
Abstract
Objectives
To detect relative frequency of anaplastic lymphoma kinase (ALK-1) gene abnormality in diffuse large cell lymphoma (DLCL) using fluorescence in situ hybridization (FISH), and correlate its presence with clinicopathological features which may be useful for choice of therapy and predict survival in newly diagnosed cases.
Patients and Methods
A prospective study was done between March 2004 and October 2009. Fifty patients newly diagnosed with DLCL were enrolled into the study. Immunophenotyping was done and detection of ALK-1 gene abnormalities were carried out by immunohistochemically (IHC) and FISH. Patients that proved to be ALK-1 positive were treated with standard cyclophosphamide –hydroxydaunorubicin-oncovin-prednisone (CHOP) protocol.
Results
All ALK +ve patients achieved complete remission (CR) vs. 93.5% CR and 6.5% partial remission (PR) for ALK –ve patients respectively. Disease free survival (DFS) at 24 months was 81.8% in the CHOP-14 group (ALK-1−) vs. 100% for the CHOP-21 group (ALK-1+). Overall survival (OS) at 30 months was 80.4% in the CHOP-14 group vs. 100% for the CHOP-21 group.
Introduction
Diffuse large cell lymphoma (DLCL), the most common type of lymphoma in adults, can be cured by anthracycline based chemotherapy in only 35% to 40% or patients. 1 The multiple unsuccessful attempts to increase this rate suggest that diffuse large cell lymphoma is actually composed of several diseases that differ in responsiveness to chemotherapy. Support of this idea comes from a study of gene-expression profiles. 2
Eastern Cooperative Oncology Group (ECOG) performance status, age, tumor stage, lactate dehydrogenase level and the number of sites of extranodal disease have prognostic value in diffuse large cell lymphoma and they are included in the international prognostic index (IPI). Although the index is of value, it has not been used successfully to stratify patients for therapeutic trials. 3
Since the outcomes for patients within the same subgroup of DLCL varies, gene-expression profiles of DLCL could be used additionally by the IPI to predict the outcome of chemotherapy, and identification of different genes could be very helpful in the cure of the disease. 4
Chromosomal translocation t(2;5)(p23;q35) has been reported in large cell lymphoma. This translocation has been cloned and shown to result in the fusion of the nucleophosmin (NPM) gene on chromosome 5 and the anaplastic lymphoma kinase (ALK) gene on chromosome 2. This fusion results in expression of an aberrant fusion protein, NPM/ALK. Anaplastic lymphoma kinase ALK is a novel receptor tyrosine kinase (RTKs) as it has an extracellular domain, a single transmembrane domain and an intracellular domain containing the tyrosine kinase activity. 5 The nucleophosmin gene (NPM), as known as NPM, B23, numatrin, is an RNA- binding nuclear phosphoprotein of 38-kd that is completely expressed. Its cell cycle dependence function includes protein shuttling between the nucleus and the cytoplasm and thus functions as a carrier of newly synthesized protein into the nucleus. 6 When NPM immunostaining is restricted to the cell cytoplasm and not present in the nucleus, a partner other than NPM is likely to be present. 7 Recently, it has been demonstrated that ALK fusion proteins may occasionally be the result of ALK rearrangements other than NPM-ALK. Ten to twenty percent of ALKomas may thus carry ALK rearrangements other than NPM-ALK. Examples already described are t(1;2)(q25;p23) resulting in a newly identified TPM3-ALK fusion gene, t(2;3) (p23;q21) fusing the TFG and ALK genes and inv(2) (p23;q35) creating the ATIC-ALK. 8
The determination of ALK positivity is important because it denotes a significant favorable prognosis.9,10 Fluorescence in situ hybridization (FISH) is a very useful technique for detection of chromosomal abnormalities. 11 It is a highly specific and rapid test that should prove to be a useful adjunct to the currently available methods for detection of the t(2;5) (p23;q35). 12
ALK is a viable target for therapeutic intervention and its inactivation might represent a pivotal approach for the treatment of ALK lymphomas as inhibition of ALK could induce biological changes capable of inhibiting cell growth and/or promoting cell death. 13 Detailed understanding of the molecular pathogenesis of hematopoietic neoplasms might guide the development of improved therapies and can inform the design of novel therapeutic strategies.14,15
A prospective study was done between March 2004 and October 2009 at Tanta University Hospital, Mansoura Oncology Centre and International Medical Center. Informed consent was obtained from all patients before immunohistochemical and molecular techniques (FISH) were conducted to detect the relative frequency of ALK-1 gene abnormalities in DLCL and its correlation with clinicopathological features. The predictive value of ALK-1 positivity on treatment response and survival in newly diagnosed cases was also explored.
