
Abstract
Colorectal cancer is the third most common cancer in the US. In recent decades, an improved understanding of the role of the angiogenesis pathway in colorectal cancer has led to advancements in treatment. Bevacizumab has been shown to improve the progression-free survival and overall survival when combined with cytotoxic chemotherapy in patients with metastatic colorectal cancer, and at present is the only antiangiogenesis agent approved for the treatment of this cancer. Aflibercept is a novel angiogenesis-targeting agent, and has demonstrated efficacy in treating metastatic colorectal cancer in a recent randomized Phase III trial. Here we review the role of angiogenesis in the tumorigenesis of colorectal cancer, strategies for targeting angiogenesis, and the clinical development of aflibercept.
Introduction
In the US, colorectal cancer is the third most common cancer in both men and women and the second most common cause of cancer mortality in both genders combined. 1 In 2011, it accounted for approximately 140,000 new cancer diagnoses and 50,000 deaths in the US alone. 1 Worldwide, more than 1.2 million new cases, and more than 600,000 deaths was attributed to colorectal cancer at the same time. 2 Therefore, colorectal cancer is a prominent global health problem. Approximately 60% of colorectal cancer cases are diagnosed at the locally advanced or metastatic stage. 3 Metastatic colorectal cancer carries a poor prognosis, with a 5-year survival rate of approximately 12%. 3 Over the past two decades, there have been significant advances in the treatment of metastatic colorectal cancer, one of which is the development of agents that target angiogenesis. Incorporation of these anti-angiogenic agents into clinical practice has led to improvements in progression-free survival and overall survival in metastatic colorectal cancer. 4 In this paper, we will review the rationale and recent progress in targeting angiogenesis in metastatic colorectal cancer, with a special focus on the novel antiangiogenesis agent, aflibercept.
Angiogenesis and Tumorigenesis
Angiogenesis is the process of new blood vessel formation. Blood vessels are needed for the supply of nutrients and oxygen and the disposal of waste products, and therefore angiogenesis is essential in the growth and development of normal tissues as well as tumors. It is widely accepted that tumors are unable to grow beyond 2–3 mm without blood vessels in vivo.5,6 Since 1971, when Folkman observed the importance of angiogenesis in tumorigenesis, and predicted that “antiangiogenesis may provide a form of cancer therapy worthy of serious exploration”, angiogenesis has generated intense research interest. 5
Angiogenesis is a highly regulated and complex process involving a variety of proangiogenic and anti-angiogenic factors and multiple signaling pathways that intertwine and regulate each other. In a healthy individual, there is a delicate balance between proangiogenesis and antiangiogenesis. However, as a tumor develops, it often outgrows its vascular supply, thus producing a hypoxic environment. Hypoxia switches on the hypoxia-inducible factor-1 alpha system, which stimulates the production of proangiogenic factors in excess of antiangiogenic factors, or the so-called “angiogenic switch” phenomenon, leading to pathological angiogenesis.7,8 One of the main proangiogenic pathways is mediated by the vascular endothelial growth factor (VEGF) family, composed of six growth factors (VEGF-A, VEGF-B, VEGF-C, VEGF-D, VEGF-E, and placenta growth factor) and three receptors (VEGFR-1, VEGFR-2, and VEGFR-3). 8
The VEGF receptors are members of the transmembrane tyrosine kinase receptor family. Each VEGF receptor is composed of several crucial domains, ie, the immunoglobulin-like, ligand-binding extramembrane domain, the transmembrane domain, the juxtamembrane domain, and the intracellular tyrosine kinase domain (see Fig. 1, modified from figures by Salmon et al, 8 Cross et al, 9 and Kerbel 10 ). Circulating VEGFs bind to the corresponding receptors, and activate the dimerization of the receptors. Upon dimerization, the receptors undergo conformational changes that expose ATP binding sites on the intracellular kinase domains, resulting in autophosphorylation of the tyrosine residues of the domains and activation of a cascade of downstream signaling transduction pathways.
