
Abstract
Objectives:
Our review aimed to consolidate the latest update on the application of in vitro maturation among immature oocyte harvest in combination with ovarian tissue cryopreservation known as ovarian tissue oocyte–in vitro maturation.
Methods:
A thorough search for relevant studies was conducted via PubMed, Google Scholar, EMBASE, and clinical.gov databases up to December 2020. The primary outcome was the oocyte maturation rate, which measured the number of immature oocytes (geminal vesicle stage) that progressed to mature oocytes (meiosis II stage) following in vitro maturation. The secondary outcomes were the fertilization rate following intracytoplasmic sperm injection/in vitro fertilization of these oocytes for the embryo cryopreservation cohort. Our review included pre-pubertal girls and women with cancer who underwent ovarian tissue oocyte–in vitro maturation as fertility preservation.
Results:
The primary search identified 207 studies. Twelve manuscripts were selected for inclusion in our review following duplication assessment, title and abstract screening, and full-text evaluation tailored to our inclusion criteria. All the population belonged to a cancer group and underwent concurrent ovarian tissue oocyte–in vitro maturation. A total of 5724 immature oocytes were obtained following ovarian tissue cryopreservation. Approximately 33.84% of the immature oocytes successfully matured via in vitro maturation, which were cryopreserved as oocytes or fertilized as embryos and subsequently stored for future use.
Conclusion:
Our review proposed the potential application of ovarian tissue oocyte–in vitro maturation in increasing the number of mature oocytes. The acceptable improvement in oocyte maturation rate following in vitro maturation indicates that improving oocyte outcomes is an excellent cost-effective strategy for fertility preservation among women with cancer.
Keywords
Introduction
Immature oocytes at the geminal vesicle (GV) stage are considered rested at the first meiotic prophase with a large nucleus. These oocytes are often discarded together with meiosis I (MI) oocytes as incomplete GV breakdown leads to maturation arrest without polar body production, which is not fertilizable. This oocyte stage is often discovered during control ovarian stimulation in standard in vitro fertilization (IVF) because of the asynchronized development of follicles, which leads to high cycle cancelation.1–3 Most cases are observed among women with polycystic ovary syndrome (PCOS), as the standard stimulation is modified to reduce the risk of hyperstimulation syndrome, which resulted in a high number of immature oocytes.4–6 In addition, the current implementation of fertility preservation (FP) among the cancer population leads to immature oocytes. To date, oocyte cryopreservation (OC) and ovarian tissue cryopreservation (OTC) are recommended for pre-pubertal girls and women before primary cancer treatment. Traditionally, OC is initiated during the follicular phase (FPh) following menstrual cycles to obtain a high number of meiosis II (MII) oocytes for cryopreservation. However, for FP purposes, most patients required immediate stimulation to avoid delay in initiating chemotherapy. Therefore, a random-start (RS) regime must be implemented in this case. Nevertheless, the RS stimulation often results in immature oocytes.2,4,5,7–10 Previously, GV and MI oocytes were discarded, as they could not be cryopreserved. The finding leads to a less favorable outcome among the cancer population; thus, cycle repetition is proposed to overcome this problem. The implementation of in vitro maturation (IVM) in OC procedure does improve the overall number of mature oocytes and their ability to be cryopreserved. The IVM of oocytes was first reported in 1935 by Pincus and Enzmann.11,12 They observed the spontaneous nature of the meiosis of rabbit ova removed from antral follicles. Four years later, Pincus and Saunders further consolidated the evidence using human oocytes.11–13 Subsequently, IVM was developed, and it became an essential intervention in the veterinary field to breed rare and distinct species. Edward RG et al. had developed the IVM concept in maturating human oocytes since 1965, which led to the first IVM baby in 1991.14,15 Since then, IVM had been implemented in improving infertility treatment and FP. At present, IVM is being used as a routine procedure in many centers with many live births reported worldwide.
