
Abstract
Duplications of the alimentary tract are very rare. A one-month-old female presented with symptoms of anorexia, vomiting and continuous watery diarrhea. The plain abdominal radiograph showed thickened intestinal wall and signs of small bowel obstruction. The fevers, vomiting, and continuous wartery diarrhea persisted despite antibiotics, and worsened. The patient failed to respond to medical managements, 27 hours after admission, the patient died due to multiple organ failures. The autopsy was performed, small bowel obstruction due to an ileocecal duplication cyst (3 × 3 cm) was recognized. The ileocecal duplication cyst was attached to the ileum which was changed edematous and necrotic. This potential diagnosis should be borne in mind for a patient who complains of abdominal symptoms with an unknown cause, and duplication cyst should be recognized as a fatal cause in infant.
Congenital duplications of the alimentary tract are rare diseases, with an incidence of 1 in 4,500 neonatal autopsies or 1 in 18,000 livebirths. 1 Mostly of them are detected in the first 2 years of life or antenatally, but can remain undetected until older age. 2 The clinical presentation depends on location, size, and the presence of ectopic gastric mucosa.
Although considered to be benign, such duplications can lead to lethal complications, including volvulus, intussusceptions, or bowel obstruction if not properly treated. 3
We report a fatal case of an infant who presented with intestinal obstruction associated with an ileocecal duplication cyst.
Report of Case
The patient was a 41-week-gestational-age infant girl with a birth weight of 3300 g. After an uneventful pregnancy, the patient was delivered spontaneously and healthy until this episode.
At 35 days of age, the patient was admitted to our hospital with a one-day history of anorexia, vomiting and recurrent diarrhea.
On admission, conscious level was Glasgow Coma scale E2 V2 M2, and blood pressure was 104/flat. Physical examination revealed a distended and tender abdomen. The plain abdominal radiograph showed thickened intestinal wall and intestinal obstruction (Fig. 1A). The patient developed recurrent diarrhea, stool cultures were negative. Laboratory values were significant for a c-reactive protein (CRP) of 1.7 mg/dl (normal range was less than 0.3 mg/dl). Blood cultures were negative and cerebrospinal fluid was normal. The patient was suspected intestinal obstruction due to enteritis, antibiotics were started (ABPC/MCIPC and AMK). 4 hours after admission, she was pale with a temperature of 39.2 °C and 220 per minutes pulse. Laboratory data revealed high CRP level (14.2 mg/dl). Blood pressure was low, and the fevers, vomiting, and diarrhea persisted and worsened despite antibiotics. She showed intractable paraoxysmal supraventricular tachycardia (PSVT). She failed to respond to medical managements and died 27 hours after admission due to multiple organ failures.

Abdominal plain radiograph showed thickened intestinal wall and intestinal obstruction.
The autopsy was performed. Macroscopic findings of small intestine showed edematous and necrotic (Fig. 1B).

Macroscopic findings of small intestine in autopsy. Edematous and necrotic ileum was seen.
The ileocecal duplication cyst (3 × 3 cm) was attached to the ileum. The cyst was unilocular, contained watery fluid, did not communicate with the adjacent intestinal lumen (Fig. 1C). Cyst fluid culture was negative.