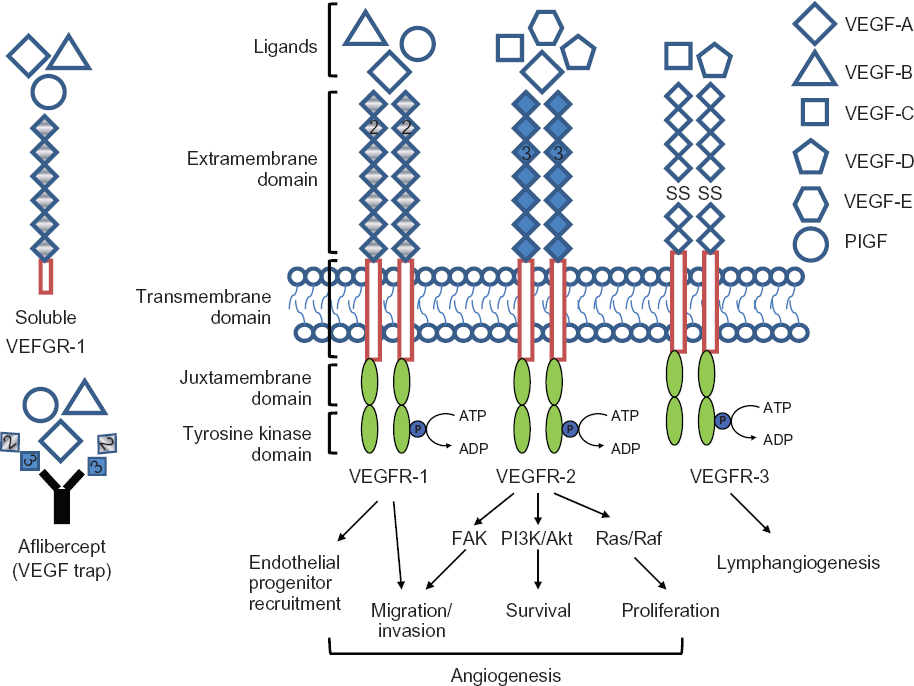
Schematic illustration of the family of veGF receptors, ligands and their functions. There are six veGF ligands, veGF-A, veGF-B, veGF-C, veGF-D, VEGF-E, and PIGF and three main VEGF receptors, VEGFR-1, VEGFR-2, and VEGFR-3. Each VEGF ligand has specific affinity to different receptors as illustrated. Binding of ligands to the extramembrane domain of the receptors trigger dimerization of the receptor, autophosphorylation of the tyrosine kinase domain of the receptor, and initiate multiple downstream signal transduction pathways that result in endothelial cell proliferation, migration, survival, and more. (The figure is modified from Salmon, 8 Cross, 9 and Kerbel 10 ).
The function of VEGFR-1 is not yet fully defined. Even though VEGFR-1 has at least 10 times stronger affinity for VEGF-A compared with VEGFR-2, its kinase activity is weak. 11 VEGFR-1 knockout mice die in utero due to increased vascular proliferation and disorganization. 12 However, embryos lacking purely the tyrosine kinase domain of VEGFR-1 can survive with normal vasculature development. 13 These findings indicate that VEGFR-1 serves to sequester VEGF-A and negatively regulates the functions of VEGFR-2 pathways. 14 On the other hand, recent research has further identified additional roles for VEGFR-1. It has been found to be important in promoting angiogenesis and the migration of hematopoietic stem cells. 15 Therefore, the exact role of VEFGR-1 remains unclear and needs further investigation.
The interaction between VEGFR-2 and VEGF-A is the best characterized ligand-receptor relationship in the angiogenesis process. Their interaction initiates a variety of downstream signaling pathways, resulting in endothelial cell proliferation, differentiation, migration, invasion, survival, and increased endothelial permeability, leading to the sprouting of new blood vessels.14,15
Deletion of the VEGFR-2 gene is not compatible with life, given that all knockout mice die in utero with severe blood vessel deficiencies. 16 On the other hand, the ligand-receptor interactions between VEGFR-3 and VEGF-C and VEGF-D appear to be the most important for the formation and migration of the lymphoendothelial system. Mutations in VEGFR-3 are identified in rare cases of congenital hereditary lymphedema in humans. 17 Elevated levels of VEGFR-3 and its ligands are found in multiple types of tumors, and are associated with lymph node metastasis. 18
Angiogenesis and Colon Cancer
Studies have shown markedly increased expression of VEGF and vascular density in primary colon tumor that was associated with metastasis compared with that without metastasis or benign adenoma. 19 It was also found that the invasive edge of the colon tumor tissue contained significantly higher vascular density than other areas within the tumor. 19 These observations all indicate that VEGF expression is crucial in tumor metastasis. VEGF expression is also correlated with higher risk of tumor recurrence.19,20 Other studies have suggested a potential role for VEGF expression as a prognostic factor and could therefore identify high-risk patients who might benefit from adjuvant chemotherapy in otherwise ambivalent clinical scenarios. 21 Prospective studies are needed to explore and validate these findings further. Given that enhanced angiogenesis has been consistently associated with poor outcomes in colorectal cancer, targeting angiogenesis was thought to be a good treatment approach.
