
Abstract
Objective
The aim of this study was to explore variables associated with poor recovery from depression.
Method
A sample of depressive patients (n = 121) referred to treatment was followed prospectively for 6 years. Clinical evaluations were done at baseline and at 6 month, 1, 2 and 6 years study visits. A diagnosis of major depression based on SCID interview at 6 year and high BDI score along follow-up indicated poor recovery. A diagnosis of full remission at 6 year and low BDI score during follow-up indicated good recovery.
Results
Chronic depression was found in 15% of patients. A repeated measures analysis of variance of HDRS-, SCL-90, hopelessness (HS) and Social and Occupational Functioning Assessment Scale (SOFAS) scores showed that those with poor recovery had recovered poorly also according these scales during the whole follow-up. Treatment factors did not associate with recovery. Logistic regression analyses revealed an independent association between poor recovery at 6 year and both high HS- and low SOFAS scores at 12 months, 24 months and 6 year assessments.
Conclusions
Assessment of hopelessness and social and occupational functioning help to early identify high-risk patients who would be in need for more individually tailored treatments.
Introduction
The trajectory of major depression (MDD) is characterized by recovery from the initial episode with subsequent recurrences [1]. It is well known that recurrent depression predicts risk for subsequent depression episodes. Full remission is the aim of treatment of depression. It is also clearly associated with better long-term prognosis than partial remission [2, 3].
There is growing body of evidence that unipolar depression could be viewed as a chronic illness with multiple phases rather than as a relapsing-remitting disorder [4–6]. Our previous follow-up study on general population found that 65% of depressive subjects were still depressed after two years. The severity of baseline depressive symptoms associated with failure to recover [7].
Knowledge of clinically valuable long-term predictors of poor recovery of MDD is limited. Keller et al. [8] found that 12% of MDD patients remained chronically ill after 5 years. Their longer follow-up [9] revealed further that 38% of chronically ill patients recovered within the next 5 years. Only the length of illness prior to intake characterized chronic MDD. In a 15 years follow-up of major depression patients [10] an association between psychosocial impairment and recurrence of major depression was found. Authors concluded that the evaluation of psychosocial impairment may help to identify patients who are at increased risk of recurrence.
Depressed patients are often undertreated by both psychiatrists and primary care physicians [9, 11]. This is unfortunate, since Akerblad et al. [12] showed that patients' adherence to antidepressant treatment showed superior long-term recovery as compared to non-adherent patients in a 2 year follow-up.
Factors related to recovery of depression have been studied in short follow-ups. A six months cohort study [13] of depressed outpatients found that early response strongly associated with the outcome of the treatment but characteristics or comorbidity of depression did not. In other short-term clinical follow-up studies several risk factors have been identified to associate with poor recovery from major depression such as higher age, low income, long duration of depressive symptoms prior to treatment, high symptom severity, loss events, neuroticism, hospital admission and comorbidity [11]. Identifying variables of poor prognosis is vital to treatment development [14]. It is clinically important to distinguish patients with poor prognosis as early as possible because these patients present a remarkable public health problem.
The first aim of this study was to explore the course of depression. Secondly, we tried to find clinically useful tools to predict the poor outcome of depression and thus to identify those patients who might need a special attention.
Materials and Methods
The clinical arm of the observational Kuopio Depression study (KUDEP) at Kuopio University Hospital consisted of 175 treatment- seeking outpatients with depression based on ICD-10 diagnostics. Patients (n = 4) were excluded if they had previously been diagnosed as suffering from a central nervous disease, a severe physical disease (recent myocardial infarction, sequelae of stroke etc.), alcohol or drug dependence, a marked deficiency in cognitive capacity, or any other serious mental disorder such as schizophrenia or other psychosis. During the 6-years follow-up period (1/1996-1/2004), 43 (25%) patients withdrew from the study or their follow-up was incomplete and seven died leaving 121 study subjects in the final 6-years follow-up sample. Approval to conduct the study was obtained from the Ethics Committee of Kuopio University Hospital and the University of Kuopio. All patients gave their written informed consent before entering the study.
At baseline, patients completed questionnaires relating to their socio-demographic background and duration of depressive symptoms (see Table 1). The following variables were used in this study: age, sex, marital status (married or co-habiting/other), length of education and duration of depressive symptoms.
Characteristics of the study population according to the status of depression at 6 year follow-up.
