
Abstract
Background
Maternal nutrition and some variables are the main determining factors of birthweight and delayed intrauterine growth of children.
Objective
To explore the association between the mothers’ biological and sociodemographic characteristics, and the anthropometry status in children under five years of age.
Design
The population consisted of a sub-sample of 1,047 mother-and-child selected pairs from the probabilistic National Nutrition Survey, carried out in Mexico. Mother-and-child pairs included mothers aged 12 to 49 years, with children under five years of age. Data on sociodemographic characteristics, obstetric history, 24-hour recall dietary intake, and the women and children's anthropometry were collected. The association between maternal characteristics and children's anthropometry status was assessed using multiple logistic regression models.
Result
Nearly 16.7% of the children <5y of age were stunted (13.5% ≤ 2y and 18.8% > 2y). The height/age of the children was severely affected by maternal height and birth order. In addition, the interaction between socioeconomic level and maternal schooling had a marginal effect (p = 0.09) in the ≤2y group. On the other hand, whether the family received social services and the interaction between maternal height and a dichotomy urbanism variable were significant (p = 0.05) and (p < 0.01) respectively in >2y group.
Conclusion
Some biological and socioeconomic characteristics among mothers have a negative effect on their children's attained size, especially in the period between 2 and 5 years of age.
Introduction
Maternal nutrition and variables like age, birth spacing, number of births, socioeconomic level, and schooling, are the most relevant determinants of birth weight and delayed intrauterine growth (DIUG) of children in developing societies. Maternal malnutrition alone may account for up to 50% of DIUG incidence in these countries (González de Cossio, Rivera, Shamah et al. 2001; González de Cossio, Sanin, Hernández et al. 1998).
Malnutrition prior to pregnancy, low weight gain during pregnancy, and a short gestational period, have immediate and long-term effects on fetal health. Such effects include low birth weight and a higher prevalence of associated complications (Neggers and Goldenberg, 2003; Osrin and de L. Costello, 2000). Maternal variables such as smoking during pregnancy are also thought to have negative effects on fetal growth, although this finding has not been fully substantiated.
Maternal height is a useful indicator to predict children's risk of developing malnutrition. However, it has low predictive value in populations with a high prevalence of excess weight among adult women (Ramakrishnan, 2004).
From an epidemiological perspective, healthy newborns in developed countries have a 98% probability of surviving during their first five years of life (Mosley, 1988). The probability of survival is greatly diminished in developing countries, as a result of physical and biological insults. These may originate in the maternal health before or during pregnancy, upon delivery, or in postnatal life. Many of these environmental, biological, and physical insults are positively related to socioeconomic conditions. Their cumulative effect is reflected as a suboptimal nutritional status. When malnutrition occurs in infants and preschool-age children, it is associated with delayed physical growth, and delayed attainment of mental development milestones, which in turn result in poor school and intellectual performance. In addition, these negative effects may also hinder the individual's capacity to earn a living, thus perpetuating the malnutrition-poverty cycle (Uauy, Albala and Kain, 2001).
Statistics reported from Mexico in 1999, showed approximately 17.7% of children less than five years of age are affected by delayed growth. Between 21 to 49% are anemic, between 33 and 66% present with iron-deficiency, between 21 and 34% present with zinc deficiency, over 50% have low serum concentrations of vitamin C, and 24% have depleted vitamin A levels (Rivera, Shamah, Villalpando, 2001; Villalpando, García-Guerra, Ramírez et al. 2003; Villalpando S, Montalvo-Velarde, Zambrano Chem et al. 2003). These micronutrients are necessary for appropriate growth. The average height of reproductive-age women in Mexico is 154 cm in urban areas and 150 cm in rural regions (González de Cossio, Rivera, Shamah et al. 2001). The height of more than half of these women is therefore below the median NCHS (National Center Health Statistics) reference data (World Health Organization, 1983).