Targeting Angiogenesis in Colon Cancer
A variety of strategies have been investigated to exploit the role of the VEGF pathway in colorectal cancer. To date, the most successful agent has been bevacizumab, a humanized monoclonal antibody that binds to VEGF-A and prevents interaction between VEGF-A and VEGFR. Another targeting strategy is to use small molecular tyrosine kinase inhibitors, such as sunitinib and sorafenib, which bind to the intracellular kinase domain of the receptor and interfere with its tyrosine kinase activities essential for downstream signaling. Additional monoclonal antibodies against the extracellular domains of VEGFRs are also under development. Furthermore, agents against VEGF messenger RNAs, endogenous antiangiogenic factors angiostatin and endostatin, and endothelial tubulin disruption agents, as well as others are all under active investigation at various stages of clinical development. 8
Bevacizumab is currently the only agent approved by the US Food and Drug Administration (FDA) specifically targeting the VEGF pathway for the treatment of colorectal cancer. It improves progression-free survival and overall survival when given to patients with metastatic colorectal cancer in combination with cytotoxic chemotherapy. 4 It is usually administrated in combination with the FOLFOX (5-fluorouracil, leucovorin, and oxaliplatin) or FOLFIRI (5-fluorouracil, leucovorin, and irinotecan) chemotherapy regimens, and is therefore approved for use in this setting.4,22,23 Agents inhibiting angiogenesis provide different mechanisms and toxicity profiles from traditional chemotherapy; hence, the approach of combining angiogenesis inhibitors with chemotherapy to achieve better disease control without an increase in toxicity has been widely adopted. However, even with bevacizumab, the median progression-free survival of metastatic colorectal cancer patients remains less than one year, with median overall survival being approximately 2 years.4,24 Therefore, improving the response rate, response durability, and survival with new targeted agents remains an area of active investigation. Aflibercept (Sanofiaventis and Regeneron Pharmaceuticals Inc) is a new agent targeting the VEGF pathway. Aflibercept has recently been shown to be well tolerated and effective in treating patients with metastatic colorectal cancer when combined with cytotoxic chemotherapy. 25 In the second part of this review, we will summarize the use of aflibercept in the treatment of metastatic colorectal cancer.
Small molecule tyrosine kinase inhibitors block the tyrosine kinase activities of VEGF receptors, thus preventing phosphorylation of signaling proteins in the downstream pathway. Multiple tyrosine kinase inhibitors have been developed, among which sunitinib and sorafenib have been approved by the FDA for the treatment of metastatic renal and hepatic cancer.26–28 More tyrosine kinase inhibitors are under active investigation. No tyrosine kinase inhibitors have yet been approved for the treatment of colorectal cancer. In large Phase III trials, vatalanib, a tyrosine kinase inhibitor for all three VEGFRs, was compared with placebo when combined with FOLFOX in both first-line and second-line settings (CONFIRM 1 and CONFIRM 2, respectively). Surprisingly, the primary endpoints were not achieved in either trial (progression-free survival in CONFIRM 1 and overall survival in CONFIRM 2).29,30 Ongoing Phase I or II trials are investigating the efficacy of other tyrosine kinase inhibitors in colorectal cancer. It is worth noting that the majority of tyrosine kinase inhibitors target multiple different receptor tyrosine kinases given their structural similarity, leading to desired and undesired “off-target” effects.
