
Abstract
Background:
Nutrition among children under 5 plays an important role in the overall development of children physically and psychologically. Nutritional deficiencies and malnutrition generally affect children. In this study, we estimate the prevalence of 3 malnutrition indicators underweight, stunting and wasting and to assess factors associated with them.
Objective:
The main objective of the study was to assess the factors contributing to malnutrition among children under 5 years old.
Design:
The study employed a descriptive cross-sectional study design to assess the factors contributing to malnutrition among children under 5 years of age.
Methods:
This is quantitative cross-sectional facility-based study of 245 children aged 11 to 49 months. A structured questionnaire was used, and anthropometric measurements were taken to collect data. The Pearson chi-square test was used to assess the bivariate association between the outcomes and the characteristics. The binary logistic regression model was employed to estimate the crude and adjusted odds of malnutrition indicators among the characteristics observed in the study.
Results:
The prevalence of underweight, stunting, and wasting were 35.9, 13.9, and 33.9%, respectively. Underweight was significantly higher among females compared to males (42.0% vs. 24.1%) and highest among children aged 11 to 23 months (53.6%). Female children had 3 times more odds of being underweight (AOR: 3.09, 95% CI: 1.56-6.12). Compared to children aged 11 to 23 months, the odds of being underweight were less among children aged 24 to 35 months (AOR: 0.26, 95% CI: 0.13-0.51, P < .001), and 36 to 47 months (AOR: 0.9, 95% CI: 0.03-0.29, P < .001). Wasting was less prevalent among children aged 11 to 23 months (4.8%). Also, wasting was high among children aged 24 to 35 months (AOR: 27.41, 95% CI: 9.12-82.37, P < .001), 36 to 47 months (AOR: 28.23, 95% CI: 7.59-104.94, P < .001), and 48 to 59 months (AOR: 18.10, 95% CI: 3.04-107.76, P < .001). None of the observed factors were associated with stunting in the study.
Conclusion:
This study concludes that child malnutrition was high among under-five children. Promoting the use of healthy complementary feeding, preventing diarrheal diseases, and vaccinating children integrated with access to nutrition education programs are vital interventions to improve the nutritional status of children.
Background
Children less than 5 years old worldwide are known to be vulnerable and susceptible to many problems, especially in nutrition. Nutritional deficiencies and malnutrition generally affect children more than any other group. Poor nutrition occurs in developing countries, as well as developed countries,1 -3 indicating that hunger and malnutrition remain devastating problems for the world’s poor and needy.
The World Health Organization defines malnutrition as deficiencies, excesses or imbalances in a person’s intake of energy and/or nutrients. 4 It covers 2 broad categories of conditions: undernutrition (which includes stunting, wasting, underweight, and micronutrient deficiencies), and other overweight, obesity, and diet-related non-communicable diseases (NCD) like heart disease, stroke, diabetes, and cancer. 4 Malnutrition may also occur in children who are unable to absorb vital nutrients or convert them to energy essential for healthy tissue formation and organ function. 5 Available research indicates that factors such as family size, parental educational level and occupation, infants and young feeding practices, and age and gender of the child grossly affect childhood nutrition.6,7
Globally, malnutrition plays a significant role in the deaths of about 16 000 young children every day, with almost all of them in the developing world.1,8 That is a yearly death toll of about 6 million children. By weakening resistance to infection and disease, malnutrition contributes to more than half of the deaths of children under 5, worldwide. Malnutrition has been a persistent problem for young children in sub-Saharan Africa. A high percentage of children fail to reach the normal international standard height-for-age; that is, they are stunted. 9 One in 3 pre-school children in the developing world is undernourished.
