
Abstract
The majority of patients with gastrointestinal cancers are over the age of 65. This age group comprises the minority of the patients enrolled in clinical trials, and it is unknown whether older patients achieve similar results as younger patients in terms of survival benefit and tolerability. In addition, there are few studies specifically designed for patients over 65 years. Subset analyses of individual trials and studies using pooled patient data from multiple trials provide some understanding on outcomes in older patients with gastrointestinal cancers. This article reviews the evidence on chemotherapeutic regimens in the elderly with colorectal, pancreatic, and gastroesophageal cancers, and discusses a practical approach to provide the best outcomes for older patients.
Keywords
Introduction
As our population ages, the treatment of older patients with cancer will become a more common part of oncology practice. Unfortunately, the geriatric population has typically been underrepresented in clinical trials, representing only 25%–30% of study participants.1,2 As a result, it is unclear if many of the advances in cancer treatment also apply to the elderly.
Data on studies in colorectal cancer indicate physicians are often reluctant to give elderly patients chemotherapy or to enroll them in clinical trials.3,4 Even after adjusting for comorbidities, performance status, and other treatment predictors, elderly patients are less likely to receive chemotherapy. 4 If they do receive palliative or adjuvant chemotherapy, it is often at reduced doses and/or with fewer cycles of treatment. This may affect outcomes, as data from the Surveillance, Epidemiology, and End Results (SEER) database suggest elderly patients who receive longer durations of 5-FU based chemotherapy have reduced mortality. 5 There is also evidence that among patients with comorbidities, those who receive cancer treatment survive longer. 6
Many investigators have attempted to address the gap that exists between the treatment of younger and older patients with cancer. This review focuses on the available data regarding systemic therapy for elderly patients with gastrointestinal malignancies, including colorectal, pancreatic, and gastroesophageal cancers.
Colorectal Cancer
Colorectal cancer (CRC) is the third most common cancer for both men and women, with 150,000 new diagnoses each year and 50,000 deaths per year. 7 The incidence of colorectal cancer increases with each decade of life. The median age at diagnosis is 71 years, and patients ≥65 years of age comprise 67% all colorectal cancer diagnoses.8,9 While the data are fairly consistent for older patients with metastatic CRC (mCRC), whether elderly patients benefit from recent advances in the adjuvant setting remains an area of controversy.
Adjuvant Therapy
The prior standard of care for adjuvant therapy for colorectal cancer was 5-fluorouracil combined with leucovorin (5-FU/LV). The benefit of adjuvant 5-FU therapy in elderly patients is clear. Three retrospective analyses documented improved survival with the use of adjuvant 5-FU therapy compared with surgery alone.10–12
It is not as evident if elderly patients benefit from the new standards in adjuvant therapy. Clinical trials have demonstrated that the addition of the chemotherapeutic agent oxaliplatin significantly improved outcomes for patients with stage III colon cancer over 5-FU/LV alone. Oxaliplatin plus 5-FU/LV (or capecitabine) in the adjuvant setting improves 3-year disease-free survival (DFS)13–15 and overall survival (OS). 13 Thus, the combination of oxaliplatin and 5-FU/LV (or capecitabine) has become the standard of care in the adjuvant setting for stage III disease.
Due to the lack of randomized trials aimed specifically at the elderly, much of the data on the use of oxaliplatin in the elderly comes from subset analyses of large randomized trials or pooled analyses involving multiple trials. One of the most detailed retrospective analyses evaluating oxaliplatin use in the elderly was a pooled analysis of 1,567 patients ≥70 years from clinical trials undergoing treatment with 5-FU/LV/oxaliplatin (FOLFOX) in either the adjuvant or advanced setting. 16 Toxicities were fairly similar between older and younger patients, with the exception of neutropenia and thrombocytopenia being significantly higher in patients ≥70 years. Additionally, the mortality at 60 days from starting therapy was not significantly different between young and older patients (1.1% vs. 2.3%, P = 0.2). Neither DFS nor OS differed significantly between patients <70 years and those ≥70 years. On multivariate analysis, age was not associated with likelihood of response among patients in the advanced disease trials. Dose intensity did not differ between older and younger patients, although older patients did receive fewer cycles of therapy.