Given that antibodies against VEGF ligands have been proven to be effective in treating metastatic colorectal cancer, antibodies against VEGF receptors are also of great interest. Preclinical studies have demonstrated the efficacy of a VEGFR-2 antibody in inhibiting tumor growth, angiogenesis, metastasis, and tumor cell survival.31,32 To date, only one Phase I trial has been published investigating a fully humanized monoclonal antibody against VEGFR-2, ramucirumab (IMC-1121B). 33 It was well tolerated without significant toxicity in this small study. Phase II and III studies are ongoing to incorporate ramucirumab in the treatment of a variety of malignancies, including colorectal, liver, kidney, prostate, ovarian, malignant melanoma, and nonsmall cell lung cancer. 34
Combining angiogenesis-targeting agents with cytotoxic chemotherapy not only provides the advantage of nonoverlapping toxicity and therefore good tolerance, but also serves to enhance efficacy. The mechanism of increased efficacy with combination therapy has been explored. Experimental models have demonstrated that tumors have disorganized vasculature and lymphatics, leading to increased interstitial fluid pressure and poor delivery of cytotoxic chemotherapy and hypoxia, thereby providing resistance to chemotherapy and radiation. Jain et al, as well as other investigators, have shown that with anti-VEGF agents, the disorganized and inefficient vasculature can be corrected. 35 Therefore, the delivery of chemotherapy and even radiation is improved, as demonstrated by Willett et al.35,36
Table 1 contains a list of VEGF targeted agents currently approved by the FDA. Aflibercept is also included for comparison, although it has not been approved by the FDA. Their approved treatment indications and their usage in colorectal cancer are highlighted.
Summary of FDA approved VEGF targeting agents in oncology and their use in colorectal cancer.

The approval of bevacizumab in MBC is currently under review.
Clinical Trials with Aflibercept in Colorectal Cancer
Pharmacodynamics and pharmacokinetics
Aflibercept (VEGF trap) is a fully humanized recombinant fusion protein composed of the extracellular domain 2 from VEGFR-1, the extracellular domain 3 from VEGFR-2, and the constant region of human immunoglobulin G1. It functions as a decoy VEGF receptor, binds VEGF-A, VEGF-B, and placental growth factors 1 and 2 with high affinity, prevents their binding to native VEGF receptors, and therefore inhibits angiogenesis. In vitro, aflibercept is able to block VEGF-induced phosphorylation of VEGFR-2 and VEGF-mediated cell proliferation completely. 37 In vivo, VEGF trap significantly inhibits the growth of various tumors (including melanoma, rhabdomyosarcoma, glioma, and neuroblastoma), and tumor-associated angiogenesis in mouse xenograft models. 38 In neuroblastoma cells, it was found that one of the main mechanisms of resistance to angiogenesis inhibitors is the co-option of blood vessels from the host. 38 High-dose aflibercept can overcome this resistance by causing regression of the co-opted host vessels and providing near-complete blockage of angiogenesis. This same effect is not seen with bevacizumab or low-dose aflibercept. In preclinical assessments, aflibercept results in stronger angiogenesis inhibition than does bevacizumab for several reasons, ie, at least 100–1000 times higher affinity to the circulating VEGFs, longer half-life, and added affinity to the placental growth factors 1 and 2. 38 Table 2 is a summary of aflibercept trials in patients with metastatic colorectal cancer. Some of these pivotal trials are discussed in detail.
Summary of clinical trials of aflibercept in metastatic colorectal cancer.

7 out of 47 patients received aflibercept had colorectal cancer
23 out of 38 patients received aflibercept had colorectal cancer
total number of patients in the trial, number of patients received aflibercept is unknown
614 out of 1226 patients received aflibercept, other patients received placebo.
Phase I Clinical Studies
The first Phase I study, published by Lockhart et al, aimed to evaluate the safety, pharmacokinetics, and pharmacodynamics of intravenously administered single-agent aflibercept. 39 Forty-seven patients with a variety of refractory solid tumors received aflibercept on study, of whom seven had colorectal cancer. Aflibercept was given in escalating doses from 0.3 to 7.0 mg/kg intravenously every 2 weeks. The half-life of aflibercept was observed to increase with dose escalation, ranging from 1.7 (0.3 mg/kg cohort) to 7.4 days (5.0 mg/kg cohort). Steady-state was not reached until at least 3 weeks after the first dose of aflibercept. No antibodies against aflibercept were detected. Bound aflibercept levels (aflibercept bound to circulating VEGF) reached a maximum at the dose of 2 mg/kg, and free aflibercept levels were consistently exceeding the bound levels beyond this dose, indicating saturation and blockage of VEGF ligands at doses ≥2 mg/kg. Additionally, higher doses resulted in increasing toxicity. Therefore, 4 mg/kg was determined to be the recommended dose for the Phase II and III combination studies.