Patients and Methods
Fifty patients histopathologically diagnosed as DLCL, aged 18 to 73 years, with performance status 0–2 were enrolled into the study. Immunophenotyping for the cases was done using a panel formed of the antibodies CD20 (Dako Cat. No. M0755, clone: L26), CD3 (Dako Cat. No. M7254 clone: F7.2.38), CD15 (Dako Cat. No. M0733, clone: C3D-1) and CD30 (Dako Cat. No. M0751, clone: Ber-H2).
Detection of ALK-1 gene abnormalities by immunohistochemistry and FISH technique. Immunohistochemistry was performed by using anti-ALK-1 mononclonal antibody (Dako Cat. No. M7195, clone: C3D-1). Dako Envision staining system (Cat. No. K 4006) was used for detection of all imunohistochemical tests done.
The basic FISH procedure was carried out as described by Remstein 2000. 16 Nuclear isolation from paraffin-embedded tissue were done as followed: Two 50 μm sections were cut from each paraffin block and transferred to a 15 mL centrifuge tube. Specimens were deparaffinized with xylene (2 mL × 5 mL for 10 min each) and treated with an ethanol to water series (100%, 85%, 70%) for 10 min each. Nuclei were extracted using a 0.005% pepsin solution for 2 h at 37 °C. The specimens were vortexed vigorously for 1 min and the isolated nuclei suspension was filtered into new 15 mL centrifuge tubes using a 40 μm nylon mesh and a transfer pipette. Nuclei were pelleted by centrifugation at 1200 r.p.m. for 8 min, washed twice in 5 mL phosphate-buffered saline (PBS) and resuspended in a small volume of PBS.
Slide Preparation for FISH
One drop of cell suspension was placed on a slide and dried at 65 °C for 10 min. Slides were placed in methanol:acetic acid (3:1) for 10 min and air-dried. The slides were then heated at 90 °C for 10 min and treated with 2× standard saline citrate (SSC; 300 mmol/L sodium chloride, 30 mmol/L sodium citrate) for 15 min at 37 °C, dehydrated with an ethanol series (70%, 85%, 100% for 1 min each) and air-dried. The slides were placed in 0.1 mmol/l citric acid (pH 6.0) at 85 °C for 1 h, dehydrated with an ethanol series (70%, 85%, 100%) and air-dried. Slides were treated with a pepsin solution (0.005% pepsin in a 0.01 N HCl solution) at 37 °C for 30 min, dehydrated with an ethanol series (70%, 85%, 100%) and air-dried.
Codenaturation of the Probe and the Slide
Using the Vysis Locus Specific Identifiable (LSI) Probe (Vysis, Inc., 3100 Woodcreek Drive, Downers Grove, IL, USA, Cat. No. 32-190069). The LSI ALK dual color, break apart rearrangement probe is designed to detect the known 2p23 rearrangements that occur in t(2;5) and its variants. The t(2;5) has been shown to fuse the NPM gene located on chromosome 5q35 with the gene on chromosome 2p23. This NPM/ALK gene fusion gives rise to a chimeric protein that is over expressed. The LSI ALK dual color, break apart rearrangement probe contains two differently labeled probes on opposite sides of the breakpoint of the ALK gene. A probe of approximately 250 kb for the telomeric side of the ALK breakpoint is labeled with spectrum orange. The centromeric probe is approximately 300 kb and labeled with spectrum green. The probe was prepared according to manufacturer instruction with modification of hydride system program so that the melting temperature was 80 °C for 8 min and hybridization temperature was 37 °C overnight. Posthybridisation washes using 0.4X SSC/0.3% NP-40 wash solution at 73 °C for 2 mins and 2X SSC/0.1% NP-40 wash solution at room temperature for 2 mins. Ten μL DAPI counter stain were added at the marked area of the slide, then a clean cover slip was applied and sealed well.