On the contrary, OTC is recommended for pre-pubertal girls with cancer worldwide. It is also been a good option among women with cancer who have limited timing frame for oocyte stimulation prior to chemotherapy. In addition, this procedure is established following ovarian tissue transplantation. To date, at least 60 live births are reported worldwide. Similarly, many immature oocytes are harvested during ovarian cortical dissection for tissue cryopreservation. Previously, these oocytes are discarded, and only tissue cryopreservation is performed. Conversely, the debate regarding the risk of minimal residual disease (MRD) following ovarian tissue transplantation, particularly in hematological cancer, initiates the urge of utilizing these immature oocytes obtained during OTC as a safe gamete source for future fertility use, as the risk of MRD is eliminated.
Therefore, based on the successful outcome in OC following IVM, the idea of combining IVM following OTO (ovarian tissue oocyte–in vitro maturation) 16 has received considerable attention to improve the outcome of FP.2,8,17 In this procedure, the immature oocytes collected during the OTC can mature via IVM and subsequently cryopreserved together with ovarian tissue. This method allows double utilization of FP methods, namely, OC and OTC, to improve FP among pre-pubertal girls and women. At present, the implementation of OTO-IVM has been widely proposed. Despite emerging evidence regarding OTO-IVM, this method remains unclear, as it is still considered at the initial stage of implementation.
Hence, our review aimed to summarize the current knowledge on OTO-IVM and consolidate the evidence of such use. In this review, we evaluated the number of immature oocytes yielded following OTC and the oocyte maturation rate (OMR) following IVM use and fertilization rates among post-IVM oocytes used in intracytoplasmic sperm injection (ICSI)/IVF. This finding can be used to strengthen the current evidence in establishing the recommendation of OTO-IVM in FP settings.
Methods
Protocol registration and search strategy
Our manuscript was formulated on the basis of the recommendation by Preferred Reporting Items for Systemic Reviews and was registered under Prospective International Register of Systematic Reviews (register no. CRD42021253406).18,19 The ethical approval for systematic review (SR) is not required. Relevant studies within 20 years (2000–2020) were thoroughly searched in October 2021. The keywords used in PubMed search were as follows: “in vitro oocyte maturation techniques” [MeSH Terms] OR “vitro” [All Fields] AND “oocyte” [All Fields] AND “maturation” [All Fields] AND “techniques” [All Fields] OR “in vitro oocyte maturation techniques” [All Fields] OR “in vitro oocyte maturation techniques” [MeSH Terms] OR “vitro” [All Fields] AND “oocyte” [All Fields] AND “maturation” [All Fields] AND “techniques” [All Fields] OR “in vitro oocyte maturation techniques” [All Fields] OR “oocyte” [All Fields] AND “vitro” [All Fields] AND “maturation” [All Fields]. For Google Scholar search, “in vitro maturation ovarian tissue” OR “in vitro maturation ovarian tissue cryopreservation” was used as keywords. Subsequently, the keywords “IVM,” “OTC,” “immature oocytes,” “ovarian tissue cryopreservation,” “oocyte cryopreservation,” and “in vitro maturation” were used for clinical.gov database search, and the keywords “ovarian tissue cryopreservation” and “in vitro maturation” were used for EMBASE database search. The references of the selected studies were also collected, and all studies were subjected to duplication evaluation using EndNote® version 20.0.1. We also improved our search for potential manuscripts by performing a manual search using the reference lists obtained from related articles.
Study selection, data extraction, and risk of bias assessment
Following the primary search, the titles and abstract of manuscripts were initially evaluated by three authors (A.M.F, Y.S., and S.T.). The inclusion criteria were as follows: English language, original articles from January 2000 to December 2020, IVM as intervention following OTC in women with cancer for FP, and OMR as the primary outcome. The selected articles were subjected to full-text screening. Review articles, case reports, studies that describe OTC procedure without IVM, and non-English manuscripts were excluded. Subsequently, all the manuscripts were reviewed independently. The included manuscripts described the type of study, participant cohort, and number of immature and successfully matured oocytes following IVM and used OMR as an outcome. Any conflicts among the authors were resolved through discussion and another opinion by the fourth author (N.S). The National Institutes of Health (NIH) tool for observational studies was used for quality assessment. 20 The evaluation was further conducted by rating each of the 14 variables as 1 for “yes” and 0 for “no” or “non-applicable (NA).” The studies were further categorized as poor (0–5), fair (6–9), or good (10–14) based on the total score. All data from the included studies were tabulated accordingly (Table 1). All the included studies in our review obtained a minimum fair score (Table 2). The data were extracted on the basis of author’s last name, year of publication, number, type of cohort, age of participants, mean oocytes retrieved from each patient, number of immature and mature oocytes following IVM, the ability of oocytes to be cryopreserved, and the mean OMR of each study as the primary outcome. In addition, the fertilization rate, pregnancy rate, biochemical pregnancy, clinical pregnancy, and live birth were recorded as the secondary outcomes if available.