The objective of this study was to explore the association between selected biological and sociodemographic characteristics of mothers with the anthropometric status of their children under five years of age. Results of this study are expected to contribute to the understanding of the origin of stunted growth in children in Mexico and by extension in other countries with similar economic development. Such information is necessary to design possible intervention strategies to reduce the incidence of child malnutrition, along with its long- and short-term consequences.
Subjects and Methods
Sample Selection
Study subjects were women aged 12 to 49 years, who had at least one child under 5 years of age at the time of the survey, and had complete data on sociodemographic characteristics, anthropometric characteristics of the mothers and their children, hemoglobin concentration, obstetric history, morbidity, breastfeeding, and 24-hour dietary intake recall, however the diet information was obtained only in a fifth of the women.
To get the sample of 1147 mother-children, we selected the mothers who had all the information required for the complete analysis. The information was provided in some cases by caregivers of the children, but in these cases the participants were excluded. In families where they have had more than one child we selected the youngest.
NNS-99 methods have been described elsewhere (Resano-Pérez, Méndez-Ramírez, Shamah Levy et al. 2003). In summary, it was a probabilistic survey conducted in four nationally-representative regions (North, Center, South, and Mexico City), stratified by urban (pop > 2500) and rural areas (pop < 2500). Families were selected according to a sampling frame developed by the Mexican National Institute of Statistics, Geography and Information
Study
Stunting of children (short height for age) was defined as height for age 2 SD below the mean NCHS-WHO reference data. Data on breastfeeding for children under 2y of age identified whether the child was or was not breastfed. Morbidity information on diarrhea and respiratory infections was also obtained. Maternal variables included age (rounded years), literacy, marital status (cohabitation with a partner or not), schooling (number of completed school years), occupation (paid occupation, student, or housewife), time of residence in the locality (lifetime, less than one year, or number of years), and ethnicity (families in which at least one member spoke an indigenous language were classified as indigenous). The socioeconomic index (SEI) was constructed based on principal components analysis, applied to variables related to characteristics of the household and family possessions, and access to the healthcare systems (insured or not). Also considered was the family residence, including region (North, Center, South, or Mexico City) and type of residence (rural or urban). Maternal characteristics included were: age at menarche (years), and existence of regular menstrual periods (dichotomy). Continuous variables were: number of pregnancies, number of interrupted pregnancies, number of liveborn children, age of the last liveborn child, number of deceased children, and birth order of the index subject; which was classified as an ordinal variable.
The percentage of adequacy of protein and energy intake was calculated based on data from the 24-hour dietary recall, and by comparing it with recommended daily allowances suggested by the United States Institute of Medicine (Dietary Reference Intakes, 2000).
Height and weight were used to calculate BMI, expressed as weight/height 2 (kg/m2). Maternal nutritional status was categorized according to WHO (1997) criteria modified by Must A (1991) and waist measurement (cm).
Hemoglobin concentrations were determined in a sample of capillary blood obtained by finger prick and measured by HemoCue. Hemoglobin determinations of families living in communities located more than 1000 m above sea level were corrected by the following equation published by Ruiz-Arguelles (1981).
Cut-off values used to diagnose anemia in children were: 6 to 11.9 months old: <95 g/L, and 12 to 59 months old: <110 g/L, and in women: <120 g/L, as recommended by INACG (1989) and by WHO (1992).
Data Analysis
The response or result variable is the dichotomic variable that identifies the presence of stunting in the children.
Due to biological factors, we stratified the sample in two age groups: those greater than 2 years of age (n = 674), and children aged 2 and under (n = 473), because until the 2 years of age it is the period in which the children reach the greater growth. Apparently simple strategies such as ensuring adequate frequency of feeding, provision of high quality complementary foods that are rich in both macro and micronutrients and promotion of exclusive breastfeeding are recognized as optimal measures to promote child growth and development (Butha, Ahmed, Black et al. 2008).
In the small children the exposure to environmental factors is closer to the measurement time, whereas in the older children the factors which affected the growth could be absent at the time of the study.
