
Abstract
Primary and secondary glioblastomas (GBMs) are two distinct diseases. The genetic and epigenetic background of these tumors is highly variable. The treatment procedure for these tumors is often unsuccessful because of the cellular heterogeneity and intrinsic ability of the tumor cells to invade healthy tissues. The fatal outcome of these tumors promotes researchers to find out new markers associated with the prognosis and treatment planning. In this communication, the role of glioblastoma stem cells in tumor progression and the malignant behavior of GBMs are summarized with attention to the signaling pathways and molecular regulators that are involved in maintaining the glioblastoma stem cell phenotype. A better understanding of these stem cell-like cells is necessary for designing new effective treatments and developing novel molecular strategies to target glioblastoma stem cells. We discuss hypoxia as a new therapeutic target for GBM. We focus on the inhibition of signaling pathways, which are associated with the hypoxia-mediated maintenance of glioblastoma stem cells, and the knockdown of hypoxia-inducible factors, which could be identified as attractive molecular target approaches for GBM therapeutics.
Introduction
Cancer stem cells, also known as tumor-initiating cells or tumor-propagating cells,1,2 have the ability to self-renew and differentiate into various cell types. 3 These cells also show stem cell properties that include asymmetric cell division, infinite growth, and multipotency. 4 Cancer stem cells have been identified in various tumor types, such as prostate tumors, pancreatic adenocarcinomas, colon carcinomas, hepatocellular carcinomas, melanoma, lung and breast cancers, osteosarcomas, and brain tumors. 5
In 2002 the stem cell properties of human cortical glial tumors were discovered and isolated precursor cells that are capable of forming neurosphere in vitro. 4 Glioblastomas (GBMs) are the most common and lethal brain tumors. The current standard therapies include tumor resection, adjuvant chemotherapy, and chemoradiotherapy.1,6 GBMs express multipotent neural stem cell (NSC)-like cells that also contain neurons, astrocytes, and oligodendrocytes within the tumor mass. 6 Cancer stem cells in malignant gliomas were called glioblastoma stem cells (GSCs). These cells have the potential to differentiate into astrocytes, oligodendrocytes, and neurons. The characteristics of glioblastoma cancer stem cells include self-renewal, 6 pluripotency, neurosphere formation, 5 proliferation, angiogenesis, invasion, modulation of immune response, 6 marker expression, multilineage differentiation, and high motility (Table 1).7,8
Biological characteristics of normal stem cells, cancer stem cells, and glioblastoma stem cells.

Niches are important for self-renewal and undifferentiated state of normal stem cells. In this regard, GSCs were located in a perivascular niche in brain tumors that recapitulates a relationship between normal neural stem/progenitors and the vasculature. 1 After DNA damage, normal stem cells could assume a quiescent state and stop proliferating. However, glioma stem cells express various proteins that promote the survival of cells following cancer treatment procedures, which include the major drug resistance proteins, such as MGMT (O-6-methylguanine-DNA methyltransferase), and antiapoptotic genes, such as FLIP (FLICE-like inhibitory protein), BCL-2 (B-Cell CLL/Lymphoma 2), BCL-XL (B-cell lymphoma-extra large), and cIAP1 (cellular inhibitor of apoptosis protein-1). 7
The major problems of these malignancies are their highly infiltrative nature and extreme resistance to conventional treatments. Active tumor angiogenesis is one of the hallmarks of GBMs. Cancer stem cells promote the development of their own perivascular niche through the secretion of proangiogenic factors, prominently vascular endothelial growth factor (VEGF). Florid angiogenesis is a defining hallmark of GBMs, although these tumors are also characterized by hypoxic regions of pseudopalisading necrosis. 1 Florid neovascularization also plays a crucial role in providing nutrition and oxygen and removing waste to facilitate the rapid growth and progression of GBMs. The degree of vascularization is significantly correlated with tumor aggressiveness and clinical prognosis. 6
