
Abstract
Background
Colon cancer is among the leading causes of cancer mortality and its incidence is increasing worldwide. This is true in spite of broad basic research into colon cancer while, concurrently, physical activity has been shown to offer significant preventive potential. This background led to the formulation of the following research questions:
Why is physical activity so effective in decreasing the incidence of colon cancer?
Is there a common denominator to colon cancer and physical activity, which has a reciprocal function?
Knowing the potential for public health impact of physical activity on colon cancer, has physical activity-colon cancer relationship been in the forefront of research efforts?
Methods
Content analysis of archival literature has been carried out on census of 32,822 message units, extracted from the National Library of Medicine and its PubMed database. The following search terms were used: colon cancer, physical activity, melatonin, age/genetics, diet (obesity, vitamin D, calcium), immunity/inflammation, and bioactive substances incorporating insulin-like growth factor 1, interleukins, and prostaglandins. The research timeframe for each category began with the first article published and ended with the last one printed in 2005.
Results/Conclusions
The effectiveness of physical activity in decreasing the incidence of colon cancer is likely the result of its biologic activity within not one or two but all of the major known colon cancer etiologies, demonstrating a powerful reciprocal relationship. Melatonin is identified as a plausible common denominator of colon cancer and physical activity. The greatest volume of publications deals with colon cancer and genetics. A significant societal health care impact could be achieved by adopting physical activity as a major cancer control strategy.
Introduction
The incidence of colon cancer is increasing worldwide. Ten million people developed colon cancer in 2000 and about five million died from this cancer. Many risk factors are known and include: diet, inadequate physical activity, obesity, alcohol consumption, and smoking, as well as family history and aging. The most prominent among the etiologic factors are physical inactivity and obesity, which are strongly and consistently associated with higher risk of colon cancer (Willer, 2003). Emmons et al. (2005) state that colorectal cancer (CRC) is the fourth leading cause of cancer and the second leading cause of cancer death in the United States.
A strong preventing influence of physical activity on colon cancer development has been well documented in the literature. The mechanisms of action, however, have been mostly hypothesized (Slattery et al. 1997; McTiernan et al. 1998; Thune and Furgber, 2001; Peters et al. 2001).
This study attempted to shed additional light on “how and why” a single preventive step, physical activity, can be so highly effective in lowering colon cancer incidence. A search has also been made to identify a plausible common denominator for colon cancer and physical activity that expresses reciprocal relationship.
Material and Methods
An archival literature research, through content analysis methodology, was chosen as the framework for this study. The three-dimensionality of this study had the following parameters: the breadth encompassed all articles published on topics extracted with specific key search terms of colon cancer, physical activity, melatonin, and related terms of age/genetics, diet (obesity, vitamin D, calcium), transit time plus immunity/inflammation, and bioactive substances incorporating insulin-like growth factor 1, interleukins, and prostaglandins. The depth of this methodology included a detailed examination of all relevant articles and a numerical summary of all message units, which included the key search terms and their combination. The methodological timeframe began with the first article published on a given topic and ended with the last one printed in 2005.
Data was collected through an electronic search of the National Library of Medicine's database, PubMed. Neudorf's outline of content analysis methodology was used allowing systematic, objective, and quantitative analysis of message units (Neuendorf, 2002).
A unit of data analysis in this study was represented by a single published article as generated by the PubMed database in response to the key word input.
Results
Physical activity was documented to exert its beneficial influence in all previously identified main colon cancer etiologic categories. Physical activity and colon cancer have a strong but reciprocal mutual relationship. With decreasing physical activity there is increasing incidence of colon cancer and vice versa.
Melatonin was identified as a plausible common denominator to colon cancer and physical activity due to the fact that it takes an active but reciprocal part in all colon cancer etiologic categories. It is diminished during cancer development but its level rises with moderate and strenuous physical activity.