In this Phase I study, antitumor responses were observed in four patients. 39 One patient with malignant thymoma and two patients with ovarian cancer had confirmed partial responses by RECIST criteria. One other patient with ovarian cancer had an unconfirmed partial response. Additionally, two patients with renal cell cancer had stable disease for more than one year.
Aflibercept was well tolerated. The dose-limiting toxicities were proteinuria and rectal ulceration observed at the dose of 7 mg/kg. 39 The most common adverse effects were fatigue (63.8%), nausea (36.2%), and vomiting (27.7%), while the most common toxicities included dysphonia (46.8%), hypertension (38.3%), and proteinuria (10.6%). Adverse events were generally mild and reversible upon aflibercept discontinuation or initiation of appropriate supportive care, such as antihypertensives. The median onset of hypertension was 3.5 days and that of proteinuria was 15 days.
Multiple other Phase I trials have demonstrated the safety of combining aflibercept with cytotoxic chemotherapy typically used for metastatic colorectal cancer, such as FOLFOX and ILV5FU2 (5-fluorouracil, leucovorin, and irinotecan). Other chemotherapies such as docetaxel, gemcitabine, pemetrexed, cisplatin, and temozolomide have also been combined with aflibercept with good safety and tolerability.6,40,41
Phase II Clinical Studies
A multicenter, open-label, Phase II trial investigated aflibercept in patients with previously treated metastatic colorectal cancer. 42 The preliminary results from this study were reported at the 2008 American Society of Clinical Oncology annual meeting. Fifty-one patients were enrolled in two cohorts, ie, bevacizumab-naïve (n = 24) or bevacizumab-treated (n = 27). Single-agent aflibercept was given at the dose of 4 mg/kg intravenously every 2 weeks. The primary endpoints were disease response rate and 4-month progression-free survival. The disease control rate (including partial response and stable disease) was 29% in bevacizumab-naïve and 30% in bevacizumab-treated cohorts, with median progression-free survival of 2.0 months and 3.4 months, respectively. The most common adverse reactions were fatigue (78%), hypertension (55%), proteinuria (49%), and headache (43%). The authors concluded that aflibercept was well tolerated and had modest activity against refractory/relapsed metastatic colorectal cancer as a single agent, regardless of prior therapy with bevacizumab.
Many other ongoing Phase II trials have found aflibercept to be safe and well tolerated in a variety of solid tumors, including nonsmall cell lung cancer, ovarian cancer, gynecologic soft tissue sarcoma, transitional cell carcinoma, melanoma, and malignant glioblastoma. 43
Phase III Clinical Studies
VELOUR is a multicenter, randomized, placebo-controlled Phase III trial, with the goal of comparing the efficacy of aflibercept versus placebo in combination with the FOLFIRI regimen as a second-line treatment for patients with metastatic colorectal cancer previously treated with oxaliplatin. 25 Enrolled patients included patients with metastatic colorectal cancer, Eastern Cooperative Oncology Group performance status 0–2, and adequate organ function after failing one oxaliplatin-based therapy. From November 2007 to March 2010, 1226 patients were enrolled, with a median age of 61 years; 58.6% were male, 97.9% of patients had a good performance status (0–1), and 30.4% of patients had received bevacizumab previously. Patients were randomized to receive FOLFIRI and aflibercept at 4 mg/kg intravenously every 2 weeks (n = 614) versus FOLFIRI and placebo (n = 612), with stratification by performance status and prior bevacizumab. The primary endpoint was overall survival, while the secondary endpoints included progression-free survival, overall response rate, safety, and aflibercept pharmacokinetics and immunogenicity. The final data collection for primary outcomes was recently completed and presented at the 2011 meeting of the European Society for Medical Oncology World Congress on Gastrointestinal Cancer.