Image Capture and Slide Screening
Digital images were captured using a CCD camera (Cohou) mounted on a fluorescence microscope (Olympus BX60) equipped with selective filters for fluorescein, rhodamine, and DAPI, and controlled by Applied image analysis software. At least 200 nuclei were analyzed for each hybridization. Cells with an intact ALK locus have a fused orange—green signal on chromosome 2 as shown in Figure 5. If an ALK translocation has occurred, then the probe is split. The proximal spectrum green-labeled probe remains on the der (2), and the distal spectrum orange-labeled probe moves to the partner derivative chromosome as shown in Figure 6.
Treatment Design
Group (A) patients were ALK-1 positive and were treated with a standard CHOP protocol consisting of cyclophosphamide (750 mg/m2 intravenously, doxorubicin (50 mg/m2 intravenously), vincristine (1.4 mg/m2 intravenously, maximum dose of 2 mg) on day 1, and prednisone (100 mg orally) given on days 1 to 5, the protocol recycled every 21 days (CHOP-21). Group (B) patients were ALK-1 negative and were treated with an intensified CHOP protocol consisting of cyclophosphamide (750 mg/m2 intravenously, intravenously, doxorubicin (50 mg/m2 intravenously), vincristine (1.4 mg/m2 intravenously, maximum dose of 2 mg) on day 1, and prednisone (100 mg orally) given on days 1 to 5, the protocol recycled every 14 days (CHOP-14), with the patients receiving recombinant human granulocyte colony—stimulating factors (G-CSF; filgrastim) subcutaneously if white blood cell count (WBC) less than 2.5 × 10 9 /L from days 10 to 13 at a dosage of 300 μg/day or 480 μg/day for patients less than 75 kg or 75 kg or more body weight, respectively.
Before every cycle of chemotherapy, complete clinical examination and complete hematological assessment was done (including complete blood picture, LDH, liver, kidney function and blood glucose) and toxicity was evaluated according to NCI toxicity criteria.
All the investigations done during the pretreatment period were repeated by the end of the 3rd cycle and properly assessed. The patients who achieved complete or partial remission received three additional cycles of chemotherapy. All patients received six cycles of chemotherapy. Patients with stable or progressive disease were shifted to salvage therapy.
Radiotherapy
In both groups, two weeks after the end of chemotherapy and with assurance of bone marrow recovery by normal blood picture, radiotherapy was delivered doe sites of initial bulky disease (largest diameter ≥ 7 cm), to extranodal sites wherever feasible as well as to patients presented with waldeyer's ring involvement using Cobalt-60 teletherapy machine. Radiation dose was 36 Gy delivered in 1.8 Gy daily fractions, 5 days a week. Radiotherapy fields were limited to regions of initial involvement.
Follow Up
Patients were seen weekly during treatment and then monthly in the first year, every 2 months in the second year, every 4–6 months thereafter or at any time if there was any complaint.