Malnutrition or micronutrient deficiencies continue to be a major health burden in developing countries. It is globally the most important risk factor for morbidity and mortality, with millions of children under 5 years of age affected.8,10 Apart from wasting, stunting, marasmus, and kwashiorkor, deficiencies in iron, iodine, vitamin A, and zinc are also manifestations of malnutrition in developing countries. 11 Interventions to prevent malnutrition range from promoting breastfeeding to food supplementation schemes, whereas micronutrient deficiencies would best be addressed through food–based strategies. These strategies include dietary diversification through home gardens and small-scale livestock to minimize the burden on public health. 4 The sub-Sahara African region has now the world’s highest rate of stunting among children at 43% and has shown little improvement over the past 15 years. Ghana has not seen much improvement in childhood malnutrition and mortality even with the remarkable gains in health infrastructure and investment since independence. Previous studies show a trend of increases in the malnutrition rate among children in Ghana. For instance, malnutrition rate among children under 2 years recorded 2.3% in 2003, 5.4% in 2004, and 7.5% in 2005.9,12 In most sub-Saharan African countries, the level of wasting among children under 5 years of age remained below the emergency threshold level but at poor nutritional threshold levels (6.5%) for Africa. Nambile and colleagues showed that approximately 45% of all deaths in children under 5 years were associated with malnutrition. This further underpins the impact of malnutrition on child survival.7,13
The literature7,8,10,13 suggests malnutrition is still a bigger problem in some parts of the world including Ghana. It is therefore critical that we continue to investigate the factors that contribute to malnutrition among children under 5 years of age. In this study, we leveraged the primary data collected at the St. Elizabeth Catholic Hospital in the Ahafo region of Ghana to estimate the prevalence of selected malnutrition indicators, underweight, stunting, and wasting among children under 5 years. We also descriptively assess the perceived factors of malnutrition as well as the caregiver’s knowledge of malnutrition. We further assess the factors associated with these 3 malnutrition indicators among children under 5 years.
Methods and Materials
Study design
The study adopted a quantitative research approach using a cross-sectional design. Quantitative research seeks to answer questions of how much and how many and is concerned with relationships (especially causal relationships) between variables. 14 The exploratory design allows the use of questionnaires distributed to a large sample of the population and is therefore intent on finding facts that relate to the field of study. 14 This is very important, especially since no or little previous studies have been done in Ghana on the factors contributing to malnutrition among children under 5 years.
Study area
The research was conducted at St. Elizabeth Catholic Hospital in the Ahafo Hwidiem of Asutifi South District in the Ahafo Region and its capital is Kenyasi This district covers an area of 1799 km 2 . Asutifi South district has a total population of 52 259, accounting for 2.7% of the Brong Ahafo Regional population of 2 310 983. The female population of 25 498 forms 49.8% of the district’s population as against the male population of 26 761 constituting 51.2%.
Study population and selection of participants
The study population was women who have children under 5 years and are attending the St. Elizabeth Catholic Hospital Outpatient Department and Children’s ward for treatment of their children with malnutrition. An initial screening sheet was used to select eligible children under 5 years of age with a diagnosis of malnutrition. To be eligible, the child should be residing in a community under the Asutifi South District in the Ahafo Region. This strategy was used to exclude women and their children who are not residing in the Asutifi South District.
Inclusion criteria
The inclusion criteria for participation in this study include:
Those willing to partake in the study
Those who have been diagnosed with malnutrition
Those who have had any form of underweight concerning Body Mass Index (BMI)
Exclusion criteria
Those who were not willing to partake in the study
Sample size determination
The study used the Cochrane sample size formula for prevalence estimation to estimate the minimum required sample size. Using a 19.0% prevalence of stunting from the 2014 Ghana Demographic Health Survey, a margin error of 5% at a 0.05 significance level.
Adopting the Cochrane’s formula, n = (Z2pq)/(e2)
e is the desired level of precision (ie, the margin of error)
p is the proportion of the population with malnutrition
q is 1-p
Using a margin of error (e) of 0.05, α = 5% at a 95% confidence interval (Z = 1.96), and
P (adopting the measure of malnutrition with the highest prevalence from the 2014 Ghana Demographic Health Survey, stunting = 19%). And q (1-p) = 81%
n = (1.962) (0.19) (0.81)/(0.052)
n = 233.39
Including a 5% non-responding rate, the final sample size was 245 Children/caregivers.
A total of 245 participants were selected to participate in the study.
Data collection tool and procedure
A questionnaire was used for the data collection. The questionnaire was designed in English and translated into the local language (Twi). The questionnaire was designed according to the study objectives based on an extensive literature review. The questionnaires were conducted by trained research assistants with previous experience in conducting surveys. The questionnaire was divided into 5 sections (A to E) with 30 test items; Section A: Child demographics and anthropometric measurement, Section B: Parent demographic information, Section C: knowledge of parents on child nutrition, Section D: Factors Contributing to malnutrition among children, and Section E: Consequences of malnutrition on children. The questionnaire was pretested, and the ambiguities found were corrected. The overall internal consistency (Cronbach’s alpha) was 0.81.