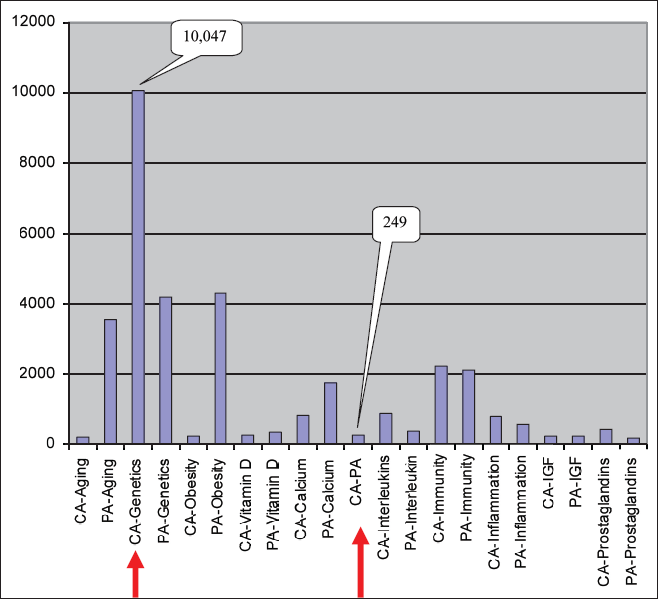
The numbers of publications identified are summarized in Figure 1. It illustrates that 10,047 articles were published on the topic of colon cancer and genetics but only 249 dealing with colon cancer and physical activity. Similarly, only 243 articles were published addressing colon cancer and obesity. The second highest volume of publications dealt with colon cancer and immunity. Figure 2 highlights the fact that physical activity takes part in all colon cancer etiologic categories. Under positive influence of physical activity, these categories become health benefit groups. The highest number of publications-4,288- dealt with physical activity and obesity. Figure 3 combined data for colon cancer and physical activity. It provides visual comparison of “what was studied” and to what extent. The gap between the 10,000 plus articles on colon cancer and genetics, and the only 200 plus publications related to physical activity and colon cancer is clearly evident. Colon cancer and obesity tracks only 200 plus publications.

Number of publications for search term combinations of colon cancer and etiologic categories including the first publication year.

Number of publications for search term combinations of physical activity and its health benefits categories including the first publication year.
Number of publications for search term combinations of colon cancer (CA) and etiologic categories, and physical activity (PA) and its health benefits categories including the first publication year.
Discussion
It has been quite revealing to look at the issue of colon cancer and physical activity through the method of content analysis. This process allowed for numerical and graphic comparisons of the research efforts of the scientific community studying the major colon cancer etiologic categories and the impact of physical activity within identical groups (Fig. 3). The major emphasis of researchers, as expressed by the highest number of publications, was found to be centered on the topic of genetics and colon cancer. Comparing the absolute numbers of publications-10,047 for genetics and colon cancer, and 249 for physical activity and colon cancer, the research effort into physical activity represents only about 2.5% of that expended on the field of genetics. Epidemiological data, however, suggest that the ration should probably be reversed in order to achieve the greatest societal health impact. This concept is based on reports that genetics play only a relatively small role in the etiology of colon cancers while it is estimated that physical activity could prevent 40–70% of colon cancers (Shephard and Shek, 1995; National Institute of Health, 2005; Fleet, 2006). If one considers a number of publications as a proxy to the effort and funding of the research community, a large discrepancy is apparent between the research into the genetics of colon cancer and the influence of physical activity.
A similar gap exists on the topic obesity-only 200 plus articles were found, while obesity is quoted to be one of the key causative factors of colon cancer (Willer, 2003). Slattery et al. (2005, p 148) also indicated that it is obesity, physical activity and energy intake that appeared to alter the risk of colorectal cancer while this risk appeared to be minimally influenced by genetic variants.
Batty and Thune (2000, p 1424) elaborated that physical activity has a marked effect on several functions of the human body that may influence cancer risk and that this association may vary across the life course. These effects, according to the authors, vary according to the mode, duration, frequency, and intensity of the activity which produce changes in bowel motility, endogenous hormones, energy balance, immune function and DNA repair. Also, Slattery and Potter (2002, p 913) wrote, that physical activity has been consistently but inversely associated with colon cancer incidence.