Oxygen tension is tightly regulated in normal physiology and is an important signal in development, with low oxygen tension associated with the maintenance of undifferentiated cell state. Hypoxia promotes the self-renewal of embryonic stem cells (ESCs) and prevents the differentiation of NSCs in vitro. 1 Hypoxia can promote the expansion of GSC fraction and regulate the expression of stem cell markers. Hypoxia may enhance tumor progression and therapeutic resistance through its promotion of a cancer stem cell phenotype and induction of VEGF and other proangiogenic factors. 6 Hypoxic and necrotic regions are common in solid tumors, and their presence correlates with an aggressive clinical course. Previous studies have proposed that tumor necrosis was driven by hypoxia, which has been supported by the demonstration of striking upregulation of hypoxia-inducible factor (HIF) target genes in the region immediately adjacent to the necrotic areas. The activation of HIF pathways by tumor hypoxia itself is the major cause of deregulated tumor metabolism. 9 Cells preferentially utilize glucose carbon for palmitate synthesis under normoxic conditions; however, fatty acids produced under hypoxia are primarily synthesized from glutamine carbon via the reductive pathway, and knockdown of IDH1 protein was shown to mitigate the use of reductive glutamine metabolism for lipogenesis under hypoxia, as reported by Metallo et al. 10
Solid tumors consist of heterogeneous cancer cells, as well as vasculatures, stromal elements, and inflammatory cells. GBMs display intratumoral heterogeneity and cellular hierarchy not only morphologically but also in differentiation status. 6
Various studies have tried to generate a model of GBM, and it was hypothesized that the GBM tumor mass was multilayered and that every tumor layer showed distinct characteristics. Pistollato et al. 11 described the distribution of GSCs based on the tissue hypoxic gradient, Piccirillo et al. 12 found a different behavior of GSCs derived from distinct tumor areas, and Tafani et al. 13 demonstrated a different proinflammatory gene expression in diverse tumor areas. The hypoxic tumor cells showed high activation of nuclear factor kappa B (NF-κB) and high expression of proinflammatory genes. The peritumor area showed high activation of NF-κB and low expression of the proinflammatory genes; the core region of the tumor showed high proliferation capacity and clonogenic ability, and the low expression of the differentiation markers and the genetic abnormalities are not shared with the tumor periphery. The necrotic core of the tumor showed highly hypoxic conditions, with a high enrichment of GSCs and expression of immature markers such as CD133 and nestin; the in vitro studies showed that this necrotic core of the tumor is resistant to chemotherapy. The intermediate layer of the tumor was hypoxic and enriched with GSCs and showed the expression of mixed lineage markers. The in vitro studies showed that the intermediate layer of the tumor was resistant to chemotherapy. The periphery of the tumor was marked by high vascularization, rare occurrence of GSCs, expression of differentiation markers, sensitivity to chemotherapy, low-level proliferation index, and clonogenic ability. In contrast, NF-κB activation and expression of proinflammatory genes were not detected in the normal brain. 14
Molecular markers for GSCs
Molecular markers associated with the maintenance of GSCs are differentially expressed in GSCs. These markers are categorized, according to the cellular localization, as cell surface markers, such as CD133, CD15, A2B5, and L1CAM6,7; cytoskeletal proteins, such as nestin; transcriptional factors, such as Sox2, Nanog, and Oct3/4; posttranscriptional factors, such as Musashi 1; and poly-comb transcriptional suppressors, such as Bmi1 and Ezh2. 15
Cell surface proteins were generally used to isolate and characterize cancer stem cells. The identification of cancer stem cell–specific cell surface markers is very important for the diagnosis and treatment of malignancies. CD133 was the first discovered cell surface marker for hematopoietic stem cells and also one of the best-studied GSC markers to date. It is expressed in both early postnatal brain and adult brain tissues. 5 CD133 expression rapidly decreased during cell differentiation, and this characteristic could be used to identify and isolate stem cells. 5 A2B5 is a cell surface marker expressed on neural precursor cells either in the adult human brain or in the subventricular zone of human embryos. 