Statistical analysis
The data was imported into Stata SE version 17 (Stata Corp, College Station, TX, USA) for all analysis. The characteristics of the study participants were described using percentages and frequencies for categorical variables and median and interquartile range for continuous variables. The prevalence and corresponding 95% confidence intervals for underweight, stunting, and wasting were estimated. The prevalence of the nutritional outcomes of the study was described across the observed characteristics. Pearson’s chi-square test was used to assess the bivariate association between the nutritional outcomes and the observed characteristics.
The binary logistic regression model was employed to estimate the crude and adjusted odds ratios of malnutrition among the children among the observed characteristics. All variables observed in the study were considered for the final multivariable binary logistic regression model. However, variables with high multicollinearity, thus variance inflation factor value above 10 (Sex of caregiver and child being given legumes), were excluded. The area under the received operating characteristics was above 60% for the multivariable model for all 3outcomes. The model was appropriately fitted from non-significant P-values (P > .05) recorded for all 3 outcomes. All statistical analyses were considered significant at an alpha value of 0.05.
Results
Background characteristics of study participants
A total 245 children were involved in this study with a median age of 24 months (IQR: 14-27) with a third (66.1%) of the children being females. The median age of the caregivers was 30 years (IQR: 25-34 years) with 6.5% of them being males. Most of the caregivers either had primary (48.2%) or Junior high (41.6%) level of education. Majority (85.7%) were Christians, 79.2% had family with less than 5 members, while 63.7% had only 1 child under the age of 5 years (Table 1).
Background characteristics of child and caregivers in study.

All the children had been breastfed with a third (33.9%) still being breastfed. The majority (58.0%) of the children were first breastfed within an hour of birth. Excluding breastfeeding in the first 6 months of birth was prevalent among 29.4% of the children while 56.7% of the caregivers breastfed or to breastfeed the children to 18 months and beyond. More than half (60.8%) of the children had experienced diarrhea 2 weeks prior to the interview. Majority of the caregivers had received education on child nutrition and feeding (Table 1).
Table 1 also the distribution of the characteristics by the sex of the child. None of the characteristics significantly varied from the Pearson’s chi-square tests (Table 1).
Table 2 describes the results of participants’ general knowledge of the causes of child malnutrition. Out of 245 participants, the majority (85.3%) indicated an unbalanced diet while a significant proportion (41.3%) agreed that mental health problems were the cause of malnutrition among children and few indicated that stomach/digestion problem (23.7%) was the causes of malnutrition among children under 5 years.
Other perceived factors and knowledge on nutrition among caregivers.

Table 2 also describes the results on knowledge of factors contributing to malnutrition among children under 5 years. The most perceived factor of malnutrition was large households (79.6%) followed by knowledge level on nutrition (63.7%). The least perceived factor of malnutrition was the marital status of the mother (8.6%) and the age of the mother (9.0%). None of the mothers agreed that the health status of the parents and the HIV status of mother were contributing factors of malnutrition among children under 5 years.
Most of the caregivers also thought the failure of children to thrive (70.2%) was a consequence of malnutrition and 83.7% of education on awareness is a measure to improve nutrition among children (Table 2).
Prevalence of malnutrition among children under 5 years of age
Among the 245 children in the study, 35.9% were underweight with 29.8% moderately underweight while 6.1% were severely underweight. The prevalence of stunting was 15.9% among the children with 9.0% moderately stunted and 4.9% severely stunted. The prevalence of wasting was 33.9% among the children with 26.9% moderately wasted and 6.9% severely wasted (Figure 1).

Nutritional status of children by sex.
Moderate underweight was higher among females (35.8%) compared to males (18.1%). Severe stunting was high among males (8.4%) compared to females (3.1%) while moderate stunting was higher among females (11.1%) compared to males (4.8%). In terms of wasting, a similar distribution was observed between males and females
Wasting was less prevalent among children in the age group 11 to 23 months with 1.2% moderately wasted and 3.6% severely wasted while moderate wasting and severe wasting were 42.6% and 5.7% among children aged 24 to 35 months, 33.3% and 20.0% among children aged 36 to 47 months and 33.3% and 11.1% among children aged 48 to 49 months (Figure 2).

Nutritional status of children by age group of children.