Summary of the results from 21 included articles identified in a systematic review of the literature.

IVM: in vitro maturation; OC: oocyte cryopreservation; NS: non-stimulated; OTC: ovarian tissue cryopreservation; IVF: in vitro fertilization.
Mean number of oocytes retrieved.

IVM: in vitro maturation.
Results
About 207 studies were discovered in the primary search (Figure 1), and 48 articles were discarded after duplication evaluation via EndNote®. The titles and abstracts of the remaining 159 articles were screened independently in accordance with the inclusion criteria. Subsequently, 128 articles were excluded, and 31 articles proceeded with the full-text evaluation. A total of 19 articles were further excluded; nine were not suitable, and 10 had no full text available (poster presentation or proceedings). Finally, 12 relevant articles were compiled for this review. The selected articles were critically evaluated for quality and bias as described in the Methodology (Supplementation 1).
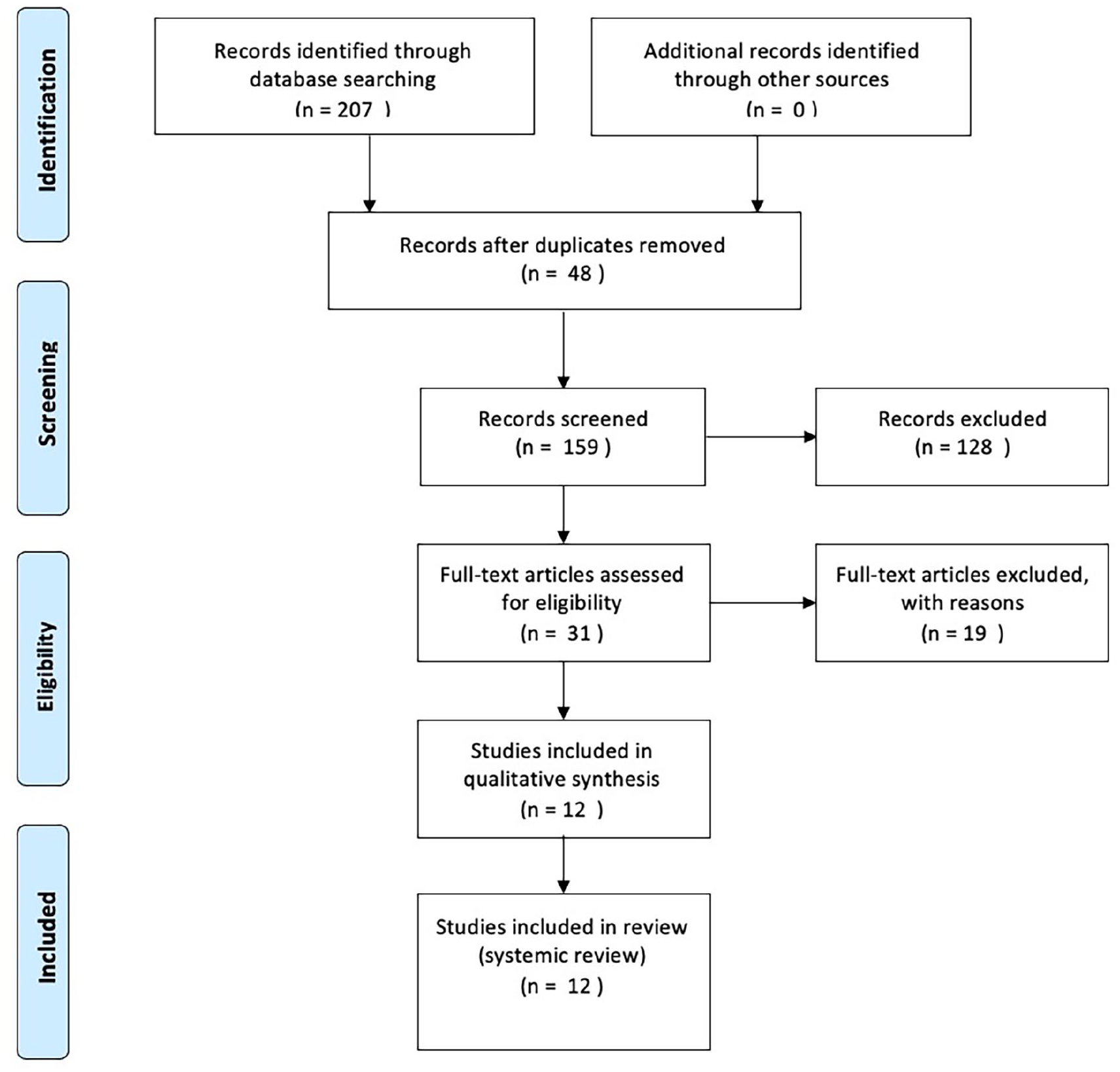
PRISMA flow chart of searching strategy.20
Demographic profile of included studies
Based on the included studies, 590 patients with cancer received concurrent OTC as part of FP treatment.21–32 At least 7.12% (n = 42) of patients were pre-pubertal (less than 12 years old), whereas 92.88% (n = 548) of patients were post-pubertal. The mean age in the pre- and post-pubertal groups was 7.04 and 25.15 years, and the youngest patient was 3.66 years old. In our review, almost all OTCs were performed via unilateral oophorectomy or wedge resection of the ovarian cortex, except for one patient who underwent bilateral oophorectomy for risk reduction surgery for BRCA1 mutation. 30 In addition, in one study, OTC was performed after oocyte retrieval following stimulated cycles (ST). 28 Otherwise, all other OTCs were performed in non-stimulated (NS) ovaries. All included studies utilized single-cycle IVM, except for one study that performed two cycles of IVM (one was conducted during the FPh, and the second was concurrent with the IVM procedure). 28 The summaries of the included studies are tabulated in Table 1.
Primary outcome
A total of 5724 oocytes were retrieved in includes studies with concurrent OTC. The mean oocyte retrieval was 11.27 oocytes for each patient. Following IVM, 1937 oocytes reached MII with OMR of 33.84%. Afterward, 1169 oocytes were successfully cryopreserved (Table 2).