The results from this pooled analysis suggest that oxaliplatin-based therapy can be administered with only mildly increased toxicity. The data also confirm that elderly patients can benefit from these therapies similarly to younger patients in terms of DFS and OS. However, the majority of the patients in this study were treated in the advanced setting. In addition, all European trials, which made up a significant percentage of the patients in the pooled analysis, did not include patients over the age of 75.
Studies of patients receiving therapy purely in the adjuvant setting have led to conflicting data regarding the benefit of oxaliplatin in elderly. Subset analyses of the Multicenter International Study of Oxaliplatin/5-Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer (MOSAIC) and the National Surgical Adjuvant Breast and Bowel Project (NASBP) C-07 trials demonstrated that the benefit of adjuvant oxaliplatin-based therapy for elderly patients is not statistically significant.13,15 In contrast, the N016968 trial, which compared bolus 5-FU/LV to a combination of capecitabine and oxaliplatin (XELOX) showed that elderly patients received a benefit in a short term endpoint of 3-year DFS, long term data from the NO 16968 trial remain pending. 14
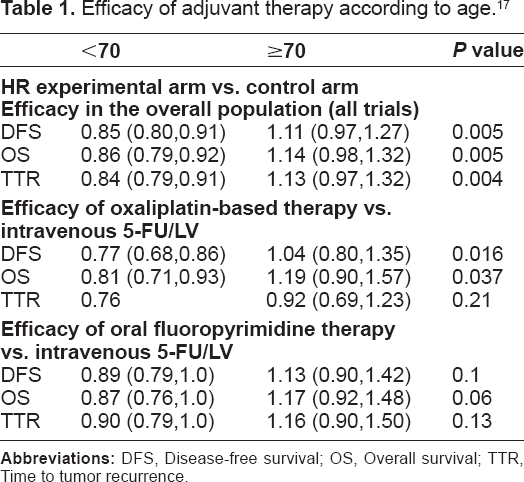
A pooled analysis of 12,669 patients from 6 randomized trials evaluated the impact of age on the efficacy of recently tested regimens (oxaliplatin-based, irinotecan-based, and oral fluoropyrimidine-based). 17 Seventeen percent of the patients (n = 2170) were ≥70 years of age. Newer adjuvant therapies were not associated with a significant treatment benefit in patients ≥70 compared to those <70 years (Table 1). This was consistent when specifically evaluating trials involving oxaliplatin and trials containing oral fluoropyrimidines. There was no increase in deaths in the first 6 months of adjuvant therapy between experimental and control arms overall or among different types of therapy. The results of this analysis raise concern about the use of oxaliplatin-based regimens in unselected elderly patients.
Efficacy of adjuvant therapy according to age. 17
A SEER-Medicare based study also evaluated the use of several regimens in 8,294 patients >65 years receiving adjuvant therapy for stage III colon cancer. 18 The analysis included patients treated with 5-FU/LV alone (n = 7,726), oxaliplatin-based therapy (n = 816), and irinotecan-based therapy (n = 382). After adjusting for multiple factors, oxaliplatin-based therapy was associated with improved overall survival (HR: 0.566; 95% CI: 0.370–0.866; P = 0.0087) and colorectal cancer-specific survival (HR: 0.385; 95% CI: 0.208–0.712; P = 0.0023) when compared to 5-FU/LV alone. Neither OS, nor colorectal cancer specific survival differed between irinotecan regimens and 5-FU/LV alone. It must be recognized that population-based studies are subject to potential selection bias as in general healthier patients are more likely to receive the more aggressive treatment.
The decision whether to treat elderly patients with oxaliplatin-based adjuvant therapy will become a growing problem over the next two decades, when the amount of people in the population over age 65 is expected to increase dramatically. This will result in greater numbers of patients requiring adjuvant therapy for resected colorectal cancer, and thus the role of oxaliplatin-based therapy in this situation needs to be further defined. Conflicting results of the above studies gives us the opportunity to individualize therapy for patients. A fit patient over 65 with low comorbidity may be a candidate of oxaliplatin-based adjuvant therapy. However, elderly patients with a poorer performance status and/or comorbidities may be more appropriate for 5-FU/LV or capecitabine alone.
Therapy for advanced/metastatic disease
In contrast to the adjuvant setting, multiple studies consistently show oxaliplatin-based therapy improves outcomes for the elderly with mCRC.19–22 Data from these and other trials also demonstrate that toxicities and tolerability were similar between older and younger patients.16,23 The reasons why the benefit of oxaliplatin therapy for elderly patients with advanced disease is not as evident in the adjuvant setting are unknown.