Factors associated with underweight among children under-5 years
The bivariate analysis showed that the sex of the child (P = .006) and age group (P < .001) were factors significantly associated with being underweight among children. From the binary logistic regression model, the crude odds of underweight was over 2 times high (COR: 2.28, 95% CI: 1.26-4.12, P = .006) among female children compared to male children while the adjusted estimated showed 3 times high (AOR: 3.06, 95% CI: 1.56-6.12, P = .001) (Table 3).
Factors associated with underweight among children.

Abbreviations: AOR, adjusted odds ratio; AUROCC: Area under the receiving operating characteristics curve; CI, confidence interval; COR, crude odds ratio; VIF, variance inflation factor.
In the crude model, (COR: 0.38, 95% CI: 0.21-0.67, P = .001) and 87% less among children aged 36 to 47 months (COR: 0.13, 95% CI: 0.04-0.42, P = .001). In the adjusted model, the odds of underweight was 74% less among children aged 24 to 35 months (AOR: 0.26, 95% CI: 0.13-0.51, P < .001) and 91% less among children aged 36 to 47 months (AOR: 0.09, 95% CI: 0.03-0.29, P < .001). The odds of underweight among children aged 48 to 49 months was not significantly different from children aged 11 to 23 months from both the crude and adjusted estimates (Table 3).
Although the employment status of the caregiver was not significant in the crude model, the adjusted odds of being underweight were over 2 times high among children whose caregivers were unemployed (AOR: 2.61, 95% CI: 1.15-5.93, P = .022) (Table 3).
Factors associated with stunting among children under 5 years
The proportion of stunting was slightly higher in female children (14.2%), children aged 48-59 months (22.2%), children born to mothers who were gainfully employed (20%), children born to families with a household size of 5 and above (39.2%), and among children whose breastfeeding was initiated after 1 hour after births (15.5%). Interestingly, the prevalence of stunting was higher in children who had complementary feeding (17.3%) and had it at age 6 months (16.7%). Also, stunting was higher in children who did not experience diarrhea (16.6%) than those who had diarrhea in the last 2 weeks (12.1%). The study found no statistically significant association between stunting and all the independent variables at P < .05.