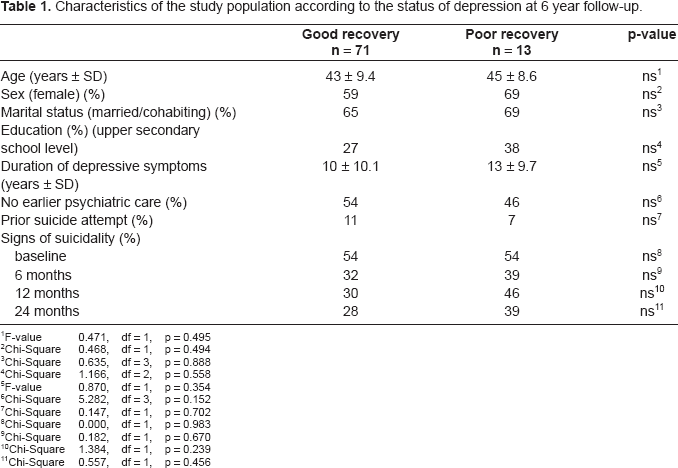
F-value 0.471, df = 1, p = 0.495
Chi-Square 0.468, df = 1, p = 0.494
Chi-Square 0.635, df = 3, p = 0.888
Chi-Square 1.166, df = 2, p = 0.558
F-value 0.870, df = 1, p = 0.354
Chi-Square 5.282, df = 3, p = 0.152
Chi-Square 0.147, df = 1, p = 0.702
Chi-Square 0.000, df = 1, p = 0.983
Chi-Square 0.182, df = 1, p = 0.670
Chi-Square 1.384, df = 1, p = 0.239
Chi-Square 0.557, df = 1, p = 0.456
The severity of depression was assessed using the 21-item Beck Depression Inventory (BDI) (range 0–63) [15]. One of the BDI items relates to self-destructiveness. The response alternatives “I have definitive plans to commit suicide”, “I would kill myself if I had the chance” and “I feel I would be better off dead” indicated signs of suicidality [16]. Previous suicide attempts were asked.
The level of depression in each patient was also assessed separately by the investigator on the basis of the Hamilton Depression Rating Scale, HDRS (range 0–52) [17]. A physician assessed the level of psychosocial functioning of the patients at baseline and the investigator on later follow-ups using to the Global Assessment of Functioning (GAF) scale (range 1–100) [18]. Social and occupational functioning was assessed by the investigator with Social and Occupational Functioning Assessment Scale (SOFAS, range 1–100). The SOFAS focuses on the individual's level of social and occupational functioning while excluding severity of symptoms [19].
The level of hopelessness was assessed by using the Beck Hopelessness Scale (HS) which is a 20-item, self-administered rating scale designed to measure negative expectancies concerning one's future life. Total HS score ranges from 0 to 20 with increasing hopelessness with increasing scores [20]. The Symptom Check List 90 (SCL-90) total score (Global Severity Index, GSI, range 1–5) was used to provide an accurate measure of psychopathology [21, 22]. All the psychometric scales used in this study are well-known and widely used instruments with adequate validity. In this study sample, Crohnbach's alphas were: BDI 0.87, HDRS 0.76, HS 0.84, SCL-90 0.96.
Data relating to treatment during follow-up were collected from patient case records and from interviews with the patients. Thus, treatment was recorded but not controlled. Antidepressant drug therapy was considered to have been adequate if the duration of treatment had exceeded 3 months during the 6 months of follow-up and 6 months during the 12-months follow-up period, and if the daily dose had fallen within a range deemed effective (e.g. minimum daily dose of tricyclics 150 mg of citalopram/fluoxetine/paroxetine 20 mg) [23]. The duration of continuous adequate antidepressant drug treatment (months) was calculated according to principles described above. Finally, we recorded total duration of psychiatric treatment. The treatment situation at 6 year was recorded.
At the end of the 6 years follow-up psychiatric diagnoses were confirmed by means of the Structured Clinical Interview for DSM-III-R (SCID I) [24]. This was performed by the experienced interviewer who had undergone a training course prior to the study, and who had achieved a total kappa of 0.78 against a trainer experienced in SCID I diagnoses. All interviews were carried out blind with the interviewer unaware of the results of concurrent self-report questionnaires.
In order to assess reliably risk factors for poor recovery we included for further analysis all who at 6-years follow-up were fully recovered from major depression (code numbers of DSM-III-R diagnoses 296.26, 296.36; Major depression, single episode or recurrent in full remission, n = 71) and all who showed poor recovery from major depression (296.21–296.24 and 296.34; Major depression, single episode (mild, moderate or severe with or without psychotic features) or major depression, recurrent n = 13). Additionally, it was also required [25] that at 6, 12 and 24 months assessment the mean of the BDI-score must be repeatedly ≥ 14 in the poor recovery (PR) group and <14 in the good recovery (GR) group (6 mo: PR 15.5 vs GR 13.2, 12 mo: 16.8 vs 11.8, 24 mo: 14.5 vs 10.9). Those (n = 37) whose depression was fluctuating during the follow-up and, thus, did not fulfil these criteria, were excluded.