Within each age group, we compared the behavior of sociodemographic and nutritional variables of the mothers of children with and without stunting. We used the t-student test for independent samples, after verifying the normality of the continuous variables, and the Chi-squared test for the categorical variables through SVY module in STATA in order to take into account the sample design. The standard errors of the estimates were adjusted for the sample design.
With the purpose to estimate the effect of maternal characteristics on the probability that a child would present with stunting, we used regression logistic models for complex samples using expansion factors to make inference to the population. Although the sample under study included siblings, it was not necessary to consider in the models a second grouping level (the family within the conglomerates) because the estimation methods used stand up to correlation within a second level. For the construction of the models we began by exploring bivariate relations. Those variables that were significant with a p-value < 0.25 formed part of a complete model that was later purged to obtain a model that only included statistically significant (p < 0.05) and biologically or socially important factors and we tested some interactions with biologically reasonable variables.
We evaluated the pertinence of the continuous variables in the model through its lineal and squared form. We verified the linearity of the continuous variables through their inclusion in the model in its categorical form (quartiles). We also tested the importance of interactions between variables mindful of their usefulness and biological sense. Through the test of the condition number we verified that a problem of multicolineality would not emerge. We used the Hosmer-Lemeshow (1989) test to evaluate the reliability of the model.
The STATA module for complex samples (SVY) was used to estimate parameters Stata version 7.0 (Stata Corp. College Station, TX, 2001 for Windows). Data was entered in the Clipper 5.1 computer program (1987), with data entering formats that included contingent and range validation. Statistical data analysis was carried out using the statistic analysis software SPSS version 10 (2000) for Windows, and Stata version 7.0.
Informed consent to participate was obtained from all women before being surveyed. The NNS-99 protocol was approved by the Mexican National Institute of Public Health (
Results
This study included 1,147 mother-and-child pairs. When applying the population expansion factors, the sample is representative of 1,469,164 pairs at a national level.
According to NNS-99, the prevalence of stunting in children under 5 years of age was 17.8%. In this subsample, it was 16.9%, with lower prevalence in children under 1 year of age.
Among the live-born children, 17% presented with stunting. Of the 84.3% of children whose mothers reported regular menstruation, 16.1% had stunting. Maternal illiteracy was associated with a 3.4 times greater probability of having stunted children; 60% of the children of the 9.3% of women surveyed who were illiterate, were stunted. 11.1% of surveyed women were indigenous and half of them had a child with stunting; the child of an indigenous woman has 2.8 times the risk of presenting with inadequate height.
Of the 17% of women who were in paid work, 12.2% had a child with inadequate height. More than 90% of the women reported having a stable partner, and of these 17.4% had a child with stunting. 24.3% of women surveyed were new migrants in the localities studied, i.e. they had resided in the locality for less than one year. Among these women, 13.6% had a child with stunting (Table 1).
Maternal characteristics and prevalence of stunted in children of less than 5 years of age.
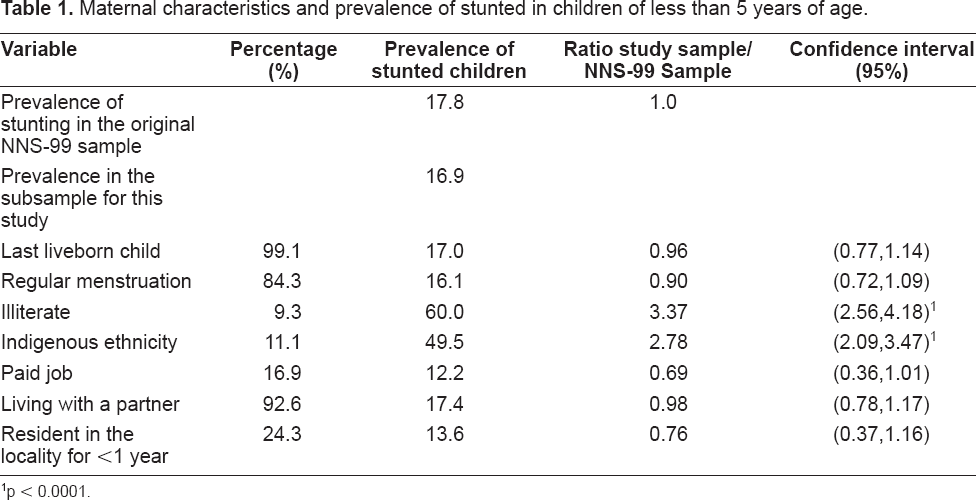
p < 0.0001.