7 Cell surface markers were used for the isolation and characterization of CD133, 16 CD15, 17 and ALDH1A3 (Aldefluor) of GSCs. 18 CD15 is also known as stage-specific embryonic antigen 1 (SSEA1) 19 and is expressed in embryonic or adult central nervous system stem cells20,21 and GBMs. 22 However, in contrast to CD133 and CD15, the other cellular factors such as Sox2 and Oct4 are not useful for the isolation of live GSCs from tumor tissues, given their intracellular localization, such as in the nucleus or the cytoplasm. The stem cell transcription factors, including Sox2, Oct4, Nanog, c-Myc, Olig2, and Bmi1, have a critical role in the self-renewal, proliferation, survival, and multi lineage differentiation of GSCs. Bmi1 is also important for the self-renewal ability of GSCs. 15 Oct4, Sox 2, and c-Myc contributed to the survival and self-renewal of brain tumor stem cells. 1 NSCs were associated with repair after stroke and severe injuries and were also suggested for the treatment of neurological disorders. 7 L1CAM (L1, CD171) is a neuronal cell adhesion molecule and is essential for the growth and migration of cells during the development of central nervous system and for the survival of CD133-positive glioma stem cells.23,24 Studies have shown that L1CAM regulates both neural cell growth and survival. By using lentiviral-mediated short hairpin RNA interference in CD133 for targeting L1CAM, it was shown that the growth and neurosphere formation of GSCs were inhibited. L1CAM-mediated signaling leads to radioresistance in GSCs. Therefore, L1CAM is a therapeutic target for GBM therapy. 24 Musashi is an RNA-binding protein25,26 and is important for grading of brain tumors and proliferative activity in gliomas and melanomas. 7 Musashi family is a highly conserved RNA-binding protein group expressed in undifferentiated stem/precursor cells at both embryonic and adult stages, and these proteins were shown to control the stem cell state through the translational regulation of target mRNAs.5,25
Therapeutic targets for GBM
The target of GBM is the bulk of the tumor. Tumor recurrence was attributed to glioma stem cell resistance. Against the bulk tumor, the most effective treatment procedures include radiation and chemotherapy. 7 Therefore, treatments that directly target glioma stem cells could yield long-term cures. It was hypothesized that once the glioma stem cells have been eliminated, the bulk tumor would not be able to sustain itself and would disseminate.
Wnt family, Sonic hedgehog, Notch, 2 transforming growth factor beta (TGF-β), bone morphogenetic protein (BMP) signaling, 27 Homeobox family, B lymphoma Mo-MLV insertion region 1 homolog (Bmi-1), PTEN (phosphatase and tensin homolog), telomerase, efflux transporters, epidermal growth factor (EGF), microRNA, and VEGF receptors are important for self-renewal and differentiation of GSCs, and they might be useful for targeted therapy in GSCs. 2 TGF-β signaling is important for the self-renewal and the maintenance of perivascular GSCs, and PI3K/Akt signaling promotes self-renewal of GSCs in vitro and is also important for the proliferation and survival of GSCs. MAPK signaling is important for the proliferation and survival of GSCs. 27 The activation of several signaling pathways, including receptor tyrosine kinase, Akt, MARK, Wnt, Notch, Hedgehog, and JAK/STAT pathways, is involved in the progression and proliferation of GSCs. 28 STAT-3 is a candidate therapeutic target for GSCs. STAT3 is activated by various cytokines and growth factors. In GSCs, STAT-3 plays a role as a molecular center in several important signaling pathways that control proliferation, cell cycle progression, antiapoptosis, invasion, angiogenesis, and immune evasion. Thus, STAT-3 has a great potential to be used as a therapeutic target. 3 The cross talk between the Notch and STAT3 pathways was reported by Garner et al. 29 , who showed that STAT-3 binds to the adjacent site in the Notch1 promoter and activation of Notch signaling directly activates transcription of stem cell markers in glioma, such as nestin. 7 The Notch signaling pathway is an important regulator of normal development, adult stem cell maintenance, and tumorigenesis in the brain. 7 Inhibiting the Notch signaling pathway, Notch receptors, ligands, and downstream pathways may inhibit the maintenance of glioma stem cell population, and inhibitors of the Notch pathway components represent promising therapeutic candidates for GBM.