The patients with poor or good recovery were compared using chi-squared analysis for categorical variables and with two-tailed analysis of variance (ANOVA) for continuous variables. The repeated measures analysis of variance including grouping variable was used to analyze the differences in clinical scale scores over time. The normal distribution of variables and residuals (standardised and unstandardised) was verified in each analysis of variance. The logistic regression models were used to calculate age- and sex-adjusted odds ratios (OR) with 95% confidence intervals (CI) for factors independently associated with poor recovery.
Results
Out of the patients 15% recovered poorly. The patients with poor recovery did not differ from the others with regard to age, sex, education, marital status, duration of depressive symptoms, prior suicide attempt, or suicidal features during follow-up (Table 1). There was no difference between the groups in treatment received during the follow-up (Table 2).
Treatment received during follow-up.
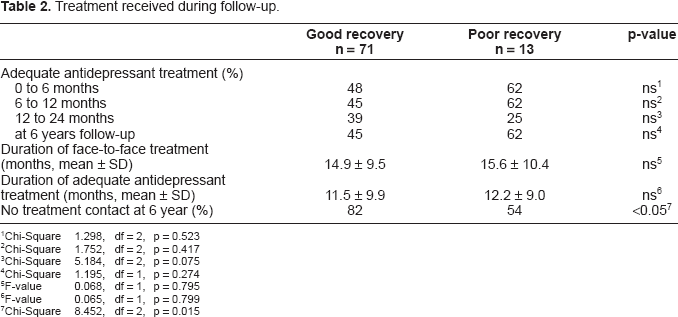
Chi-Square 1.298, df = 2, p = 0.523
Chi-Square 1.752, df = 2, p = 0.417
Chi-Square 5.184, df = 2, p = 0.075
Chi-Square 1.195, df = 1, p = 0.274
F-value 0.068, df = 1, p = 0.795
F-value 0.065, df = 1, p = 0.799
Chi-Square 8.452, df = 2, p = 0.015
The patients with poor recovery had statistically higher HS scores at 12 and 24 months assessment, while SOFAS scores differed statistically significantly between the groups at baseline, at 12 and 24 months. At 6 years follow-up the patients with poor recovery were more symptomatic than others in all outcome measures (Table 3).
Clinical outcome during follow-up in good (GR) and poor recovery (PR) group.
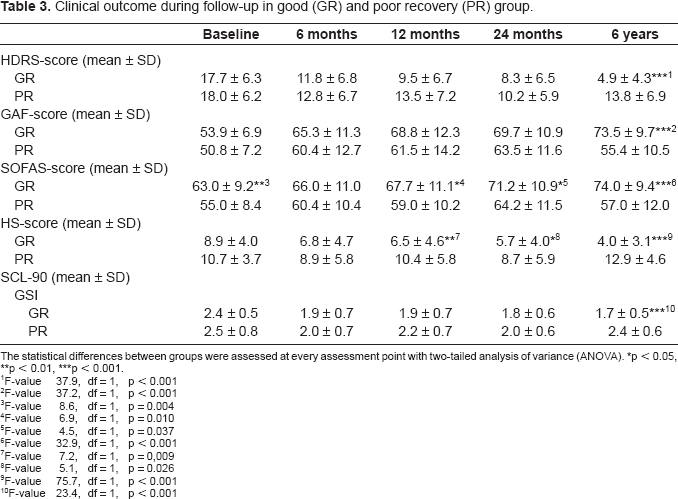
The statistical differences between groups were assessed at every assessment point with two-tailed analysis of variance (ANOVA).
p < 0.05
p < 0.01
p < 0.001.
F-value 37.9, df = 1, p < 0.001
F-value 37.2, df = 1, p < 0.001
F-value 8.6, df = 1, p = 0.004
F-value 6.9, df = 1, p = 0.010
F-value 4.5, df = 1, p = 0.037
F-value 32.9, df = 1, p < 0.001
F-value 7.2, df = 1, p = 0,009
F-value 5.1, df = 1, p = 0.026
F-value 75.7, df = 1, p < 0.001
F-value 23.4, df = 1, p < 0.001
Repeated measures analysis of variance (Table 3) showed a significant decreasing linear trend in HDRS [(F(4, 328) = 5.4), p < 0.001], GAF [F(3.5, 279.2) = 6.1, p < 0.001], SOFAS [F(4, 316) = 4.3, p < 0.01] and SCL-90 [F(3.3, 267.2) = 6.6, p < 0.001], HS [F(4, 308) = 6.7, p < 0.001] and scores during the five study phases. Significant interaction between follow-up time and recovery groups were seen in all scales. Results of these scales showed that patients in poor recovery group had recovered less well from their symptoms during the whole follow-up than patients with good recovery.