The average age of the mothers of the children under age 2 was between 26.4 and 27.6 years, and no significant differences between the mothers of children with stunted height and normal children were noted. However, in the group of mothers of children older than 24 months, there is a significant difference (p = 0.03) in favor of the mothers of children with a normal nutritional status and that were older (29.7 years old versus 27.9). Among both the children <24 months and the older age group, it was observed that as socioeconomic status improved, a proportional decline occurred in the probability of a child with stunted height (p < 0.001). Also in both age groups, the highest prevalence of low height was found in the southern and central regions of the country and in rural areas.
Differences in years of schooling among the mothers are statistically significant, given that fewer years of study and lower literacy increased the risk of having children of small height (p < 0.001) (Table 2).
Selected variables of mothers to stunted and non-stunted children ≤24 m and >24 to 59 m 1 .
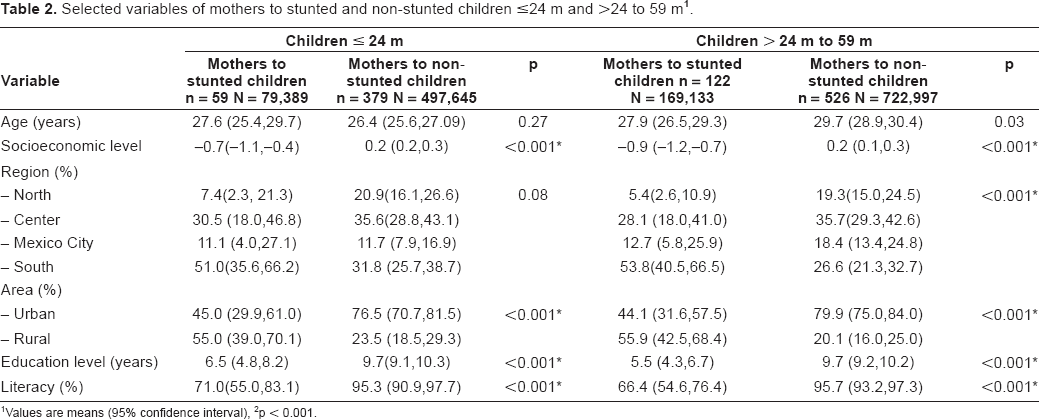
Values are means (95% confidence interval)
p < 0.001.
Specifically for the children under 24 months of age, it was observed that a lower socioeconomic level increased the risk of smaller height, as did residing in the South or in rural areas, or having mothers with less schooling and/or illiteracy (p < 0.001) (Table 2). 11.3% of the children between ages 2 and 5 had a sibling and 0.6% had 2 siblings in the sample, while in the group of those under age 2 the percentages were 2.8% and 0.2% respectively.
Two models were developed with logistic regression in complex samples to estimate the probability that a child would present with smaller height (Table 3). For children under 24 months, the interaction between birth order and maternal height and the interaction between maternal schooling and the ISE showed significant effects in the probability of stunting.

The interaction between maternal height and birth order (p < 0.026) shows that lower maternal height and higher birth order increased the probability of stunting. As maternal height increased, the probability of having a child of small stature decreased, but for children in fourth or later position among siblings in the birth order, the probability decreased very slowly (Fig. 1). On the other hand, less maternal schooling and lower socioeconomic level increased the probability of stunting (p = 0.086) (Fig. 2).