Nestin is an intermediate filament protein that is produced in stem cells during the normal development. Nestin has several important cellular functions, including signaling, cytoskeleton organization, and metabolism of brain cells. Nestin is frequently expressed in GBMs and is important for the grading and clinical outcome of GBMs. 2 Nestin-positive (+) and CD133-positive (+) brain tumor cells were located in the proximity of the tumor vascular system, which indicates that glioma stem cells could be associated with a vascular stem cell niche. 7 Recent studies showed that CD133-positive GSCs were resistant to conventional anticancer therapies, 2 and CD133 positivity has been postulated to be a glioma stem cell marker. The failure to cure GBM has been attributed to the fact that therapies were aimed at the tumor bulk, without significantly harming tumor stem cell–like cells. CD133+ brain cells could become therapy targets to eliminate brain tumors.
The Hedgehog pathway has a vital role in normal brain development, NSC survival, and glioma tumorigenesis, 7 and cyclopamine treatment inhibits the Hedgehog pathway and decreases the glioma stem cells. The VEGF family and tyrosine kinase VEGF receptors are important in glioma angiogenesis, and targeting this vascular niche could be a treatment strategy. 7
The mTOR (rapamycin) plays a critical role in regulating mRNA translation and protein synthesis in response to various environmental signals 30 and is a target for radiosensitization in GBM. Kahn and colleagues exposed GSCs to AZD2014, 31 which is a dual mTORC1/mTORC2 inhibitor, 32 and showed the inhibition of mTORC 1 and 2 activities in GSCs. The combined use of AZD2014 and radiation delivered to mice bearing GSC-initiated orthotopic xenografts significantly prolonged survival when compared with the individual treatments. They concluded that AZD2014 enhanced the radiosensitivity of GSCs both in vitro and under orthotopic in vivo conditions and suggested that this effect involved an inhibition of DNA repair. 31
Heat shock protein 90 (HSP-90) is a molecular chaperone that plays an essential role in many cellular processes, including cell cycle control, cell survival, hormone and other signaling pathways. It is important for stress response and has a key role in maintaining cellular homeostasis. 33 HSP-90 inhibits the GSCs and synergizes with radiation/Temozolomide (TMZ). Increasing the radiosensitivity of GSCs has been suggested as another therapeutic approach for treatment planning of GBMs, which could be done by using antiepidermal growth factor receptors, such as cetuximab and nimotuzumab. 2 The previous studies showed that combination of BCNU (Carmustine) and chloride channel blocker promotes apoptosis and sensitizes gliomas to BCNU. 2
Cell-based cancer therapy was aimed at inhibiting the self-renewing capacity of tumors. The viral delivery of the replicaton-restricted viruses and retrovirus, adenovirus (Adv), and herpes simplex virus-1 (HSV-1) were the most studied viral brain tumor therapy vectors, 34 delivery of suicide genes to convert prodrugs in the tumor and achieve tumor cell death, delivery of cytokine genes to activate and attract immune cells against the tumor, delivery of tumor-suppressor genes to repro-gram tumor cells into apoptosis, or delivery of conditionally replicating viruses to specifically lyse tumor cells while sparing normal tissue. 35 Uzzaman et al showed that the ESC-derived astrocytes conditionally expressing genes can be used to induce apoptosis in malignant glioma cells in vitro. The tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) gene was shown to induce apoptosis in a variety of tumor cells, including gliomas. The authors conclude that TRAIL was a rare example because it kills cancer cells but not normal cells. 34 Brescia et al. 36 used lentivirus-mediated short hairpin RNA for silencing CD133 in human GBM neurospheres and showed that CD133 could be used as a therapeutic target for GBMs.
NSCs were first used as oncolytic virus carriers by Herrlinger and colleagues. They used NSCs to carry conditionally replicating HSV into preimplanted cerebral gliomas, and the possible advantages over the inoculation of viral particles were that the migratory NSCs might deliver the viruses at further distances within the tumor compared to virus alone, they can protect the viruses from host immunosurveillance, and their own lysis removes them from the host after therapy. 37
Anti-stem cell-based studies for the treatment of GBM
Recent studies defined either the normal signaling pathways or the clinical features of benign or malignant brain tumors and GSCs, which provide information about the marker or the therapeutic target of the brain tumors.