Similarly in both bivariate and multiple logistic regression analysis, none of the independent variables was a significant factor for stunting. However, it was observed that the adjusted odds of stunting were much higher among children of age 24 to 35 months (AOR = 1.53, 95% CI: 0.13-18.44) and 36 to 47 months compared to children of age 11 to 23 months (AOR = 1.94, 95% CI: 0.15-25.22). Also, the likelihood of being stunted among children who had complementary feeding was 2.6 times higher than those who did not have (AOR = 2.59, 95% CI: 0.22-30.80). Children born to families with household size of 5 and above were 1.8 times more likely to be stunted compared to those born to families with household size below 5 (AOR = 1.84, 95% CI: 0.75-4.51) (Table 4).
Factors associated with stunting among children.
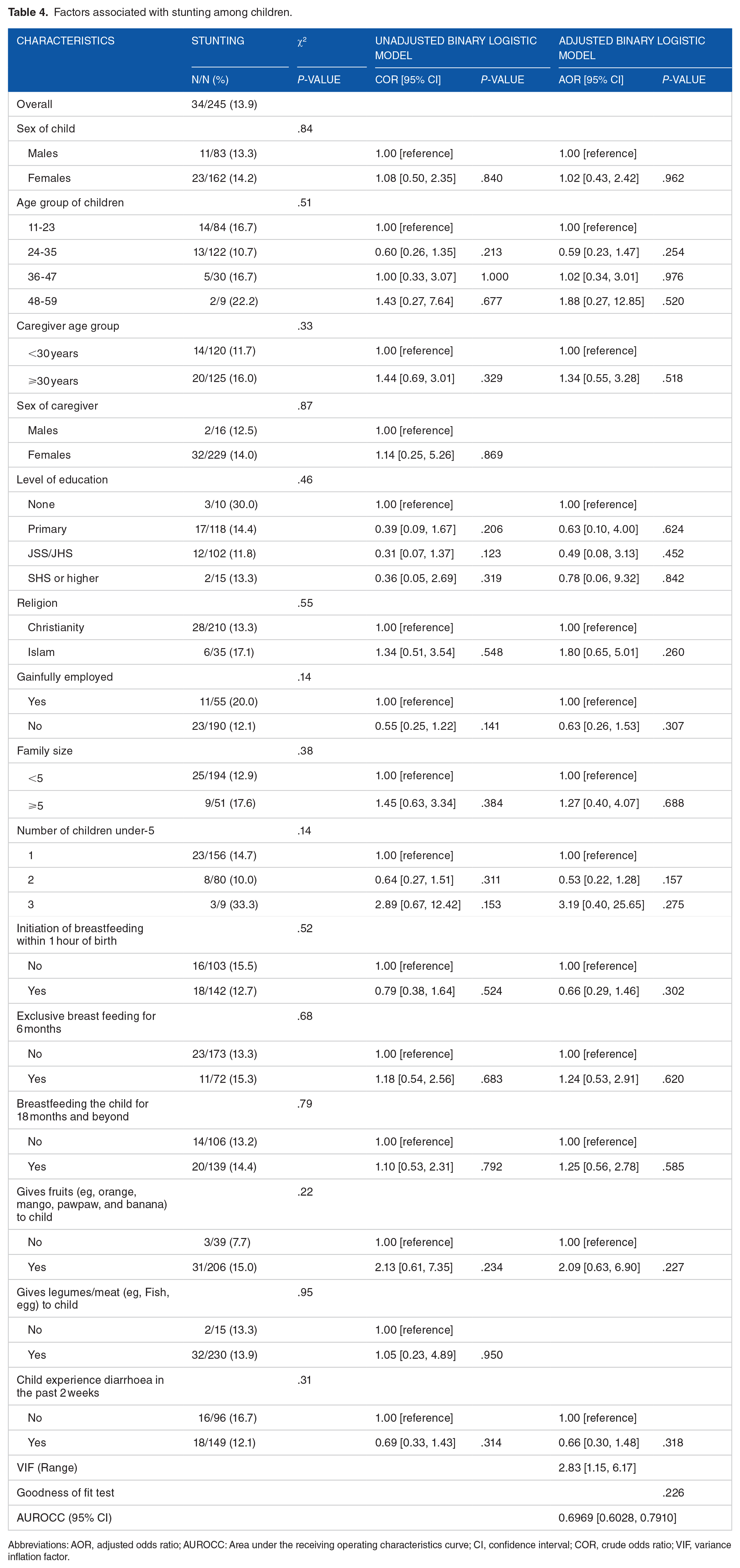
Abbreviations: AOR, adjusted odds ratio; AUROCC: Area under the receiving operating characteristics curve; CI, confidence interval; COR, crude odds ratio; VIF, variance inflation factor.
Factors associated with wasting among children under 5 years
The bivariate analysis showed that age group (P < .001) was the only factor significantly associated with underweight among children. In the crude model, the odds of underweight compared to children aged 11 to 23 months was over 18 times high among children aged 24 to 35 months (COR: 18.73, 95% CI: 6.44-54.56, P < .001), 22 times high among children aged 36 to 47 months (COR: 22.86, 95% CI: 6.64-78.71, P < .001), and 16 times high among children aged 48 to 59 months (COR: 16.00, 95% CI: 3.05-83.96, P = .001). In the adjusted model, the odds of underweight was 27 times high among children aged 24 to 35 months (AOR: 27.41, 95% CI: 9.12-82.37, P < .001), 28 times high among children aged 36 to 47 months (AOR: 28.23, 95% CI: 7.59-104.94, P < .001), and 18 times high among children aged 48 to 59 months (AOR: 18.10, 95% CI: 3.04-107.76, P = .001) (Table 5).
Factors associated with wasting among children.