Among the children older than 24 months, the variables that formed part of the final model were: maternal height, birth order, the interaction of maternal height with locality type (urban- rural), and access to health services (p = 0.01). If the child occupied higher placement in the birth order, the probability increased (Fig. 3).

From the interaction we interpreted that the women with smaller height and who resided in a rural environment had a greater probability of having a child with a smaller height. But if maternal height surpassed 150 cm, the probability of stunted height is the same in both rural and urban areas (p = 0.001) (Fig. 4) (Table 3).

Models with interactions of low height (<150 cm) of the mothers were explored; nevertheless we did not observe any effects that could offer major information changes to the previous models.
Discussion
In Mexico, the probability of small height is associated with maternal characteristics primarily related to socioeconomic status, like low maternal schooling, and residency in the southern region of the country and in rural zones (Table 2).
In reference to ethnicity, the risk of small stature is 2.8 times greater for residents of indigenous areas. The notable difference among indigenous and non-indigenous children is the result of the significant differences in the living conditions of the two populations. The majority of indigenous children are exposed to a poor diet and greater risk of developing infections, which are the two direct causes of malnutrition. Mothers are generally those who make the decisions related to health care, feeding, and child rearing patterns.
Most studies exploring the association between maternal characteristics and children's growth are focused on the first two years of life. Studies using birth weight as the outcome variable or those assessing growth during the first two life years, reflect the effects of maternal characteristics during pregnancy or breastfeeding (Kelly, Kevany, de Onis, Shah, 1996; Kramer, Kelly 1998; Doley, Crawford and Costeloe, 2000). The present study presents the effects of social and environmental variables on the anthropometric status of children who are no longer biologically dependent on the mother for their growth, although they remain reliant on her social and intellectual abilities.
As expected, genetic factors were important contributors to children's growth. Children of tall mothers were taller at baseline and experienced a faster rate of increase in height over time. Even though the present study does not consider paternal height, its effect has been documented in other studies in which the influence of the height of both parents on children's growth has been shown (Black and Krishnakumar, 1999). Maternal height and pre-pregnancy weight, which are the result of genetic and environmental influences prior to pregnancy, are also important determinants of birth size, particularly in developing countries (Kramer, 1987). Our study, like in other studies illustrates (Hernandez-Diaz, Peterson, Dixit, Hernández et al. 1999) that maternal height plays a fundamental role in the height the child will reach up to age five, and while it can not be assured, we suspect it can also be associated with height attained in adult life. In children <24 months it is associated in an important manner with the birth order that the child occupies, and among the children older than 24 months, with area of residence.
In our study the BMI of mothers has shown a positive but not a significant tendency of undernutrition in the under five year olds. Children of well-nourished mothers had a lower risk of being under-weight compared to children of acutely malnourished mothers. The reason may be that thin or malnourished mothers cannot provide sufficient breast milk because of their nutritional deficiency. Acute malnutrition of the mother could be an impediment for her child's growth (Rayhan and Sekander, 2006).
Also, there are evidence that some socioeconomic, demographic and health and community factors on chronic malnutrition or stunting and other factors such as birth order, months of breast-feeding, birth size, mother's BMI, mother's height; were significantly associated with severe as well as moderate stunting (Rahman and Chowdhury, 2007).
We did not find an association between biological characteristics of mothers and children anthropometric.
The prevalence of stunting in children under five years of age in this sample was 16.9%, which is comparable to the 17.8% obtained for the total sample of NNS-99 (Rivera, Shamah, Villalpando et al. 2001). It can thus be concluded that the sub-sample used in this study, as well as its conclusions, are relevant to the whole sample. Our data confirm findings from other studies showing that stunting starts in the second or third year of life, and remaining stable in the following years (Frongillio, 1999). The pattern appearance of stunting, suggests that there is a window of opportunity for preventive interventions, when the child is 2 to 3 years old.