Strategies can be applied to reduce or minimize toxicity from the commonly used FOLFOX regimen. For instance, the “modified” FOLFOX regimens often omit the 5-FU bolus to minimize side effects, especially the degree of neutropenia and mucositis. Another option is to use the “stop-and-go” strategy as in the OPTFMOX trials. 24 With disease stability, 6–8 cycles of FOLFOX (with or without bevacizumab) can be followed by maintenance 5-FU or capecitabine (and bevacizumab). Upon progression oxaliplatin can be reintroduced or an alternative, irinotecan-based regimen can be used. This strategy does not compromise efficacy, and reduces the incidence of grade 3/4 neurotoxicity, and potentially maximizes benefit from oxaliplatin therapy.
Capecitabine plus oxaliplatin (XELOX) was found to be non-inferior to 5-FU plus oxaliplatin in a large randomized phase III trial in terms of progression-free and overall survival. 25 To determine whether this regimen was appropriate for elderly patients, an analysis of a phase II trial examined outcomes of when XELOX was used in patients ≥65 with mCRC. 22 Of 96 patients on the trial, 44 were ≥65 years. Older patients received a median of 8 cycles of XELOX. Response rates (RR) (58% and 52%), time to tumor progression (TTP) and OS were similar between younger and older patients (P > 0.5), and there were no significant differences in toxicity. A separate phase II trial evaluating XELOX in the elderly with mCRC also concluded it was a safe and effective regimen to use in selected elderly patients. 26
Irinotecan-based therapy has also become a standard for mCRC, typically when combined with 5-FU/LV (FOLFIRI). Two phase III trials have investigated the combination of FOLFIRI compared to 5-FU/LV, and both demonstrated improved RR and PFS for the triple combination regimen.27,28 The trial by Douillard et al 27 reported an improved OS 17.4 months for the irinotecan containing regimen versus 14.1 months for the 5-FU/LV arm (P = 0.031). Könne et al 28 did not report a significant increase in OS for the triple combination regimen when compared to the 5-FU/LV arm, but this was felt due to the increased availability of second and third line therapies. Patients over the age of 70 appear to achieve similar benefits as well as similar toxicity rates as younger individuals receiving irinotecan-based therapy. 29
Triple drug regimens have been examined in advanced CRC. Falcone et al 30 reported a significant improvement in OS (22.6 months vs. 16.7 months; HR 0.70, P = 0.032) with FOLFOXIRI when compared to FOLFIRI alone. This trial purposely selected patients to exclude elderly and frail individuals. A separate study comparing these 2 regimens included older patients (median age 66; 56% > 65 years) and poorer PS (36% ECOG PS of 0). 31 Compared the Falcone study, the doses were lower, there was no difference in OS, and elderly patients had significantly more toxicity.
More recently, monoclonal antibodies directed against the epidermal growth factor receptor (EGFR), cetuximab and panitumumab, have been developed. When used as a single agent in the last line setting or in combination with cytotoxic chemotherapy, the EGFR inhibitors provide benefit in the metastatic setting, but not the adjuvant setting.32–34 In an analysis of 56 patients age ≥70 years, the efficacy and tolerability appeared similar between younger and older patients. 35 These agents provide no survival advantage to patients with KRAS mutant tumors, and in fact, have the potential to add harm to this subset of patients.36,37 Therefore, all colorectal tumors should be tested for KRAS mutation status prior to administering EFGR inhibitors.
Bevacizumab is another targeted therapy showing benefit in advanced colorectal cancer.38–40 However, the use of bevacizumab in elderly patients should be carefully considered. A 1.8 fold increased risk of arterial thrombotic events (ATE) was seen with the use of bevacizumab in patients >65 years, an effect magnified with a prior history of ATEs. 41 Data from the Bevacizumab Regimens: Investigation of Treatment Effects and Safety (BRiTE) registry confirmed this risk in patients >75 years. 42 On the other hand, elderly patients did not have an increased risk of gastrointestinal bleeding/perforation or hypertension compared with a younger cohort. Elderly patients must be counseled on the increased risk of ATEs, and for those with prior ATE, bevacizumab is contraindicated.