After a median follow-up of 22.28 months, the aflibercept group showed superior median overall survival (13.50 months versus 12.06 months, hazards ratio 0.817, P = 0.0032) and progression-free survival (6.90 months versus 4.67 months, hazards ratio 0.758, P = 0.00007) compared with the placebo group. The overall response rate in the aflibercept group was 19.8% compared with 11.1% in the placebo group (P = 0.0001). Grade 3 or 4 adverse events associated with aflibercept included diarrhea, fatigue, stomatitis, infections, hypertension, abdominal pain, neutropenia, and proteinuria (Fig. 2). Adverse events led to treatment discontinuation in 26.6% of patients in the aflibercept group, compared with 12.1% in the placebo group. The authors concluded that aflibercept in combination with FOLFIRI improved overall survival and progression-free survival in patients with metastatic colorectal cancer previously treated with oxaliplatin. While improvement in the primary outcomes was significant, it is unknown whether the addition of aflibercept translated into improvement in other important clinical outcomes, such as quality of life, considering the high rate of treatment discontinuation. Some toxicities potentially contributing to the discontinuation rate include doubling of the rate of diarrhea (2.5 times), febrile neutropenia (2.0 times), stomatitis (2.7 times), and infections (2.0 times). In addition, there were several-fold increases in hypertension (13 times) and proteinuria (6.5 times) in patients receiving aflibercept (Fig. 2). Given its potential use in the palliative setting, significant side effects and potential harm to the patients’ quality of life are crucial factors to be considered, in addition to response rate and survivorship. More data in this regard are expected to be available for review upon final study publication.

Grade 3/4 adverse events with >5% difference in incidence between aflibercept and placebo arms in the VELOUR trial.
Common Toxicity of Aflibercept
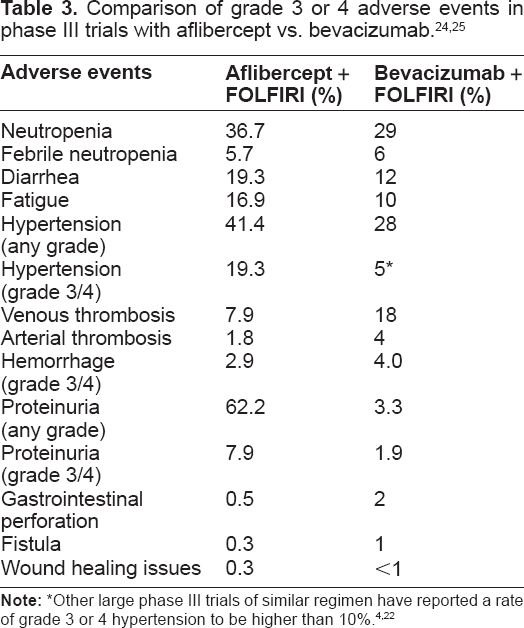
Aflibercept demonstrated toxicity similar to other agents targeting the VEGF pathway, such as bevacizumab. The most common adverse events in clinical trials included hypertension, proteinuria, fatigue, and diarrhea (Fig. 2). Table 3 compares the main side effects observed in the Phase III VELOUR trial (aflibercept combined with FOLFIRI) with those in the Phase IV AVIRI study (bevacizumab in combination with FOLFIRI).22,23 This comparison could be informative, although a cross-trial comparison carried inherent problems and needed to be interpreted with great caution. For example, the patient population differed between the two trials; VELOUR investigated the regimen as a second-line treatment, while in the AVIRI study, bevacizumab plus FOLFIRI were used in the first-line setting. As shown in Table 3, the most noticeable difference was that aflibercept trials revealed a numerically higher risk of hypertension and proteinuria of any grade and grade 3/4. Proteinuria of any grade was reported in 62% of patients receiving aflibercept, while approximately 8% had proteinuria of more than grade three. In the AVIRI study, bevacizumab was associated with an incidence of proteinuria of any grade and proteinuria ≥grade 3 of 3.3% and 1.9%, respectively. Any grade of hypertension was reported in 41% of patients on the aflibercept arm, compared with close to 20% with ≥grade 3. In patients receiving bevacizumab, 28% developed hypertension of any degree, while 5%–10% developed more severe hypertension (≥grade 3). In Phase III trials of other small molecule tyrosine kinase inhibitors, such as sunitinib and sorafenib, which shared many of the toxicities of VEGF antagonists, the rates of hypertension were found to be closer to that of bevacizumab. Any grade and grade 3/4 of hypertension were found in 24% and 8% of patients taking sunitinib, whereas these were observed in 17% and 4% of patients on sorafenib, respectively.26,27 The reason for this increased toxicity in the aflibercept group was unclear, but the enhanced affinity of aflibercept for VEGF-A and stronger inhibition of the VEGF pathway might play a role. Additionally, it is worth noting that in the VELOUR trial, the rate of proteinuria found in the placebo arm was higher than expected, ie, 40.7% with any grade and 1% with grade 3/4. Gastrointestinal perforations, fistula, and wound healing complications were rare events and occurred in less than 1% of the patients.