The follow up period ranged between 5 months and 40 months with a median of 16 months, the patients who discontinue their prescribed course of treatment or lost follow up early were excluded from the statistical analysis and survival results. Death within 4 weeks after the end of therapy from causes other than lymphoma was designated as therapy-related death. Evaluation of tumor response and end point was done according to the International Workshop criteria. 17
Statistical Analysis
Statistical presentation and analysis of the present study was conducted using the mean, standard deviation, analysis of variance [ANOVA] test, Chi-square correlation test, ROC curve, and Statistical Package for the Social Sciences (SPSS V.11). Kaplan-Meier method was used for estimating survival and log rank test to compare curves. The P value is significant at 0.05 levels. 18
Results
According to the morphologic criteria and the immunohistochemistry; studies were done using CD3, CD20, CD30 and CD15 were an essential panel for our cases. The most common cells found were B-cell (37/50) at 74.0%, versus only 26.0% of those with the T/Null phenotype. CD3 was expressed in twelve patients, CD20 was expressed in 37 cases while eleven patients were positive for CD30. Co-expression of both CD3 and CD30 was seen in 6 cases while co-expression of both CD20 and CD30 was seen in 4 cases and all patients were negative for CD15. Accordingly 6 cases were diagnosed as ALTCL (12.0%), the majority of patients (33/50) were diagnosed as DLBCL (66.0%), while 4 cases (8.0%) were of DLBCL-anaplastic variant, only one patient was diagnosed as null anaplastic and six patients (12.0%) were of peripheral T-cell, unspecified.
Anaplastic lymphoma kinase expression by immunohistochemistry was confined to (10.0%) 5 cases (4 patients with ALTCL and the only case of null anaplastic, while none of the other pathological subtypes were labeled for ALK-1 Ab). 80% of the ALK-positive cases showed the morphology of the classic or common type, any cytoplasmic or nuclear staining was considered positive, as shown in Figures 2 and 3 while ALK− cases include as shown in Figure 4. 37 (100.0%) B-phenotype and 8 (61.5%) T-phenotype. These results showed that ALK positive staining was confined to T/Null-phenotype only (38.5%).
The t(2;5)(p23;q35) chromosomal translocation and its variants were detected by FISH technique in the five T/null-ALCL cases that express ALK protein except one, which appeared as weak cytoplasmic staining by IHC (3 cases of ALTCL and the null anaplastic case).
The concordance rate between IHC staining and FISH was 80% (4/5) with 100% specificity to FISH technique (Table 1).
Concordance between methods for ALK detection.

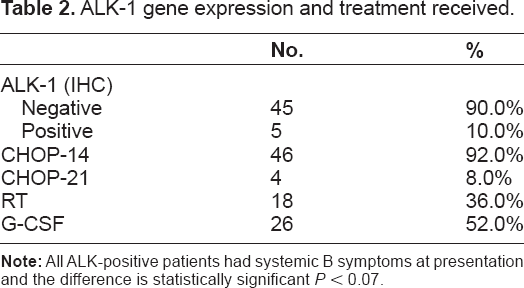
These four cases received CHOP-21 (group A), while the ALK− cases (46) received CHOP-14 (group B), in both groups eighteen patients (two cases in group A vs. sixteen in group B) received radiotherapy as a form of consolidation therapy (36 Gy/4 weeks/20 fraction). In group B, twenty-six patients received granulocyte colony stimulating factor; the maximum number used was three doses/cycle while the minimum was one/cycle (Table 2). No evident treatment delay was observed in all treatment groups as the treatment duration almost matched the planned duration.
ALK-1 gene expression and treatment received.
All ALK+ patients achieved CR vs. 93.5% CR and 6.5% partial remission (PR) for ALK− patients respectively. Hematological toxicities in the form of leucopenia and anemia were more common in CHOP-14 group. The actual estimate of DFS at 24 months was 81.8% in the CHOP-14 group (ALK-1−) vs. 100% for the CHOP-21 group (ALK-1+). The actual OS at 30 months was 80.4% in the CHOP-14 group vs. 100% for the CHOP-21 group (Table 3).
Evaluation of early response (after 3rd cycle) of treatment relevant to ALK-1 positivity.

Statistically significant differences in term of treatment outcome were found as regarding IPI and ALK-1 rearrangement (P < 0.05).