The transcription factor Bmi1 (Polycomb complex protein) has a major role in the proliferation of neural and hematopoietic stem cells. It regulates p16/INK, a cell cycle regulatory protein. During tumorigenesis, Bmi1 is required for cancer stem cell function and is generally overexpressed in brain tumors. 38 In addition, it is required for the malignant transformation of NSCs and astrocytes; high levels of Bmi1 expression facilitate high-grade gliomas in vivo, while low levels initiate or are associated with less malignant glioma. 39 Overexpression of Bmi1 causes uncontrolled cell division due to activation of p16/INK. Knockdown of Bmi1 might cause cessation of cell division.
The tumor suppressor gene PTEN (phosphatase and tensin homolog) is an important inhibitor of NSC proliferation and is mutated in human GBMs. The mutation of PTEN resulted in a lack of inhibition of NSC proliferation, 40 but there was a proliferation of stem cells. As mentioned earlier, the current treatment strategies focused on the bulk of the tumor. Due to stem cell proliferation, recurrence of tumor or resistance to therapy might be expected. The use of stem cells in association with conventional treatments may result in better prognosis of the patients.
Yang and colleagues used plasmid DNA via cationic polyurethane-short branch polyethylenimine (PU-PEI) to delivery tumor-suppressive microRNA145 within tumor, and demonstrated radiosensitization and chemosensitization of CSC-derived brain tumors and prolongation of animal survival after local intracranial injection of PU-PEI-miR145. Therefore, they showed that miR145 down-modulated the expression of Oct4 and Sox2 genes related to stemness feature. However, due to the absence of active cancer stem cells, this cancer stem cells (CSCs) targeting is still debated in clinical usages. 41
Tobias et al demonstrated that stem cell–based oncolytic therapy was well suited compared to chemoradiotherapy. They showed that the increased efficacy observed with combination therapy was dependent on the relative timing of administration and that NSCs loaded with CRAd-S-pk7 (CRAd-Survivin-pk7) should be given prior to XRT-TMZ therapy. They concluded that the potential radiosensitization induced by adenovirus infection might be a powerful tool for targeting therapeutically resistant tumor cells. 42
The other popular therapeutic target in GBM is EGFR, which is overexpressed in the majority of GBM tumors, including some of the CSC populations, and it is associated with tumorigenesis and aggressive phenotypes. A recent CSC-targeted study used cetuximab that binds to both the EGFR and EGFRvIII deletion mutant and demonstrated the in vivo efficacy of anti-EGF nanomedicine in GBM tumors. However, the fate of CSCs and the molecular basis for the observed therapeutic benefits are still unclear in this study. 43
Lee and colleagues tried to evaluate the safety outcomes of gene-directed enzyme prodrug therapy (GDEPT) in NSCs using double suicide genes. They confirmed the therapeutic efficacy of an NSC engineered with double suicide genes; HB1.F3-CD.TK was compared to NSCs with a single prodrug enzyme or untransfected controls. The viability or proliferation of the various NSCs was compared in vitro and in vivo to evaluate the degree of self-elimination of NSCs as a measure of safety. Lee and colleagues used an animal model of GBM and showed that HB1.F3-CD.TK had comparable therapeutic efficacy to its single gene counterpart, HB1.F3-CD. In vitro and in vivo tumor tropism and antitumor therapeutic effects of HB1.F3-CD.TK were also shown. Lee et al concluded that the double-prodrug enzyme-directed gene therapy showed good therapeutic efficacy as well as efficient eradication of NSCs to ensure safety for clinical applications of stem cell–based gene therapies. 44
Bao and colleagues targeted L1CAM by shRNA, which potently disrupts neurosphere formation, suppresses tumor growth, and increases the survival of mice bearing intracranial GBM xenografts. They found that L1CAM knockdown in vitro reduced the invasion potential of GBM stem cells and decreased the expression of invasion-associated proteins. They suggested that L1CAM played a crucial role in mediating GBM stem cell invasion and that L1CAM might represent a critical target for developing a novel anti-invasion strategy. They also hypothesized that L1CAM promoted GBM stem cell invasion and molecular targeting of L1CAM in GBM stem cells in vivo inhibits tumor invasion. 45 Lathia and colleagues demonstrated the tumorigenic potential of CSCs and non-stem tumor cells in the same microenvironment using a xenograft mouse model. Besides the tumor formation, they showed that a fraction of the initial transplanted CSCs maintained the expression of stem cells and proliferation markers, which were significantly higher compared to the non-stem tumor cell population, and further demonstrated that CSCs generated cellular heterogeneity within the tumor. 