Adverse events, such as hypertension, were generally manageable with medications. Currently, there are no standard guidelines on management for VEGF inhibitor-associated hypertension. In the initial pivotal trial investigating the combination of bevacizumab and chemotherapy in the treatment of metastatic colorectal cancer, all hypertensive episodes were manageable with standard antihypertensives such as angiotensin-converting enzyme inhibitors, calcium channel blockers, and diuretics. 4 In recent years, advantages of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers in this population have been identified, including a low interaction potential with antiangiogenesis agents, the benefit of addressing treatment-induced proteinuria concurrently, and prevention of the expression of plasminogen activator inhibitor-1.44,45 Plasminogen activator inhibitor-1 was often found to be stimulated by antiangiogenesis agents, resulting in resistance of fibrinolysis and a higher risk of thrombosis.44,45 Furthermore, in multiple cancer cell lines and animal models, angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers were found to delay tumor cell growth, which was thought to be due to the effects of angiotensin II inhibition. 45 Therefore, some researchers advocated angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers to be among the first-line therapies for hypertension associated with angiogenesis blockers.44,45
Current Place of Aflibercept in Treatment of Metastatic Colorectal Cancer
Given the preliminary positive results of the Phase III VELOUR trial, Sanofi-Aventis and Regeneron Pharmaceuticals Inc, are preparing to submit regulatory applications for marketing approval to the US FDA and European Medicines Agency later this year. If successful, aflibercept will become the second VEGF pathway targeted agent approved for the treatment of metastatic colorectal cancer. It is anticipated that this agent would be administered along with FOLFIRI chemotherapy in patients whose tumors have progressed despite first-line therapy.
Future Directions
Multiple Phase I, II, and III trials are ongoing to investigate the effects of aflibercept alone or in combination with chemotherapy to treat a variety of malignancies. The AFFIRM trial is an ongoing Phase II study investigating the combination of aflibercept with FOLFOX as the first-line treatment for metastatic colorectal cancer. 46 The trial has completed accrual and its preliminary results are expected in late 2011. Given that bevacizumab showed a 5-month improvement in overall survival when combined with irinotecan, bolus fluorouracil, and leucovorin in an untreated population, it is of great interest how aflibercept would perform in this similar clinical setting. 4 When more new agents targeting the VEGF pathway become available, it would be prudent to compare the efficacy of these new agents with existing therapies, such as bevacizumab. The preliminary results of the VELOUR trial are comparable with those of E3200, the Phase III trial comparing FOLFOX with or without bevacizumab as second-line therapy in patients who have progressed on irinotecan-based therapy. 47 The optimal sequence of these biological agents, possibility of cross-resistance, and utility of the continuation of VEGF inhibition after progression are also important clinical questions that need to be answered.
Another area to be explored is the combination of VEGF and EGFR (endothelial growth factor receptor) blockade. Preclinical data and Phase II BOND-2 trial provided encouraging results on the combination of bevacizumab and cetuximab (an endothelial growth factor receptor inhibitor) with irinotecan in patients with metastatic colorectal cancer refractory to irinotecan. 48 However, large Phase III trials disappointingly showed increased toxicity with shortened progression-free survival when panitumumab or cetuximab was added to bevacizumab with chemotherapy.49,50 The reasons of these failed Phase III trials are unclear, and it is also unknown that if aflibercept can perform better in a similar situation.