Newer advances in the treatment of mCRC should not be withheld from older patients based on age alone. Multiple studies indicate selected patients ≥65 years can achieve similar benefits to oxaliplatin- and irinotecan-based therapy as well as targeted therapy without substantial addition in toxicity. One must use caution in those with poorer PS or multiple comorbidities, as these patients are a different population than those typically enrolled on clinical trials. Fluoropyrimidine therapy alone may be more appropriate for such individuals.
Pancreatic Cancer
Pancreatic cancer is a disease of older patients. The median age at diagnosis in the United States is 72 years, and over 68% of those diagnosed are ≥65 years of age. 43 This section will discuss systemic therapy for older patients in the adjuvant, locally advanced, and metastatic settings.
Adjuvant Therapy
Two agents are currently used for adjuvant therapy after resection of pancreatic cancer: 5-FU or gemcitabine. The ESPAC-1 trial demonstrated a small, but significant survival benefit for 5-FU therapy versus those who did not receive chemotherapy, with median survivals of 19.7 months and 14.0 months respectively (HR 0.66 [95% CI 0.52–0.83], P = 0.0005). 44 The subsequent CONKO-1 trial demonstrated a significant increase in PFS and OS for patients receiving gemcitabine versus observation alone. 45 After extended follow-up, the median OS was 22.8 months in the gemcitabine arm and 20.2 months in the observation arm (P = 0.005), with estimated survival at 5 years of 21.0% and 9.0% respectively.
In the ESPAC-3 trial patients with resected pancreatic cancer were randomized to receive bolus 5-FU/LV (Mayo Clinic regimen) versus gemcitabine. 46 The median age of patients on this trial was 63 years (range 31–85 years). Median survival was similar between the 5-FU/LV arm and the gemcitabine arm, 23.0 months and 23.6 months respectively (P = 0.39). Quality of life (QOL) did not differ between the 2 treatment arms, but there were significantly higher rates of adverse events in the 5FU group. 14% of patients had serious AEs in the 5-FU group, with higher rates of grade 3/4 stomatitis, but hematologic toxicities were more common in the gemcitabine arm. Age was not a prognostic factor for survival. Given the lower rates of adverse events with gemcitabine, it would appear to be a more reasonable option for elderly patients.
Studies investigating the use of concurrent chemoradiation therapy in the adjuvant setting have yielded conflicting results regarding the survival benefit with the addition of radiation therapy.47–50 Concurrent chemoradiation therapy is often utilized in the adjuvant setting when there is evidence of nodal involvement detected at the time of surgery. The aforementioned studies did not include subset analyses for tolerability or survival outcomes in elderly patients. However, we might be able to extrapolate from data on the use of concurrent chemoradiation therapy in elderly patients with locally advanced, unresectable pancreatic cancer (see below).
Locally advanced disease
Concurrent chemoradiation therapy became a standard for locally advanced, unresectable pancreatic cancer after it was shown to improve 1-year survival by 30% over radiation therapy alone. 51 A small retrospective analysis evaluated outcomes of patients undergoing chemoradiation therapy with protracted 5-FU infusion (200 mg/m2/day) along with radiation therapy (50.4 Gy in 28 fractions over 5.5 weeks) according to age: <70 years (n = 39) or ≥70 years (n = 19). 52 There were no significant differences in severe toxicity, response rates or incidence in treatment discontinuation. Median OS was slightly higher among the older patients (11.3 months) versus younger patients (9.5 months), likely a reflection of higher baseline performance status in the older group. This small study provides evidence that selected elderly patients can tolerate concurrent 5-FU-based chemoradiation therapy as well as younger patients.
Miyamoto et al 53 reported a series of 42 patients >75 years of age who received chemoradiation therapy either as adjuvant or definitive therapy for pancreatic cancer. The study included 3 patients who received both 5-FU and gemcitabine and 2 patients who received capecitabine as radiosensitizer; the remaining 37 patients received 5-FU. The median OS was 8.6 months in the inoperable patients and 20.6 months for those in the adjuvant therapy group, similar to historic controls. Nausea, pain, and failure to thrive were the most common toxicities during treatment. Hospitalization occurred in 8 patients (19%), 7 patients (18%) had an emergency room visit, and 9 patients (21%) did not complete therapy.