Secondary outcome
About 118 embryos were obtained following IVF/ICSI with 64.53% of mean fertilization rate in post-IVM oocytes. All embryos were cryopreserved. In addition, no record of pregnancy rates and biochemical, clinical, and live birth was found, as all of our studies included utilized FP (Table 3).
The secondary outcome of fertilization rates following IVM.

OC: oocyte cryopreservation.
Discussion
This review found that OTO-IVM could improve FP treatment outcome among cancer population. Following IVM, the OMR affects the number of mature oocytes that can be either directly cryopreserved or utilized via ICSI/IVF for embryo cryopreservation. Otherwise, most of the included studies in our review show that the OMR following IVM is at least 30%. Although in this review, the OMR is lower compared with the conventional IVM, it is immature because of the oocytes retrieved during OTC; follicles with a size of at least 5–10 mm represent class 3–5, whereas those with a size of 12–14 mm indicate class 6–7 in conventional IVM. The classes of oocytes had been established since 1986. The pre-antral follicle starting from 0.1 mm to ovulation follicle size of 20 mm indicates the class of oocyte maturation, in which the smaller follicle size indicates the lower class of oocytes, thereby representing the most immature stage of oocytes. 33
Most IVM is used in NS cycles to tailor women with a higher risk of ovarian hyperstimulation syndrome (OHSS), such as those with PCOS. Early oocyte pick-up (OPU) in an ST cycle or before the growth of dominant follicles in NS follicles is recommended for this group of women. The idea of NS cycles was initiated by Cha et al. 14 in 1991, who successfully delivered triplets using NS oocyte donation. Subsequently, this strategy was expanded and combined with IVM, which led to a better outcome of using immature oocytes. In addition, IVM in an NS cycle has been proposed in cancer cases where stimulation is not permissible. 13 Therefore, in this cohort of patients, the cycles should be repeated to increase the number of oocytes within the same menstrual cycle. 34 However, the risk of failed oocyte maturation after 48 h of IVM culture is considered as a risk in NS cycles, which lead to low embryo yield with difficulty in recovering immature oocytes in follicles that are less than 9 mm. 35 Furthermore, this technical issue did not interfere with OTO-IVM.