46 Galli et al. 47 isolated stem cell–like cells from GBM tissue and established tumors by orthotopic xenotransplantation in nude mice. Clarke et al studied in vitro models of tumor hypoxia with nude mice bearing intracranial U87-luciferase xenografts and showed the oxygen-induced radiosensitization of tumor tissue in GBM xenografts. The suppression of tumor growth and increased survival were also noted. They demonstrated that pretreating tumors with elevated levels of oxygen prior to radiotherapy might represent a means for selectively targeting radiation-resistant hypoxic cancer cells and could serve as a safe and effective adjuvant to radiation therapy for patients with GBM. 48
Current glioma therapies might fail to cure patients because of the glioma stem cell process mechanisms that evade treatments and enhance survival. The remaining cells that evade the therapy promote tumor regrowth. Furthermore, perivascular tumor cells and hypoxic conditions play a fundamental role in GBM growth and progression, and the hypoxic microenvironment induces angiogenesis, cell migration, and tumor resistance. This nature of the HIF represents a new molecular target to inhibit the malignant progression of GBM. The GSCs have potent angiogenic properties and can recruit vessels during tumorigenesis, because angiogenesis is a critical factor for the development and growth of GBM, and targeting the antiangiogenesis pathway decreases tumor cell proliferation and tumor size. Gene- and viral-based therapies have resulted in improvements in cancer treatment, and a number of anticancer genes have been successfully engineered into stem cells, which have promoted anticancer effects in various cancer models. Most of the studies on the use of stem cells in delivering the therapeutic genes mediated through lentiviruses, retroviruses, plasmids, and adenoviruses to treat multiple diseases including cancer showed promising results in animal trials by prolonging the life of the animal and reducing complications and/or tumor volume. The success of these treatments depends on selecting an appropriate method for gene delivery to the cells, and future treatment planning should be based on combinations of gene therapy and stem cell therapy. Genetic modification of stem cells with beneficial genes of interest is a prerequisite for the successful use of stem cell–based therapeutic applications in the future.
GSCs and therapeutic resistance
GBMs are highly infiltrative tumors that display extreme resistance to conventional radiotherapy and chemotherapy. Studies have shown that the GSCs contribute to therapeutic resistance6,14,49,50 because of the tumor heterogeneity. As the tumor contains different regions as mentioned above, there is a variation in the sensitivity of each region to the treatment; for example, the tumor periphery is highly sensitive to therapy, whereas the necrotic core or the intermediate core is resistant to treatment. 14 The region in which surgical resection is performed or radiotherapy is applied is very important because of the heterogeneous structure of the tumor.
GSCs represent important therapeutic targets because they have intrinsic machinery that overcomes current chemoradiotherapeutic approaches. Some of the molecular mechanisms underlying GSC resistance to chemoradiotherapy are discussed below. The discovery of GSCs may help explain the aggressiveness, relapse, and treatment resistance of GBM. The high DNA repair capacity and the increased resistance to radiation-induced apoptosis of GSCs compared to the non-stem tumor cells enable the GSCs to rapidly recover from the genotoxic stress. 6 This means that the treatment procedure that induces genotoxic stress is not the proper treatment choice for these tumors.
Recent studies showed that the low-molecular-weight inhibitor of Chk2 and Chk1 kinases relieves the radioresistance of GSCs and suggested that the targeted DNA damage checkpoint activation might sensitize these stem cells to radiotherapy. 6
Multiple molecular mechanisms regulate the radioresistance of GSCs. Recent studies suggested that targeting Sir T1 expression or HSP90 activity abates radioresistance of GSCs. The inhibition of the Notch signaling pathway by the γ-secretase inhibitor or Notch shRNA makes GSCs more sensitive to radiation. Notch pathway is another potential target for reducing GBM radioresistance, 6 and recent studies showed that GSCs can initiate gliomagenesis via activation of the Notch signaling pathway 5 ; if the Notch pathway is silenced or knocked down, the genes in this pathway may help to prevent tumor recurrence.