Metastatic Disease
The pivotal trial reported by Bums et al 54 established the role of gemcitabine for patients with advanced pancreatic cancer. Patients were randomized to receive gemcitabine versus 5-FU (administered at 500 mg/m2 over 30 minutes without LV). There was a significant OS benefit in the gemcitabine arm with a median survival of 5.6 months compared to 4.4 months in the 5-FU arm (P = 0.0025), and the 1-year survival rate was 18% versus 2%, respectively. While the difference in median survival was not dramatic, patients in the gemcitabine arm had a significant improvement in clinical benefits, pre-defined as an improvement in performance status, opioid requirements and weight loss (23.8% vs. 4.8%).
We can gain insight on toxicities specifically in the elderly with gemcitabine from a small retrospective study of 39 patients ≥70 years who received gemcitabine 1000 mg/m2 weeks 1–3 of a 4 week cycle for advanced pancreatic cancer. 55 Fifty-nine percent of patients received 100% of planned dose-intensity Grade 3–4 adverse events were most commonly neutropenia (38%), thrombocytopenia (28%), and anemia (18%). The median PFS was 7 months and OS was 10 months. The authors concluded that selected elderly patients could receive similar benefits to younger patients.
Multiple agents have been combined with gemcitabine in attempts to improve outcomes for patients with metastatic pancreatic cancer. The only agent that has demonstrated a survival benefit is erlotinib. In a phase III trial, patients were randomized to gemcitabine plus erlotinib versus gemcitabine alone. 56 The OS was 6.24 months in the combination arm versus 5.91 months alone (HR 0.82; 95% CI 0.69–0.99; P = 0.038). Efficacy and toxicity was not evaluated by age. However, due to the minimal survival benefit, it is generally felt the increase in toxicity and cost does not warrant the routine use of erlotinib, particularly in the elderly population.
Oxaliplatin has also shown activity in metastatic pancreatic cancer in the second-line setting. 57 Extrapolating from experience among elderly patients with colorectal cancer, one would expect that oxaliplatin could safely be administered to patients ≥65 years. However, the performance status of patients with metastatic pancreatic cancer typically declines much quicker than mCRC, so extra caution must be used in this setting. The triple drug combination regimen using 5-FU, irinotecan and oxaliplatin (FOLFIRINOX), albeit highly active, is likely too toxic to be recommended for standard use in elderly patients with pancreatic cancer. 58
Gastroesophageal Cancers
Patients ≥65 years of age make up 60.9% and 63.6% of esophageal and gastric cancers respectively. For the general population, there is clear evidence that chemotherapy, whether alone or in combination with radiation therapy, improves survival in patients with gastroesophageal cancers over surgery alone.59–63 Preoperative, perioperative, and postoperative regimens with or without radiation therapy have been studied. The following discussion addresses each approach as it relates to treating the elderly.
Perioperative therapy for gastric cancer
The Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial randomized patients with operable gastric cancer to receive three cycles of ECF (epirubicin, cisplatin, 5-FU) before and after surgery, versus surgery alone. 61 Patients in the chemotherapy arm had a 5-year survival of 36.3% versus 23% in the surgery alone arm, with a HR for death of 0.74 (95% CI 0.59–0.93; P = 0.009). The median age of patients on the trial was 62 years (range 23–85 years), and 20% of patients were >70 years. The survival results were independent of age, with patients >70 years benefitting as much as those <70 years. Toxicity was not evaluated based on age. Postoperative complications did not differ between the two groups, but only half of the patients received chemotherapy after resection mainly due to progression/early death, complications, or patient refusal.
Adjuvant therapy for gastric cancer
Despite many clinical trials, there is no clear adjuvant therapy standard for gastric cancer, although meta-analyses have concluded adjuvant therapy does provide benefit.64–66 A recent large meta-analysis from the Global Advanced/Adjuvant Stomach Tumor Research International Collaboration (GASTRIC) Group included 17 randomized trials and 3838 patients. 67 The GASTRIC investigators found that adjuvant therapy for gastric cancer was associated with improved survival (HR 0.82, 95% CI 0.75–0.9, P < 0.001). There appears to be the greatest benefit from 5-FU based therapy, even as monotherapy. Although there was not a specific analysis related to age, it is likely that older patients fit enough for a clinical trial do stand to benefit from adjuvant therapy, even if they are not candidates for combination therapy regimens.