During the standard OTC, most oocytes are harvested during medulla scrapping while processing the cortex layer to obtain at least 1–2 mm thickening, and all visible follicles can be aspirated directly prior to scrapping. The maturation of these oocytes will be assessed following IVM culture (Figure 2). As established, the size of follicles affects the classes of oocytes and their stage. However, the use of follicle size to predict the presence of oocytes remains unknown. Some aspirated follicles do not contain any oocytes upon examination under a microscope. The available evidence indicates that oocytes can be obtained in follicles that are more than 6 mm, and maturation is acceptable after 48 h regardless of the menstrual cycle phase during OTC. 21 Thus, follicle size should be observed during OTC and aspirated before tissue processing, or oocytes can be collected at the end of tissue processing. Then, these oocytes should be cultured with IVM as OTO-IVM.

(a) OTC standard protocol—dissection of ovarian tissue fragment 1 cm3 for cryopreservation. (b) Aspiration of visible follicles with needle or using scalpel to harvest possible oocytes before ovarian cortex dissection. (c) Immature oocytes (GV) harvest cultured with IVM media aiming for maturation (MII); at least 24–48 h as oocytes from OTC usually class 4–5 thus required longer IVM culture hours as compared to standard IVM. (d) Matured oocytes (MII) will be cryopreserved and use in future for IVF/ICSI.
On the contrary, the ovarian tissue will be transported to the embryology lab for processing during the standard OTC procedure. Some literature shows that the risk of acute ischemia during this critical period can lead to oocyte degeneration; however, most of this evidence is obtained from animal studies.36,37 Acute ischemia may be due to sudden loss of blood supply during oophorectomy and temperature changes during storage while transporting the tissue to embryology lab for OTC. In regard to the duration of oocyte maturation, our review revealed that although oocyte maturation is better in a shorter time, prolonged culture up to 48 h is acceptable, as it helps in yielding mature oocytes following the IVM culture.22,38 The oocyte maturation outcomes either within less than 48 h or within 48 h are comparable. Thus, the proposed OTO-IVM environment with culture up to 48 h is acceptable to ensure that good numbers of mature oocytes are obtained following OTO-IVM. 38
Using OC alone for FP, most OPUs are scheduled in an ad hoc basis without proper stimulation to cater to the limited period of FP treatment. Therefore, most patients undergo OPU following RS protocol regardless of the ovarian phase. Although it requires a higher dose of gonadotropin, the outcome of the luteal phase (LP) OPU is comparable to that of FPh, which is considered as the gold standard. 39 Regarding OTO-IVM, our review found that although LP OTO-IVM yields a lower number of oocytes than FPh OTO-IVM, the OMR and fertilization rates are comparable, although no stimulation is needed for this procedure. 28 Follicle development was better in the FPh, as an adequate amount of follicle-stimulating hormone and estradiol are present. Moreover, the production of these hormones is dormant in the LP because of the high level of progesterone. 40 However, this phenomenon was different as earlier evidence showed that possible mature oocytes could be harvested in LP OTO-IVM. 41 Previously, Hwang et al. 42 reported pregnancy after utilizing oocytes donated by a woman during her cesarean section. Since then, more evidence was gathered to consolidate that LP oocytes can be harvested and utilized. The anovulatory follicle theory within the LP postulates that certain follicles are developed until the late antral stage despite the high luteinizing hormone and progesterone levels. 43 In addition, priming with human chorionic gonadotropin can improve the maturation of FPh oocytes, but its role in small follicles in the LP is limited, which needs to be explored. Nonetheless, the maturation of oocytes with or without priming has acceptable fertilization rates. 44