The statistically significant results of statistical analyses (Tables 1–3) were used to select variables for logistic models assessing poor recovery. Several separate logistic regression analyses showed that high HS-score at 12 month associated positively with poor recovery (OR 1.28, 95% CI 1.08–1.52, p = 0.004). Significant association was also found with high HS-scores at 24 month (OR 1.19, 95% CI 1.02–1.39, p = 0.025), and at 6 year follow-ups (OR 1.70, 95% CI 1.28–2.25, p < 0.001) and poor recovery. High SOFAS -score at 12 month associated negatively with poor recovery at 6 year (OR 0.90, 95% CI 0.84–0.98, p = 0.009). Further, the statistically significant association was found between SOFAS-score at 24 month (OR 0.93, 95% CI 0.87–0.99, p = 0.024) and at 6 year (OR 0.85, 95% CI 0.77–0.93, p < 0.001), and poor recovery. All the models were adjusted with age, sex and length of treatment.
Discussion
We found out that 15% of the patients had chronic course of depression. Keller et al. [8] reported earlier that 12% of MDD patient remained chronically ill in a 5 year follow-up. Kennedy et al. [6] reported that during 10-year follow-up 18% of originally psychiatric inpatients with severe depression never achieved full asymptomatic status for even a month. Our results are in accordance with these earlier reports. This study revealed that the high HS—and low SOFAS- scores during follow-up were associated independently with poor recovery.
Since hopelessness and psychosocial functioning give valuable information about patients' depression and its consequences, their assessment could be considered in ordinary clinical practice. This might help to find out patients with possible poor outcome. The ability to identify high-risk subjects for whom an appropriate intervention can be designed [14] is crucial for better long-term outcome in treatment of major depression.
The mean HS-score of Finnish general population (mean 3.9) parallels that of our patients in good recovery group while among those with poor recovery the hopelessness was more prominent. In Finnish general population HS-score was found to be dynamic independent concept not related only to depression [26]. Furthermore, hopelessness predicted suicide in 10-year follow-up [27]. Thus it should be investigated how hopelessness among depression patients could be alleviated.
A recent review [7] highlighted the need of research on long-term social functioning in major depression. It was also concluded that social functioning may change many times over long follow-up and therefore there is need to use longitudinal instruments. We used cross-sectionally assessed SOFAS-scores which associated in logistic regression analyses with poor recovery. This parallels with Kennedy's and coworkers [5] conclusion that long-term impairment in social functioning is often associated with non-remission of depression. Furthermore, in one study SOFAS scores on admission of psychiatric inpatients [28] correlated negatively with duration of hospital stay and SOFAS on discharge negatively with psychiatric 2-year outcome. Assessing the social-occupational area in depressed patients may enable to start and focus corrective strategies as early as possible in order to prevent long term poor recovery and functioning.
No associations between treatment variables and the outcome of the treatment were found. However, special interventions might benefit depressed patients with high level of hopelessness and low level of psychosocial functioning. We are aware that in an observational study, the causal relationship between intensity of treatment and outcome can not be studied reliably. Also quality of face-to-face relationships could not be monitored. The mean duration of face-to-face treatment period was near to 15 months. Again, its length did not associate with recovery. The possible benefits of drug treatment were not fully utilized. Still, further alleviation of symptoms was possible after active treatment was discontinued for some, but for those with poor recovery this was not so favourable. They might have benefited from more active and individually tailored treatment and from possibility of longer treatment.
The sample size of our study was quite small which is a limitation. Therefore, we could not completely exclude the possibility of a type 2 statistical error. The follow-up time was long which can be considered as a strength. We reported earlier [29] that in this sample somatic comorbidity has only minor effect on alleviation of depressive symptoms in a 6-month follow-up and therefore this variable was not analyzed. Our sample was clinically complex because the mean duration of depressive symptoms prior to treatment was long. About the half of patients had received earlier psychiatric care. Thus, our results can not be generalized to patients with the first major depression episode. Our results are useful in special health care where more chronic and complicated patients are treated. The assessment of recovery was based on the results of diagnostics at 6 years follow-up as well as on the BDI scores along the follow-up. Depressive symptoms are fluctuating and therefore more frequent assessments of depressive symptoms or longitudinal interviewing would have been methodologically better.
Taken together, the assessment of hopelessness and social functioning is important in depressed patients. Paying attention on them in admission and during treatment may promote recovery from depression.