Active tumor angiogenesis is one of the hallmarks of the aggressive nature of GBM. GBM stem cells promote therapeutic resistance and metastasis and stimulate tumor angiogenesis by expressing elevated levels of VEGF that contribute to the tumor growth, which has been translated into a useful therapeutic strategy in the treatment of recurrent or progressive GBMs. GBMs rarely metastasize beyond the central nervous system; these highly infiltrative cancers often invade into normal brain tissues preventing surgical resection, and GBM stem cells display an aggressive phenotype. Targeting GBM stem cells may effectively reduce tumor recurrence and significantly improve GBM treatment. 6
Two groups of alkylating agents are commonly used for the treatment of GBM in the clinic: TMZ and nitrosoureas. MGMT is an important DNA repair enzyme that contributes to GBM resistance to temozolomide. The epigenetically mediated silencing of the MGMT gene in GBM has been shown to correlate with increased survival. Moreover, a correlation with outcome has been demonstrated independently of the treatment choice, ie, chemotherapy or radiotherapy. 51 Recent studies showed that MGMT status has no predictive value in primary GBMs. 52 Chemoresistance of GSCs was first investigated by Eramo et al. 53 Later, Beier et al. 54 described that TMZ may selectively deplete clonogenic and tumorigenic cells in a dose-dependent manner, whereas it hardly affected the overall viability, and the authors concluded that the cells with stem cell–like properties were selectively depleted, irrespective of the CD133 or MGMT status. Liu et al. 55 showed that CD133+ cells exhibited significantly less viability compared to CD133-tumor cells when treated with TMZ, and cells with methylated MGMT showed CD133 that exhibited stem cell–like properties. Pistollato et al. 11 showed an increased resistance of central, hypoxic CD133 CSCs, compared to cells derived from the periphery, due to increased MGMT expression. Bralten et al. 56 showed that no CD133 expression was detected in secondary GBMs, which are derived from lower grade gliomas, and suggested that IDH1 mutations are mostly found in secondary GBMs, which might inhibit the growth of GBM cells in vitro.
MGMT methylation occurs highly in secondary GBMs and can be used as a predictive marker for TMZ treatment. In the light of these data, we can safely assume that the GSCs that show higher CD133 expression and resistance to TMZ are the primary GBMs, which are directly derived from NSCs, and the tumors that show lower CD133 expression and treated successfully with TMZ are the secondary GBMs, which are derived from lower grade astrocytomas. On the other hand, restricted oxygen conditions elevate the CSC fraction and promote acquisition of a stem cell-like state such that multiple HIF-regulated genes are preferentially expressed in glioma stem cells in comparison to non-stem tumor cells and normal neural progenitors. When we look at the previous studies, Lai et al. 57 showed that GBMs with IDH mutation may originate from lineage-committed neural cells and gliomas without IDH mutation may arise from NSCs. IDH1 mutation is known to occur highly in secondary GBMs, which are derived from lower level astrocytomas. This means that IDH1 mutant, CD133–, and MGMT+ tumors are secondary GBMs, and CD133+ and IDH1 wild-type tumors are primary GBMs. If the mutant IDH1 appears on these tumors, it causes high hypoxia that, in turn, induces proliferation of GSCs, leading to resistance to the therapy. Several studies have demonstrated that GBM cells that are CD133 negative are still capable of tumor initiation, and some GBM tumors do not contain any CD133-positive cells.58–60 The reason for this situation is believed to be the precursor cell type from which the primary and secondary GBMs were developed into different progenitor cells and affect different genetic pathways (Fig. 1).