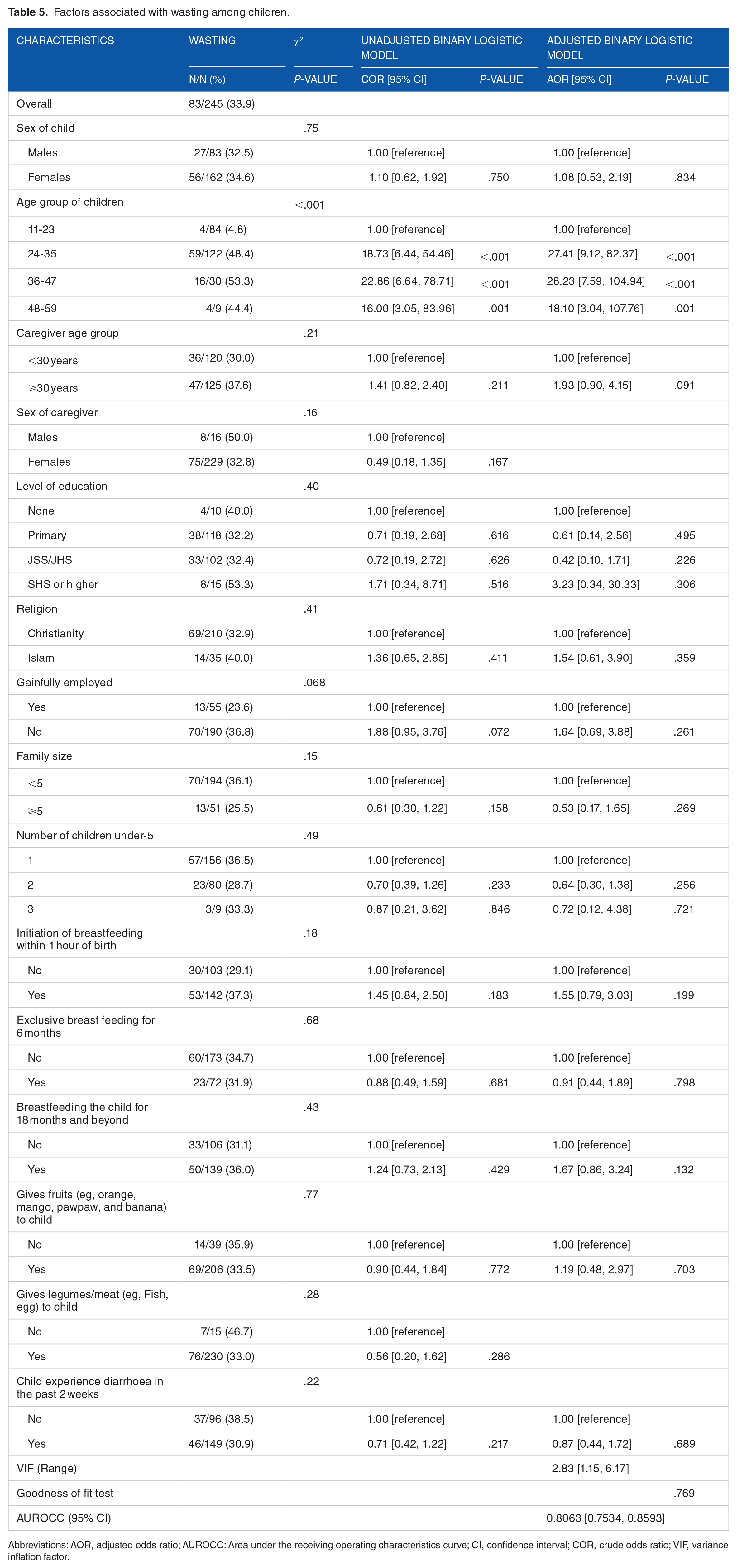
Abbreviations: AOR, adjusted odds ratio; AUROCC: Area under the receiving operating characteristics curve; CI, confidence interval; COR, crude odds ratio; VIF, variance inflation factor.
Discussion
This study sought to assess the prevalence and factors associated with 3 selected malnutrition indicators including underweight, stunting, and wasting among children below the age of 5 years visiting a health facility in the Ahafo region of Ghana. The study also descriptively assesses the perceived factors of malnutrition and knowledge among the mothers.
The analyses showed that 35.9% of children under 5 years were underweight, 13.9% stunted and 33.9% wasted; results far higher than the UNICEF 2019 Report for Ghana with averages of 13% for underweight, 18% for stunting and 7% for wasting. 2 These results provide an evidence base for relevant stakeholders and policymakers to support the development of interventions aimed at improving the nutrition and livelihoods of children under 5 years residing at Ahafo, Hwidiem.
