin stimulation is the best option. 35 In the absence of a male partner, oocyte cryopreservation can be offered. Recent studies have shown that the capacity for fertilization and embryo development of cryopreserved oocytes is similar to fresh oocytes.38–40 Subsequently, these oocytes can be thawed and inseminated with either the partner's sperm or donor sperm.
Oocyte Cryopreservation
When urgent chemotherapy is required or in cases where ovarian stimulation is contraindicated due to high estradiol levels (such as in women with estrogen-receptor positive breast cancer), immature oocytes can be extracted and matured in vitro (IVM).21,37,40–43 The mature oocytes can then be inseminated, and the resultant embryos cryopreserved or vitrified for later use. This technique is still considered experimental.
Ovarian Tissue Cryopreservation
Another investigational option for fertility preservation is cryopreservation of ovarian tissue and reimplantation at a later date.44–48 This requires laparoscopic surgery and removal of either strips of ovarian cortex or the whole ovary for cryopreservation. When fertility is desired and the patient is medically allowed to conceive, it can be transplanted orthotopically to the ovarian fossa or inside the atrophic ovarian cortex. It appears that a combination of ovarian tissue transplantation followed by ovarian stimulation is a viable option. 49 To date, 28 babies have been born after ovarian tissue transplantation into the pelvis. 50 No pregnancy has been reported from heterotopic transplant to the forearm. However, in women with hematological malignancies,51,52 ovarian tissue transplantation may reintroduce malignant cells causing recurrence.
GnRH Agonist
Ovarian suppression with GnRH agonist prior to chemotherapy may reduce the insult to the ovaries. This can be combined with other fertility preservation techniques. The potential benefit of ovarian suppression remains unclear. While an Italian randomized trial 53 suggested a reduction in premature ovarian failure following suppression with GnRH agonist, other studies showed no apparent effect in terms of ovarian reserve (FSH, inhibin) and length of amenorrhea after chemotherapy.54,55
Safety and Risks of Conception after Chemotherapy
Following chemotherapy, women are usually advised to wait between 6 and 12 months before embarking on attempting natural conception. The time interval depends on the type of malignancy (elevated estradiol may stimulate recurrence in some cancers) and the type of chemotherapy. Cytotoxic chemotherapy may potentially cause mutations and oxidative damage to somatic and germ cells raising concerns for possible teratogenicity. However, there is no evidence of such outcomes in humans. An early report 56 showed no significant differences in the rates of cytogenetic syndromes, single-gene defects, or simple malformations in survivors of childhood cancers compared with healthy controls.
A report on reproductive outcome in both male and female cancer survivors showed no differences in miscarriage or live birth rates when evaluated for chemotherapy type and dose. 28 Compared with the children of the survivor's siblings, there was no increase in the rate of genetic or congenital disease in the children of cancer survivors. Similarly, a Dutch study found no increased incidence of Turner's syndrome or Down syndrome in the children of cancer survivors, compared with children of their healthy siblings. 57
Another study of reproductive outcome in survivors of adult cancer found no increase in the rate of congenital malformations compared with that of healthy controls. 58 Meirow et al reported reduced pregnancy rates and increased fetal malformation rates in mice that conceived soon after cyclophosphamide chemotherapy. 24 The rate of teratogenicity was highest immediately after cyclophosphamide and normalized at 12 weeks. They postulated that the effect is worst on the mature oocytes (late pre-antral follicles) at the time of chemotherapy, and the damaged oocytes are lost after a certain amount of time. Another explanation is that the oocytes may have the ability to repair DNA damage. The time frame of 3 weeks in the mouse, which represents follicle growth from primordial follicle to maturity, is equivalent to approximately 6 to 12 months in the human. The authors caution that oocytes up to 12 months following chemotherapy in women may be at a disadvantage.
The potential clinical implication is that a period of contraception after completion of chemotherapy is prudent. It can be followed by attempted natural conception after remission of the disease. However, there will be some women who are unable to conceive spontaneously and need fertility treatment.
Assessment of Fertility after Chemotherapy
Assessment of women after chemotherapy should include a careful history, including menstrual history and reported menopausal symptoms, physical examination, and biochemical and biophysical markers of ovarian reserve. The most important markers appear to be AMH and AFC. The evaluation should also include serum FSH, LH, E2, and Inhibin B.
Fertility Preservation for Women Delaying Pregnancy
Women may be single and not interested in pursuing fertility or may have a partner but not be ready to conceive. In either case, the women (or couple) should be counseled comprehensively and should understand the risk of premature ovarian failure secondary to chemotherapy. A couple should ideally be offered IVF with embryo cryopreservation, with the protocol tailored according to the individual. For example, a survivor of estrogen-receptor positive breast cancer may need to be protected with aromatase inhibitor during ovarian stimulation, reducing a marked elevation in E2. The IVF protocol will also depend on the ovarian reserve and the presence or absence of concurrent male factor infertility.
Single women may be offered ovarian stimulation followed by retrieval and cryopreservation of oocytes. Progress in oocyte vitrification, cryopreservation, and fertilization technique has increased the rates of clinical pregnancy and live births. 59 An alternative for single women is insemination of oocytes with a sperm donor followed by embryo cryopreservation.
Options for Fertility Preservation after Chemotherapy for Women with Ovarian Failure
In some women, ovarian failure after chemotherapy is permanent. This is indicated by amenorrhoea and other evidence of ovarian failure clinically, endocrinologically, and on ultrasound. Here, oocyte donation should be considered. Another alternative is certainly adoption. It is important to be aware that premature ovarian failure is associated with other health problems such as the risk of osteoporosis 60 and cardiovascular disease61,62 and altered psychosexual function.63,64
Psychological Evaluation and Support
Dealing with the diagnosis and prognosis of cancer, the concerns of shortened life expectancy, disability, loss of employment, changes in body image, potential loss of fertility, relationship issues, and possible genetics impairment can be extremely overwhelming. Medical care should include professional counseling. Issues specifically surrounding fertility preservation can be intense and challenging, and the clinicians should ensure that adequate support is available.
Conclusion
Young women dealing with malignancy may have an easier psychological recovery with the hope and prospect of having a biological child. With time, the option of fertility preservation will become better established, and concrete data will be available to assist women in making the best informed decision regarding future fertility. It is important that a woman's care should involve a multidisciplinary team including oncologist, reproductive endocrinologist, psychologist, and other health care professionals.
Ideally, fertility preservation techniques should be initiated prior to commencing chemotherapy. If this is not feasible, many options exist following the completion of chemotherapy. Despite potential damage to ovarian reserve, natural or assisted fertility is still possible. The window of potential teratogenicity appears to be 6 to 12 months after the completion of chemotherapy. Knowledge of ovarian reserve specific to age and chemotherapy protocol and dose can help guide women and couples to make the best choice regarding the timing and choice of fertility preservation technique.
Author Contributions
JHH wrote the first draft of manuscript under the supervision of TT. Both JHH and TT played a role in preparation and finalizing the manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
JHH has no conflict interest. TT is an advisor for Watson Pharma and one of the investigators for HALT Medical.
Dsiclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests. Provenance: the authors were invited to submit this paper.