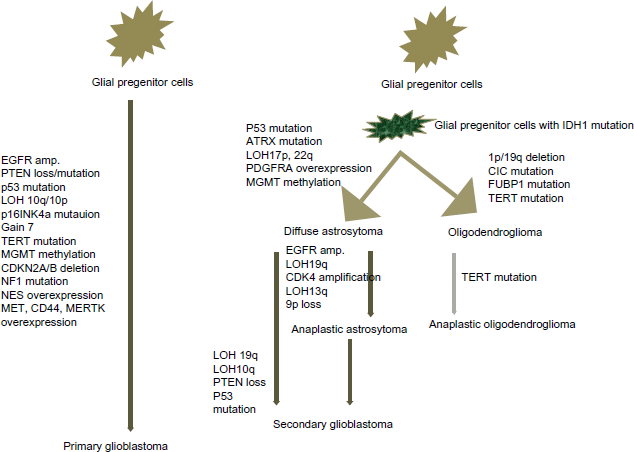
An illustration demonstrating the pathways of primary and secondary GBMs.
Hypoxia is common in many types of solid tumors. Hypoxic conditions have a negative impact on tumor growth. Hypoxia also enhances tumor progression and therapeutic resistance and promotes tumor angiogenesis and cancer invasion. The HIF1α and HIF2α control VEGF expression in GSCs. Hypoxia can promote the expansion of GSCs, prevent the differentiation of NSCs, and promote the maintenance of self-renewal potential of ESCs. 6 Heddleston et al. 61 showed that restricted oxygen conditions increase the expression of GSCs when glucose was used as a primary carbon source for mammalian tissues, but Metallo and colleagues showed that when IDH1 protein was knocked down, it mitigated the use of reductive glutamine metabolism for lipogenesis under hypoxia, 10 so that the cells survive and proliferate under hypoxic conditions. Hypoxia was associated with tumor growth, progression, and resistance of GBM to conventional therapy and also known to support the survival of nonneoplastic NSCs and GSCs, which confer drug resistance, self-renewal potential, and tumorigenicity in vivo (Fig. 2A). 62 Cancer stem cells in brain tumors reside in a perivascular niche that recapitulates a relationship between normal neural stem/progenitors and the vasculature, 1 which means that GSCs were maintained within a hypoxic niche; hypoxia plays a key role in the initiation, progression, and recurrence of GBM (Fig. 2B). On the other hand, the Notch pathway is essential for the hypoxia-mediated maintenance of GSCs; either depletion of HIFs or inactivation of Notch signaling partly inhibited the hypoxia-mediated maintenance of GSCs. Li et al. 63 showed that the hypoxic environment increased the expression of CD133 and nestin, which are markers of CSCs, but reduced the proportion of cells positive for glial fibrillary acidic protein, a marker for differentiation of stem cells. Li and colleagues concluded that hypoxia could dedifferentiate the differentiated glioma cells and promote the acquisition of stemness in these cells. But these in vitro and in vivo studies were performed to evaluate the specific mechanism of hypoxia and treatment resistance, and future studies will be aimed at identifying the target for the treatment of glioma.

Schematic representation of the effect of HIF on the progression of GBM. (
Conclusion
GBM is the one of the deadliest forms of cancer. The discovery of major genetic alterations in glioma progression has made a major contribution to our understanding of the molecular pathways involved in gliomagenesis. Current studies have focused on defining specific markers that facilitate the identification and isolation of the tumor in order to use these markers for a therapy target. In this review, we discussed the GSC phenotype, characteristics, and markers that are used to identify GSCs and the genetic basis of resistance to treatment. In the light of these observations, we have outlined strategies for the successful eradication of GSCs, including targeting the cellular pathways and cell surface markers. Finally, we summarized the therapeutic importance of these cells. Due to their high tumorigenic potential and resistance to current therapies, GSCs represent critical drug targets. We discussed hypoxia, GBM progression, initiation, recurrence, and maintenance of the phenotype of glioma stem cells under hypoxic conditions. Therefore, exploring the potential of combinational treatment strategies holds a great promise. The use of stem cells in combination with conventional treatments may show better prognosis. Furthermore, the treatment of GSCs using one's own autologous cells combined with suicidal gene therapies is a promising strategy forward. Future studies should focus on defining the HIF-mediated GSC survival and treatment procedures, leading to the possibility that HIFs could be a promising molecular target approach for GBM therapeutics.
Author Contributions
Conceived and designed the manuscript and wrote the manuscript: RK. The author reviewed and approved the final manuscript.