The Intergroup trial 0116 randomized patients to receive adjuvant 5-FU for one cycle followed by chemoradiation followed by 2 more cycles of 5-FU versus surgery alone. 62 Median survival was superior in the experimental arm compared to surgery alone, 36 months and 27 months respectively, P = 0.005. The median age on the trial was 60 years in the treatment arm (range 25–87) and 59 years in the control arm (range 23–30). The effects of treatment were independent of age, however there was no toxicity analysis in relation to age. Hematologic toxicities occurred in 54% of patients and gastrointestinal toxicity in 33% of patients. This trial was criticized because more than half the patients received less than a D1 resection, and it remains uncertain if chemotherapy would have improved survival had adequate resection been performed on every patient. This regimen is not commonly utilized outside of the US.
A large, randomized phase III trial from Japan demonstrated a survival benefit for S-1, another oral fluoropyrimidine, over surgery alone. 63 Three-year OS was 80.1% in the S-1 arm compared to 70.1% in the surgery alone arm (HR 0.68, 95% CI 0.52 to 0.87; P = 0.003). The most common adverse events with S-1 were anorexia (6.0%), nausea (3.7%), and diarrhea (3.1%). Due to differences in tolerability in non-Asian patients, S-1 has not been utilized in Western countries.
Preoperative therapy for esophageal cancer
In general, the trend has been to utilize preoperative therapy in locally advanced adenocarcinomas of the esophagus and gastroesophageal junction, based on results of several phase III trials.68,69 The advantage to this approach is therapy prior to surgical resection is more feasible than after resection. In addition, preoperative therapy can downstage the tumor as well as potentially address any micrometastatic disease.
Data would suggest that elderly individuals have the potential to benefit from this approach as much as younger individuals, with slightly more toxicity. Rice et al 70 reported a retrospective study evaluating patients with esophageal cancer ≥70 years who did (n = 35) or did not (n = 39) receive preoperative chemoradiotherapy compared to patients <70 years. The chemotherapy used was most commonly cisplatin/5-FU or ataxane. The efficacy of therapy did not differ between younger or older patients, with no difference in 1- or 3-year survival. Older age (>70) was not a predictor in postoperative mortality. Older patients had greater incidence of perioperative blood transfusions and postoperative atrial arrhythmias.
For those patients who are not candidates for cisplatin/5-FU, carboplatin and paclitaxel are alternative radiosensitizing agents with OS benefit over surgery alone and an acceptable toxicity profile, in particular for patients with squamous cell carcinomas. 71
Treatment for advanced/metastatic gastroesophageal cancer
A meta-analysis of randomized phase II and III trials in advanced gastric cancer clearly demonstrated chemotherapy improves survival in advanced gastroesophageal cancer. 72 Multiple agents including platinums, fluoropyrimidines, anthracyclines, taxanes, and irinotecan show activity. The trend over the years has gone from single agent to doublet to triplet chemotherapy regimens. As more agents are used concomitantly, survival has improved at the price of increased toxicity.
Three-drug regimens became a new standard based on the phase III trial V325 that demonstrated a survival benefit over for docetaxel and cisplatin plus fluorouracil (DCF) over cisplatin plus 5-FU (CF) alone. 73 Patients in the DCF arm had a median OS of 9.2 months, compared to 8.6 months in the CF arm (P = 0.02). The 2-year survival rate of 18% in the experimental arm established DCF as a new standard. The small improvement in OS came with significantly higher rates of grade III/IV neutropenia (82% vs. 57%), diarrhea (19% vs. 8%), and lethargy (19% vs. 14%). In addition, 50% of patients were taken off therapy due to adverse events or patient refusal. Elderly patients were very underrepresented in this trial, with the median age of participants 55 years. Given the high rates of hematologic toxicities and small survival benefit, it remains unclear if this regimen will be tolerable in the elderly patient. Modified DCF regimens, such as reported by Shah et al 74 are associated with reduced rates of neutropenia without compromising efficacy and may be more appropriate for older adults.
The goal of the Randomized ECF for adjuvant and locally advanced esophagogastric cancer (REAL-2) study was to establish the non-inferiority of capecitabine (X) to 5-FU (F) and oxaliplatin (O) to cisplatin (C) when combined with epirubicin (E). 75 Patients were randomized in a 2 by 2 design to receive ECF, ECX, EOF and EOX. The median survival in the four study arms was 9.9 months, 9.9 months, 9.3 months and 11.2 months respectively. This trial established the non-inferiority of capecitabine (to 5-FU) and oxaliplatin (to cisplatin), a result that has enhanced the options available. Importantly, the oxaliplatin-containing arms had less neutropenia, alopecia, renal toxicity, and thromboembolism, but greater neuropathy and diarrhea. In contrast to the V325 trial, REAL-2 included older patients; the median age varied between 61 and 65 among the treatment arms.