Following OTO-IVM, the ability of post-IVM oocytes during OTC to form euploid blastocyst remains unclear, although live births are reported worldwide. 45 As established, the intracellular maturation of oocytes is complex, and it depends on various regulators, including growth factors, gonadotropins, steroid, and sterols. Delineating the complex interaction between these positive and negative components is critical for determining the role that oocyte maturation plays in regulating follicle development and ovulation, which may lead to novel methods that can be used to modulate these processes in women with normal and aberrant fertility. In addition, the epidermal growth factor (EGF) is dependent on these hormones to produce essential proteins that balance the oocyte microenvironment. 46 An alteration of this condition leads to the non-synchronization of EGF network ligands and affects the overall quality of the oocytes. Thus, the oocyte maturation in the nucleus and cytoplasm must be archived. 47
Given this complex mechanism, a possibly high developmental failure may be observed in post-IVM oocytes following ICSI/IVF. Most of the evidence highlights the occurrence of nuclear asynchrony and DNA fragmentation caused by inadequate culture duration, which interferes with oocyte competence and consequently leads to implantation failure and abortion.46,47 However, these phenomena were also observed in non-IVM oocytes through the recent development of artificial intelligence with the combination of time-lapsed monitoring. This finding indicates that both oocytes, with or without IVM, are susceptible to developmental failure probably because of genetic factors rather than culture issue. Kirillova et al. 48 reported a euploid blastocyst formation following ICSI from oocytes obtained following OTO-IVM, leading to a better predictive of quality blastocyst following OTO-IVM. Her team then proposes the use of the biphasic IVM system for OTO-IVM. It portrays reasonable maturation rates following OTO-IVM compared with standard IVM, as it improves the molecular problems aiming at synchronizing nuclear and cytoplasmic maturation. 49 Thus, extrapolating from this evidence, the OTO-IVM can be implemented, as the current pregnancy rates following conventional IVM are reported to be up to 30%–40%. 45
Limitation
Our review is limited to the role of OTO-IVM. Although our data quality is good based on NIH tool scoring (Table 1), the IVM medium component was not explored in detail. The adjunct medium or hormone added to enhance IVM outcome (e.g. growth hormone) and the different techniques of oocytes following OTC were not discussed. Theoretically, additional hormone in different types or media influences the OMR, which needs to be further explored. Otherwise, the participants in this review are mostly post-pubertal; thus, evidence for the pre-pubertal group is limited. Finally, no clinical pregnancy rates are reported in this review, as in the oocytes and embryos were not utilized in this cancer cohorts.
Conclusion
Our findings indicate that OTO-IVM can increase the number of mature (MII) oocytes following OTC, and subsequently improve the FP strategy. Furthermore, OTO-IVM can be performed even without any stimulation and regardless of the menstrual phase, as the follicles size does not interfere with the number of oocyte yield, OMR, and fertilization rates. Nevertheless, the careful selection of patients with adequate culture time is essential. In the future, elucidating the microenvironment in post-IVM oocyte harvest during OTO-IVM can be explored to determine the molecular basis of competent oocytes following IVM and to improve assisted reproductive technology.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221114269 – Supplemental material for Twenty-first century oocyte cryopreservation—in vitro maturation of immature oocytes from ovarian tissue cryopreservation in cancer patients: A systematic review
Supplemental material, sj-docx-1-whe-10.1177_17455057221114269 for Twenty-first century oocyte cryopreservation—in vitro maturation of immature oocytes from ovarian tissue cryopreservation in cancer patients: A systematic review by Ahmad Mohd Faizal, Yodo Sugishita, Yuki Suzuki-Takahashi, Hideyuki Iwahata, Seido Takae, Yuki Horage-Okutsu and Nao Suzuki in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.