The study findings indicated that most respondents observed that malnutrition was a multifaceted problem with a complex sequence of causation. This is consistent with the UNICEF Framework on malnutrition. Regarding the knowledge of mothers on the causes of child malnutrition, the majority of the mothers (79.2%) indicated an unbalanced diet, insufficient meals that’s less than 3 meals per day (40.9%), poor appetite (39.8%), inadequate breastfeeding within 6 months (25.8%) while few the respondents indicated that stomach/digestion (22.0%) also cause of malnutrition among children. maternal knowledge of causes of malnutrition was good, however, mothers were not aware poor hygienic condition in which food is being prepared for the child, unsafe water diseases and infections can equally cause severe malnutrition.15 -19
It has been observed that poor child-feeding practices are likely to increase the incidence of diarrhea, and fever and ARI increases the risk of children being undernourished. 18 The results showed the attitude of mothers toward breastfeeding was very good as all mothers had been practicing breastfeeding for their children. At the time of this study only 31.4% of mothers breastfeeding their child or children. More than half of these mothers initiated breastfeeding their children within 30 minutes after birth while 39.0% of the mothers’ breastfeed their children from 1 to 2 hours.
Stunting refers to a child who is too short for his or her age. Children affected by stunting can suffer severe irreversible physical and cognitive damage that accompanies stunted growth. The devastating consequences of stunting can last a lifetime and even affect the next generation. 20 According to the UNICEF, WHO and World Bank Group 2021 report, on Joint Child Malnutrition, an estimated 149.2 million children under the age of 5 suffered from stunting in 2020 worldwide. The stunting rates are decreasing in all regions worldwide, except for the African region which faces a rising number of stunted children. 4 The number of stunted children under the age of 5 years in Africa has risen from 49.7 to 57.5 million between 2000 and 2019. 4 During the same period, Southern Africa alone had reported a rise of 100 000 stunted under-5 years children.
Wasting refers to a child who is too thin for his or her height. Wasting is the result of recent rapid weight loss or the failure to gain weight. A child who is moderately or severely wasted has an increased risk of death, but treatment is possible. According to UNICEF, WHO and World Bank Group 2021 report, of the 45.4 million children under the age of 5 years who were wasted, 14.3 million were severely wasted, with over a one-third of them living in Africa.
This study reported an overall prevalence of underweight, stunting, and wasting were 35.9, 13.9, and 33.9%, respectively. The reported pattern of malnutrition is far above the global trend analysis of malnutrition subcategories in 2017 which revealed that stunting affected an estimated 22.2% of children under 5, wasting continued to threaten the lives of an estimated 7.5% of children under 5 while 5.6% children under 5 around the world were overweight. 20 The prevalence of stunting in this study was much lower than the pooled estimate of stunting for East Africa (39.0%), West Africa (31.8%), Southern Africa (30.6%), and Central Africa (28.8%) (Akombi et al 21 ). However, the estimated prevalence of underweight and wasting in this study were much higher compared to the pool estimate for East Africa (14.4 and 5.4%), for West Africa (20 and 10%), for Southern Africa (10.7 and 4.1%), and for Central Africa (12.8 and 6.7%).
Also, an evidence-based study 4 has shown that of the 149.2 million children under 5 years were stunted 36% resided in Africa 56% were found in Asia, 45.4 million were wasted and 38.9 million were overweight. The number of children with stunting is declining in all regions except Africa. Similarly, in this study stunting (13.9%) was much higher than the global estimates of 7.5%.
Regarding the associated factors of being underweight, analysis of this study indicated child’s sex, age of children, and complementary feeding were significantly associated with being underweight. It was observed that the female child was 8 times more likely to be underweight compared to their male counterpart. Further, it was also observed that the likelihood of being underweight among children aged 24 to 35 months was nearly 2 times higher than children under 24 months. Children who enjoyed any form of complementary feeding were less likely to be underweight. These findings were similar to the observation made, 22 which identified the sex of the child and pre-lacteal feeding to be significantly associated with being underweight. However, unlike this study’s findings, they also found mothers’ education and child immunization status to be significantly associated with underweight in their study population.
Conclusion
In general, mothers who participated in this study had a good knowledge and perception regarding childhood malnutrition and the study shows that the majority of mothers knew the correct causes, consequences, and preventive measures of malnutrition.
This study indicated a higher proportion of children born to mothers who participated in this study are malnourished, as the prevalence of underweight, stunting, and wasting were 35.9, 13.9, and 33.9%, respectively.
The study found that child’s sex, age of children, and complementary feeding are significant factors affecting underweight. The age of children and complementary feeding were significantly associated with wasting. However, none of the independent variables studied was significantly linked to stunting. Although, not significant children who suffered diarrhea were more likely to be wasted.