The efficacy of anti-VEGF in the adjuvant setting is of interest to researchers due to the good performance of bevacizumab in metastatic colorectal cancer. However, bevacizumab failed to show benefits when combined with cytotoxic chemotherapy as adjuvant therapy in two large, randomized, Phase III trials.51,52 Considering that aflibercept is a much stronger VEGF inhibitor than bevacizumab, one may speculate on its possible efficacy in the adjuvant setting to treat these microscopic metastases.
Other active Phase III studies on aflibercept include the VENICE trial, evaluating aflibercept versus placebo combined with docetaxel and prednisone in treating patients with metastatic androgen independent prostate cancer, and the VITAL trial, evaluating aflibercept versus placebo in combination with docetaxel as a second-line treatment for patients with metastatic nonsmall cell lung cancer.53,54 Table 4 is a summary of the ongoing Phase III trials incorporating aflibercept. Although the preliminary results from the VITAL trial indicated that the addition of aflibercept to docetaxel failed to improve overall survival, its progression-free survival and overall response rate were superior to placebo. Final results remain to be seen after their data are published. 54
Summary of phase III trials of aflibercept.
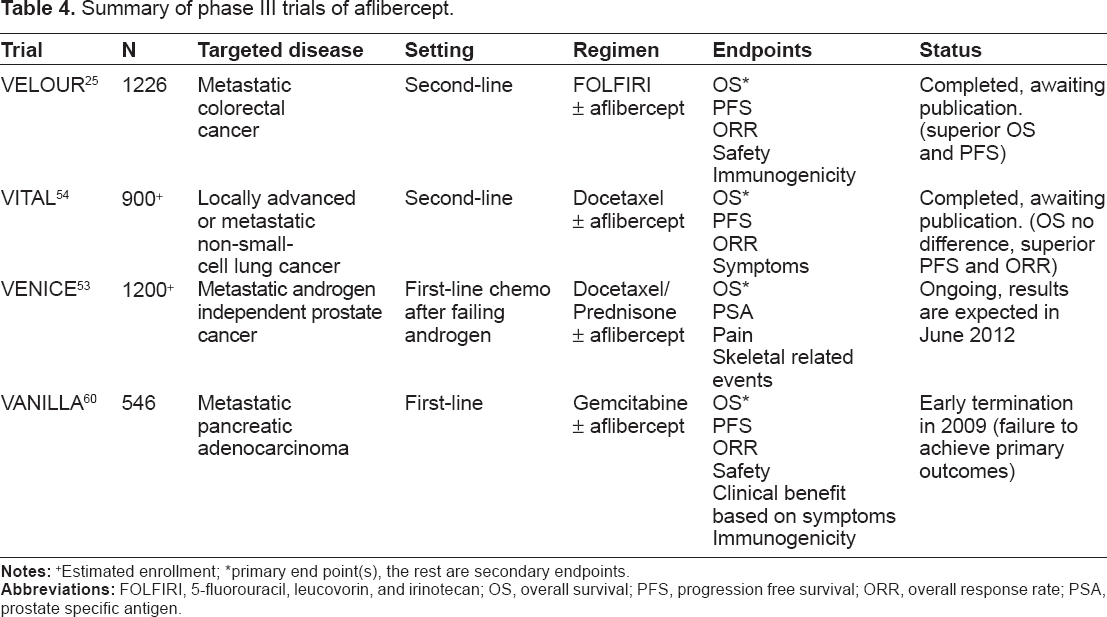
primary end point(s), the rest are secondary endpoints.
Given the significantly increased toxicity associated with aflibercept and other VEGF inhibitors, it is important to identify patients who would benefit most from VEGF inhibitors and avoid treatment-related toxicities in patients who will not benefit. Circulating biomarkers, such as VEGF and VEGFR2, have been investigated, but have not consistently demonstrated prognostic value. 55 There is ongoing research to identify more reliable factors to assist in these important clinical decisions.
Conclusion
Aflibercept is a new agent targeting the VEGF pathway in the treatment of solid tumors. The VELOUR trial showed the efficacy of aflibercept in improving progression-free survival and overall survival when combined with FOLFIRI as a second-line treatment for metastatic colorectal cancer. Aflibercept is also associated with increased toxicities, such as proteinuria and hypertension. Ongoing Phase II and Phase III trials will determine further the role of aflibercept in the treatment of colorectal cancer and other solid tumors.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.