There have not been prospective trials specifically evaluating outcomes in the elderly with esophagogastric cancers. However there are two pooled analyses of data from clinical trials examining outcomes in the elderly. The first includes 257 patients ≥70 years from 3 clinical trials. The incidence of grade III/IV toxicities, response rates, and overall survival did not differ significantly between patients ≥70 years compared to those <70 years. Another analysis of 367 patients with incurable esophagogastric cancers within 8 consecutive first line therapy trials through North Central Cancer Treatment Group (NCCTG) from 1987 to 2006 included 154 patients ≥65 years of age. 76 Despite having poorer performance status, there was also no difference in median survival or PFS between older and younger patients respectively. In this analysis, there were higher rates of adverse events including grade 3+ leucopenia, stomatitis, fatigue and grade 4 vomiting. In addition, there were higher rates of grade 4+ events in the elderly (40% vs. 28%, P = 0.02).
S-1 has shown activity in patients with advanced gastric cancer both as a single agent and in combination with cisplatin or irinotecan among Japanese patients.63,77–79 However, when tested in the Western patients, S-1 combined with cisplatin did not show a survival advantage over 5-FU plus cisplatin. 80 Therefore, S-1 has not been approved for use in the US.
The Trastuzumab for Gastric Cancer (ToGA) trial demonstrated clear benefit of targeted therapy for gastric cancer and established trastuzumab as the new standard for HER2+ disease. 81 Twenty percent of patients on this trial had GE junction tumors. Trastuzumab, when added to 5-FU plus cisplatin, significantly improved median OS over 5-FU plus cisplatin alone 13.8 months versus 11.1 months respectively (HR 0.74; 95% CI 0.60–0.91; P = 0.0046). There was no difference in adverse events between the 2 arms, with nausea, vomiting, and neutropenia being the most common toxicities. Cardiac dysfunction (denned as a ≥10% drop in left ventricular systolic function to <50%) occurred in 11 of 237 patients (5%) in the trastuzumab arm compared to 2 of 187 patients (1%) with chemotherapy alone, but these changes were clinically asymptomatic. The average age of the patients on trial was approximately 59 years. Age was a prespecified sub-group of patients evaluated for OS, the HR for survival 0.66 (95% CI 0.49–0.88), indicating a significant benefit for patients ≥60 years of age. Trastuzumab can be used without adding significant toxicity, however careful monitoring for systolic dysfunction is recommended.
Although multiple clinical trials trying to define optimal management for gastroesophageal cancers have left us with unanswered questions, they have also provided evidence for a variety of agents and regimens that have activity in this disease. This gives oncologists the ability to tailor treatment to the particular needs of each elderly patient.
Conclusions
The data reviewed in this article provide evidence that elderly patients with gastrointestinal cancers can benefit from systemic therapy. The decision to select patients for particular regimens should not be based solely on age alone. Likewise, agents that prolong survival should not automatically be withheld from patients with imperfect performance status or comorbidity. Each individual should be assessed for an appropriate regimen. Most importantly, the decision of how to treat elderly patients must incorporate goals and preferences of the patient after a careful discussion of risks and benefits.
Several tools exist that may be utilized to guide treatment decisions for the older patient with cancer such as geriatric assessment scores, comorbidity indices, frailty indices, and prognostic indices for survival. These may help the clinician to better estimate the patient's physical and mental condition to determine if the potential survival benefits are worth the potential toxicity, however they may not be easy to incorporate in a busy clinical practice. Efforts are ongoing to assess shorter screening tools to identify those geriatric patients who may not tolerate standard therapy. 82
In order to improve upon our knowledge of how to treat older patients with cancer, these patients should be enrolled in clinical trials with more frequency. In addition, there is a need for clinical trials need to be designed for this patient population. An upcoming Intergroup study will evaluate oxaliplatin/fluoropyrimidine therapy plus bevacizumab versus fluoropyrimidine plus bevacizumab as first-line therapy in elderly patients with mCRC. This trial incorporates as a component the prospective validation of a frailty index. Future trials should also be designed to incorporate an assessment of outcomes in relation to age to provide further guidance on whether the regimen is appropriate for elderly patients.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.