The ileocecal duplication cyst (3 × 3 cm) was attached to the ileum.
Intestinal obstruction due to the ileocecal duplication cyst was recognized. Microscopic finding of the ileocecal duplication cyst had an undefined mucosal lining though it resembled pyrolic glands or duodenal glands.
Discussion
Duplications of the alimentary tract can be located anywhere between the mouth and the anus. 4 They are most commonly found in the ileum (30%), ileocecal valve (30%), duodenum (10%), stomach (8%) Jejunum (8%), colon (7%) and rectum (5%) with the half of the all lesions may contain ectopic gastric mucosa.5,6 Most alimentary tract duplications are cystic (80%-90%), with the remainder being tubular 7 They have three common features, hollow structure that has a wall of smooth muscle often shared with the contiguous intestinal tract, lined by mucous membrane similar to some part of the alimentary canal, and usually attached to some part of the alimentary tube. 8
The clinical symptoms are highly variable from minor digestive problems to intestinal obstruction, gastrointestinal bleeding, or perforation. 9 Most patients present before the age of 2 years with obstructive symptoms, pain, or an abdominal mass. A minority of patients will have volvulus or intussusceptions. The presence of gastric or pancreatic mucosa can lead to peptic ulceration, perforation, and hemorrhage. Early diagnosis and treatment reduces the risk of dangerous complications, such as bowel perforation, bleeding, obstruction, and malignant alteration. Resection of duplication alone is the treatment of choice, and in uncomplicated cases laparoscopic resection is advised. Surgically treated intestinal duplications have good prognosis, however, such duplications can have a fatal consequence if not properly treated. Possible complications like bowel perforation, bleeding, obstruction, and malignant alterations are the reason why all duplications should be surgically treated at the time of diagnosis. 10
Alimentary tract duplications can be easily misdiagnosed as other disorders. 5 Pyloric and duodenal duplications can mimic hypertrophic pyloric stenosis or choledochal cyst.11,12 Ovarian cyst should be considered in female patients, and adolescent patients can sometimes have a presumptive diagnosis of Crohn's disease. 5 Yousefzadeh et al 13 showed that duplication of the colon and rectum clinically presented as abdominal pain, vomiting and chronic constipation, a significant number of patients were thought to have Hirschsprung's disease.
In our fatal case, there are two reasons for this diagnostic difficulty: first, fevers, vomiting, and recurrent diarrhea persisted and worsened despite antibiotics. The patient was suspected intestinal obstruction due to enteritis, however, actually the ileocecal duplication cyst led to intestinal obstruction and necrotizing ileum; second, the patient died in an instant due to multiple organ failures. If this patient was considered for exploratory laparotomy, she might be able to be alive. However, the patient was getting worse very quickly due to multiple organ failures and showed intractable PSVT. She couldn't even move to perform CT scan. Exploratory laparotomy was impossible.
It is demonstrated a high association of other anomalies in these patients including skeletal and urologic abnormalities,13,14 however, in this case, there were no other congenital anomalies.
Sudden unexpected death of infants associated with duplication cysts is extremely rare with only 4 cases reported in medical literature to date (Table 1). Puligandla PS et al 5 and Byard RW 15 reported the patients presented with group B streptococcal sepsis and Clostridium perfringens sepsis, respectively. Kibayashi et al 16 reported the patient died at home after being diagnosed as having gastroenteritis. In present case, though blood, stool and cyst cultures were negative, the patient had high fever and CRP level elevated. Infection is suspected to be a risk factor for sudden and unexpected death in infants with duplication cysts.
Infant death cases due to duplication cyst.
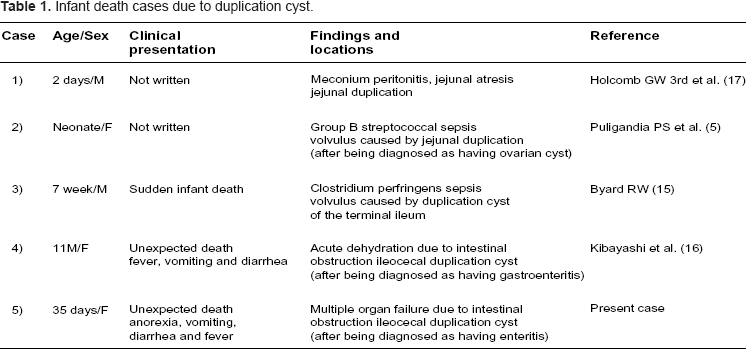
In all cases, the preoperative diagnosis of alimentary tract duplication was difficult. This potential diagnosis should be borne in mind for a patient who complains of abdominal symptoms with an unknown cause, and duplication cyst should be recognized as a fatal cause in infant.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material. Written consent was obtained from the patients parents for publication of this study.