Toxicity 2ry to the drug effect are seen in Table 4 which illustrates the most frequently noticed toxicities in the both groups, (NCI CTC 1999, were used in defining the grades of toxicity). Alopecia is the most common toxicity occurring in all patients of both groups. Hematological toxicities in the form of leucopenia and anemia occurred more commonly in the CHOP-14 group, while no one was affected by thrombocytopenia in either group. Infection only occurred in the CHOP-14 group (7 cases) which is usually associated with neutropenia and systemic fungal infection with systemic use of antibiotic, antifungal and growth factors. In the CHOP-21 group, gastrointestinal toxicities include N/V, diarrhea and mucosities occurring in 75%, 25% and 25% vs. 89.1%, 8.7% and 21.7% in the CHOP-14 group respectively. No cardiac or lung toxicities were detected in either group.
Toxicities according to treatment arms.
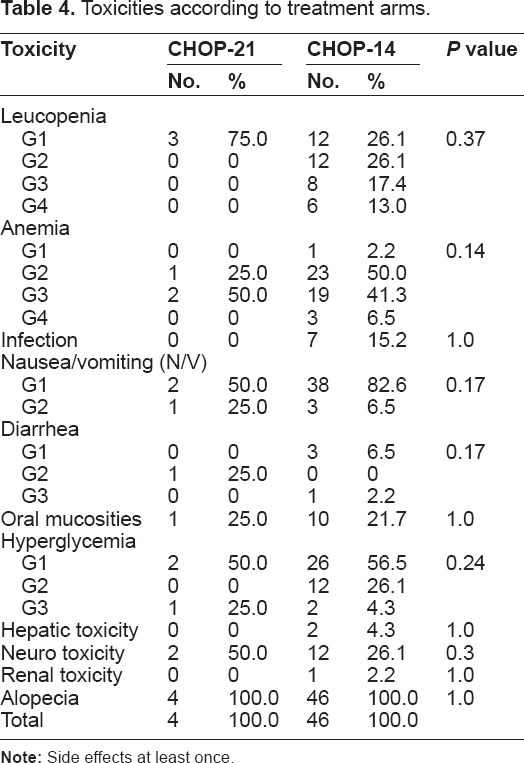
There were three cases with therapy associated deaths (toxic deaths), all in CHOP-14 group. Two cases had documented septicemia with G4 neutropenia while the third one fell into a coma with unknown etiology and died. In the CHOP-14 arm, six patients relapsed vs. none in the CHOP-21 arm. All relapsed patients received second line salvage chemotherapy.
Disease Free Survival
The actual estimate of DFS at 24 months was 81.8% in the CHOP-14 group (ALK-1−) vs. 100% for the CHOP-21 group (ALK-1+), however no statistically significant difference was found between the two groups (P = 0.45).
Overall Survival
The actual OS at 30 months was 80.4% in the CHOP-14 group (ALK-1−) vs. 100% for the CHOP-21 group (ALK-1+), however no statistically significant difference was found between the two groups (P = 0.48) (Figure 1).

Overall survival of both groups.

A case of anaplastic large T-cell lymphoma positive for ALK-1 antibody with membranous and cytolplasmic expression.

A case of anaplastic large T-cell lymphoma positive for ALK-1 antibody with nuclear and cytolplasmic expression.

A case of anaplastic large T-cell lymphoma negative for ALK-1 antibody.

Normal interphase shows an intact ALK loci have a fused orange-green signals in both normal chromosome 2.

ALK split-apart FISH probe shows split orange and green signals, the proximal spectrum green-labeled probe remains on the derivative chromosome 2, and the distal spectrum orange-labeled probe moves to the partner derivative chromosome, intact ALK locus have a fused orange-green on chromosome 2.