Most of the variability of “height for age” used in this study to indicate stunting, was explained by changes in the variables associated with poverty. A high proportion of stunted children had mothers with low educational levels and inadequate nutrition, variables which in turn are associated with a low socioeconomic level. The inverse association between birth order and the index child's height/age suggests that opportunities for adequate growth decrease as family size increases. Decreased opportunities could be the result of lower availability of food, less personal care for the child, and accessibility to health services. Although no differences in energy and protein intakes were found between mothers of stunted children and those of non-stunted children, a lower prevalence of stunting was observed in children whose mothers were overweight or obese according to BMI (normal: 47.1%, overweight: 41.2%, and obese: 12.8%). This maternal characteristic may represent the woman's ability to provide her family with food. However, the prevalence of excess weight and obesity was inversely related to socioeconomic level among women in this sample (data not shown). Other studies have linked maternal obesity and overweight with more complications during pregnancy and delivery, as well as to low birth weight (Perlow, and Morgan, 1994; Perlow, Morgan, Montgomery, Towers and Porto, 1992). However in our study, among children aged >24 mo, maternal obesity or overweight proved to be a protecting factor for height for age.
This is relevant, if we consider that in countries of Latin America, where the prevalence of obesity is a growing problem, and these countries are confronted by a complex overlay of two sets of health problems where maternal overweight coexists with undernutrition in children (stunting) (Waters, 2006).
The simultaneous prevalence of overweight or obesity and linear growth retardation (stunting) has been noted in countries undergoing nutritional transition. Some studies have suggested that greater national incomes are associated with greater obesity levels in women and lower levels of stunting in children. (Martorell, Kettel, Hughes and Grummer-Strawn, 1998).
Some studies found that concurrent overweight or obesity and stunting is an important public health issue in low-income areas of rural Mexico beginning in early childhood. Even within this impoverished population, children living in households with low relative socioeconomic level are the most vulnerable (Fernald and Neufeld, 2007).
Barquera et al. 2007 has shown that maternal central adiposity was associated not only to chronic diseases, but also to child stunting.
The mean age at menarche was higher than that found in other studies (Ramos, 1986). This may be due to recall bias, since, for many women, menarche occurred long before the survey date. It could also be interpreted as a delay in attaining the critical body mass necessary for menarche (Frisch and Revelle, 1970). Delayed body mass attainment is often related to nutritional deficiencies, including energy and micronutrient deficiencies (ACC/SCN, 2000; Svedberg, 2000), serving as an example of the transmission of malnutrition across generations.
We found three interactions: in the children under 24 months of age, it was observed that smaller maternal height and higher birth order resulted in greater probability of smaller height. The birth order number that the child occupied in the home can be a determinant of the nutritional state in poor families, due to the vying among siblings for low resources and care, and maternal height also reflects said situation.
The other interaction also applies to the children <24 months, among whom the probability of small height is seen to increase due to low maternal schooling and socioeconomic status, variables again associated with poverty level.
The third interaction applies to the children >24 months, for whom maternal height and area of residence increased the probability of small height. This is surely due to the adaptation of the child to the malnutrition in poor communities of our country.
In conclusion, this study demonstrates that maternal biological and social characteristics are determinants of their <5 year-old children's anthropometric status. Some of them are modifiable or preventable (maternal education, family planning programs, orientation regarding age at the last pregnancy). Others are not (ethnicity). Interventions aimed to reduce the negative impact of those variables and efficacy and effectiveness evaluation research of these programs are warranted.
Sponsorship
This study is supported by the Health Ministry of Mexico.
Disclosure
The authors report no conflicts of interest.
Footnotes
Acknowledgement
Teresa Shamah was the person in charge of the National Nutrition Survey, and the idea to develop this manuscript, from its conception, design, conduct and interpretation of data was hers.
Lucia Cuevas was responsible for complete supervision of data collection and analysis while.
Hortensia Moreno participated in processing and analysis of the information and in the design of the statistic models.
Eric Monterrubio and Marco Antonio Avila participated in processing and analysis of the information. They helped us on the section of results and discussion.