Discussion
The biologic insights provided by molecular studies should allow for more targeted therapies to be developed, which will increase treatment choice and the possibility of tailored therapy in the future. 19
The NPM/ALK is an oncogenic fusion protein expressed in about 50% of ALCL cases, and has emerged as a novel tumorigenic player in several human cancers. 20
This protein derives from the t(2;5)(p23;q35) chromosomal translocation that fuses the catalytic domain of the tyrosine kinase, anaplastic lymphoma kinase, with the dimerization domain of nucleophosmin protein. 21 It promotes tumorigenesis through its functional and physical interactions with various biologically important proteins. The identification of these interacting proteins has proven to be useful to further our understanding of NPM-ALK-mediated tumorigenesis. ALK-positive neoplasms represent a distinct entity. Because their morphology is often neither anaplastic nor large cell, it was suggested that they should hence forth be referred to as ALK lymphomas.9,22
The present study was designed to evaluate dose dense CHOP regimen (every 2 weeks) and CHOP regimen (every 3 weeks) in ALK-negative and ALK-positive DLCL patients within the age range of 18–73 years in order to identify which treatment regimen could be associated with a better outcome and reduced toxicity irrespective of age stratification.
Among the fifty patients included in the current study, ages ranging from 18–73 years with a median age of 52.00 years, similar findings were reported by Egyptian investigators.23,24 This pattern was different in western countries, where in an American study, the median age of NHL patients was 65 years. 25 This difference in age distribution could be explained by the population structure in Egypt where the mean life span is less than in western countries.
Of the patients included in the study, 58.0% were male while 42.0% were female. As in most other series, male predominance was shown in this study, with males to female ratio of 1.4:1 which is similar to that reported by Pulford et al 26 and Wunderlich et al. 27 However, it was lower than reported by Egyptian authors 1.8:1, 1.9:1 and 2.8:1,23,28,29 while in western countries it was 1.6:1. 30
Serum LDH was above normal in 48% of our patients. This was in agreement with the results of Wunderlich et al. 27 As in most other series, B-phenotype predominance was shown in this study (74.0%) vs. 26.0% of cases with T/Null-cell phenotype and this is similar to that reported by Itoh et al. 31 However it was lower than reported by Pfreundschuh et al. 32
The majority of patients (70%) had good PS (0–1) and 30% had bad PS (2). Systemic B symptoms were encountered at the onset of disease in 40% of patients, this is in agreement with that reported by Itoh et al. 31
In the present study, extranodal presentation represent only 10% of cases which is lower than that reported by Pulford et al 26 and Wunderlich et al 27 where extranodal disease represented 38% and 31% respectively.
Bone marrow involvement was encountered in 10% of cases. This is in agreement with Pfreundschuh et al 33 who reported incidence of 11.6% with bone marrow involvement. On the other hand, our figures are lower than reported by Wunderlich et al 27 where 19% suffered from bone marrow involvement.
A total of 50 cases were analyzed for expression of ALK protein by immunohistochemistry staining with ALK-1 Ab. Five out of fifty cases (10%) were found to be ALK-1 positive by IHC, they constitute 4/6 ALTCL (66.6%) and the case with anaplastic null large cell phenotype. This was consistence with Falini et al 34 Gascoyne et al 35 Drexler et al 36 Savage et al 37 EL Sawi, 38 Rizvi et al 39 and Falini et al 40 whom found that 50%–75% of ALCL cases express ALK protein.
About 80% of the ALK-positive cases showed the morphology of the classic or common type, this was similar to that reported by Liang et al. 41 However all DLBCL cases were negative for ALK-1 immunostaining. These were in accordance with the results obtained by Benharroch et al 22 and Colleoni et al 42 who didn't find ALK protein in DLBCL. On the contrary, Kadin and Moris, 43 and Kutok and Aster, 44 found that some DLBCL express ALK protein. In addition, Gascoyne et al 45 describes 6 cases of ALK positive DLBCL, while Lee et al 46 reported three cases and Beltran et al 47 reported four cases.
ALK protein expression by immunohistochemical staining displayed a combined nuclear and cytoplasmic pattern in three cases. In one case, this suggests NPM-ALK fusion, cytoplasmic and membranous stain. In another case, it suggests fusion to a variant partner gene, as the staining was restricted to the cytoplasm. This is in agreement with reports by Benharroch et al 22 Falini et al 48 and Liang et al. 41
Five cases (10.0%) were found to be ALK positive by IHC while ALK abnormalities were detected by FISH technique in four of them. The negative case by FISH technique was the situation where ALK protein was expressed weakly in the cytoplasm. This may be attributed to technical problem which lead to false positive staining of the cytoplasm, as formalin stain due to issues with fixation lead to formalin precipitation.
Both ALK-1 immunostaining and FISH detection of t(2;5) could be used as a marker for ALK-positive cases however FISH technique is a more specific parameter for discrimination. This is in agreement with Mathew et al 49 Drexler et al 36 Cessna et al 50 Paternoster et al 51 and Cataldo et al. 52 Contrary to our results, Fan and Rizkalla 53 reported that immunohistochemical studies using antibody ALK-1 and FISH for ALK gene rearrangement, are equally effective for identifying patients with ALCL irrespective to variant translocations.
Analysis of the clinicopathological features of the ALK-positive group versus the ALK-negative group revealed some differences; ALK-1 positive cases were common in younger ages while ALK-negative patients tended to be older, confirming the results of Falini et al 34 Leoncini et al; 54 Fan et al 55 and Rizvi et al 39 who found ALK-positive cases mainly in young patients. All ALK positive cases had B symptoms which in agreement with Rizvi et al. 39
In the current study, three ALK+ patients were with early stages, while those with stage III and IV represent 25% of positive cases vs. 32% of ALK− cases which is lower than reported by Kutok and Aster; 44 Rizvi et al. 39 This difference may be due to small sample size.
Serum LDH was high in all ALK-positive patients. This was higher than reported by Gascoyne et al 35 and Weisenburger et al 56 whom found high serum LDH in 31% and 45% respectively.
The majority of ALK-positive and ALK-negative patients fell into the low risk IPI group. However, the remainder had an IPI score of >2. This is in comparable with other series Savage et al. 37
Concerning phenotype in DLCL cases, there is highly significant difference found between ALK-1 abnormalities and cell lineage of DLCL cases, where all ALK-positive cases were limited to T/null-ALCL, and all B-phenotype were ALK-1 negative. These results were similar to those obtained by Colleoni et al 57 and EL Sawi 38 who noted that all ALK positive cases were of T-phenotype and none was of B- phenotype. On the contrary, Gascoyne et al 35 and Drexler et al 36 found that 8%–14% of ALCL-B phenotype express ALK protein.
The four ALK-positive cases received CHOP-21 while the ALK− cases (46) received CHOP-14.
All patients in group A attained complete remission (100.0%), compared to 93.5% CR, and 6.5% PR in group B, (P = 0.77). In the CHOP-14 arm, the CR rate (93.5%) is higher than the reported one in the German study, Pfreundschuh et al 58 (CR:79% in NHL-B1 trial, and CR:76% in NHL-B2 trial), however, two trials by Pronzato et al 59 and Itoh et al 31 in phase II studies showed inferior results (CR:40% and 60% respectively). Regarding the overall response, published data by Gregory et al 60 reported overall response of 89%, but with lower CR rate of 43%.
In the CHOP-21 arm, the CR rate (100.0%) is better than the reported one in the German study, Pfreundschuh et al32,58 (CR:80% in NHL-B1 trial, and CR:60% in NHL-B2 trial).
These results could be attributed to different inclusion criteria, non stratified age limit, small sample size and specificity of DLCL subtypes as well as selection of 3-week or 2-week CHOP scheme according to ALK-1 gene rearrangement.
In the present study, the actuarial estimate of disease free survival at 2 years was 81.8% vs. 100% for the CHOP-14 and CHOP-21 respectively, with no statistically significant difference between the two groups (P = 0.4).
In the CHOP-14 arm, DFS of 81.8% better than DFS of 43%, 52%, 58%, and 44% reported by Itoh et al 31 Gregory et al 60 and Pfreundschuh et al 58 (B1 and B2) respectively. In the CHOP-21 arm, published data by Pfreundschuh et al 58 showed DFS of 69% in B1 trial, and only 41% in B2 trial, both results were highly inferior to our results.
The actuarial estimate of overall survival at 30 months was 100% vs. 80.4% for the group A and group B, however no statistically significant difference was found between the two groups (P = 0.48).
In the CHOP-14 arm, OS (80.4%) was better than those reported by the Japanese study (42%) and the German study B2 trial (53%), as well as when compared to the data published by Gregory et al 60 (OS of 77%) and OS of the German study B1 trial (84%). In the CHOP-21 arm, OS (100%) was higher than those showed by Pfreundschuh et al32,58 in B1 trial (80%), and NHL B2 trial (46%).
These results of disease free survival and overall survival should be analyzed carefully as these trials have different patient populations with different characteristics. In addition the median follow up duration varies between different trials. For example, Itoh et al 31 had a follow up duration of 3 years while Gregory et al 60 used 1.7 years and Pfreundschuh et al 58 5 years. Longer follow up in this study may affect the result comparability. All patients in group A attained complete remission (100.0%), compared to 93.5% CR, and 6.5% PR in group B, (P = 0.77).
Immunohistochemical detection of ALK-1 rearrangement is a good negative test, but its postivity needs confirmation by the FISH technique especially if it affects the treatment strategy. The current outcome in ALK-positive disease is favorable with standard CHOP regimen while intensified CHOP regimen is well tolerated for ALK negative patients. This offers a better outcome and is associated with low morbidity and mortality.
The four ALK-positive cases received CHOP-21 while the ALK negative cases (46) received CHOP-14. These are in keeping with most other series who reported that patients with ALK-positive ALCL should be treated with standard CHOP chemotherapy (CHOP-21) as it is expected to have a better outcome. This may be due to the fact that ALK-positive cases are associated with younger aged patients, which could influence survival. ALK-positive cases are also associated with higher proliferation and with higher mitotic activity thus making them more responsive to treatment. Kutok and Aster 44 reported, however, that a relatively young age at presentation may not account for the favorable outcome of ALK+ ALCL, as age was not an independent prognostic indicator in multivariate analyses. Accumulated data, as presented in numerous studies, strongly suggests that standard CHOP is an inadequate therapy for most individuals with ALK-negative large cell lymphoma.37,61
In addition to such well-known factors as a normal serum LDH and an IPI score of ≤3, ALK protein expression by the tumor cells is an independent prognostic factor that predicts a favorable clinical outcome. Aberrant ALD expression is critical in the definition of DLCL as a disease entity, and we believe that the inclusion of this biologic marker as a diagnostic criterion further efines this heterogeneous category. Therefore, we suggest that larger studies be performed to accurately evaluate the frequency and types of ALK gene rearrangement in Egyptian patients with DLCL.
Our improved understanding of the molecular pathogenesis of ALK+ ALCL promises to lead to more specific, effective, and less toxic therapies. Lessons learned in the treatment of other neoplasms with tyrosine kinas inhibitors, in combination with other new drugs targeting cyclin/cdk signaling 62 are likely to be applied to the treatment of ALK+ ALCL in the future. This strategy is even more promising in ALK-positive malignancies.
Conclusions
ALK protein expression by the tumor cells is an independent prognostic factor that predicts a favorable clinical outcome with standard CHOP regimen. The FISH is powerful technique for detection of nucleophosmin (NPM)-ALK rearrangement.
Author Contributions
All the authors shared the study design, data collection and literatureresearch. El-Sebaaie A was responsible for performing the IHC. Abdou S and Shahin D were responsible for performing Immunophenotyping, FISH and helped in writing the initial version of the manuscript and in the statistical analysis. Salem H. helped in data collection and literature research, and writing the initial version of the manuscript. Korashy L, Sherif F, El-Zawahry H, Farrag W. and Abdel-Khalik O. assembled the patients’ cohorts, treatment design, coordinated clinical data collection, critically revised the statistical analysis of the clinical results and wrote the final version of the manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
The authors have read and confirmed their agreement with the ICMJE author ship and conflict of interest criteria. All the authors of this paper report no conflicts of interest. All the authors of this paper confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material.