In real time, however, the individual etiologic factors do not work in isolation. Multifactorial influence seems to be the norm. For example, Fernandez et al. (2004) compared the effect of environmental factors and family history on the risk of developing colon cancer. For subjects without family history, they found that the odds ratio for colon cancer was 2.27; it reached 3.20 for those with family history and low risk factor score; and finally, for those with family history and high risk factor score, the odds ratio was 7.08.
Examining the individual etiologic categories also revealed some interesting observations. As Emmons et al. (2005) documented, there is a parallel aging-colon cancer relationship. This observation heralds that colon cancer incidence will continue to increase with its accompanying human and economic cost. This is due to the fact that, as The National Institute of Health (2005, p 1) reported, there is an evolving striking shifts in aging on a population scale. One pathway of influence, between aging and colon cancer, may be, as Shephard and Shek (1995, p 1) reported, the depression of immune function that is secondary to old age which is known to be associated with an enhanced susceptibility to tumors. These authors also demonstrated exercise-induced changes in the activity of macrophages, natural killer cells, lymphokine activated killer cells, neutrophils, and regulating cytokines suggesting that immunomodulation may contribute to the protective value of exercise. Along the same line, Johe and Osterud (2005, p 324) confirmed that physical exercise is associated with cellular activation of the blood cells.
Another negative societal shift that is evolving and predisposing a great number of people to colon cancer, according to Abu-Abid, Szold and Klausner (2004, p 73), is the fact that more than half of adult Americans are overweight or obese. Furthermore, it is of great concern that older children and adolescents in the United States currently do not achieve the recommended intake of calcium, as reported by Greer and Krebs (2006, p 578). Regular physical activity, on the other hand, provides health benefits, including the reduction in risk of colon cancer, and premature mortality, as documented by Belza and Warms (2004, p 181). Slattery et al. (2005, p 75) considered the degree of energy expenditure as an important factor in the etiology of colon cancer.
Vitamin D, as observed by Slattery et al (2004) who identified cellular vitamin D receptors, is involved in cell growth and differentiation. Freedman, Dosemeci, and McGlynn (2002, p 257) previously commented on the correlation between the exposure to sunlight and the mortality from female breast, ovarian, prostate, and colon cancer. Closely related to the issue of vitamin D and colon cancer is the impact of calcium. Fleet (2006, p 527), for example, indicates that colon cancer risk is reduced both by high dietary calcium consumption and high total dairy food intakes. He observed that dietary calcium and vitamin D status were comodulators of colon cancer and that vitamin D deficiency abolished the protective effects of calcium on tumor formation. Cosman (2005, p 73) argued that because bone loss with age is universal, its prevention requires adequate vitamin D intake and regular physical activity.
Inflammation is another suspected pathway leading to colon cancer. This is derived from observations similar to Clevers (2006, p 761) who points out, for example, that chronic inflammation of the intestine and colorectal cancer are closely associated and that the risk of colorectal cancer among patients with ulcerative colitis is an order of magnitude higher than the risk among those without it. Pertinent to the question of the role of inflammation in colon cancer etiology are also the observations on the effect of nonsteroidal anti-inflammatory drugs (NSAIDs) and the incidence of colon cancer. Potter (1999, p 916) summarized that NSAIDs, including aspirin, have been consistently associated with a reduced risk of colorectal cancer in rodents and that aspirin and celecoxib, a specific cyclooxygenase-2 [COX-2] inhibitor, restrained carcinogenesis. All the mechanisms by which physical activity may affect colon cancer are not clear, however. For example, Hou et al. (2004, p 860) considered interleukin 1 levels as playing an important role in the etiology of colon cancer, and Slattery et al. (2003, p 214) proposed that biologic mechanisms through which physical activity reduces the risk of colon cancer may involve altering prostaglandins levels. In addition, DeLellis et al. (2004, p 1444) confirmed that a high circulating concentration of insulin-like growth factor-1 (IGF-1) and the low circulating concentration of IGF binding protein-3 (IGFBP-3) have been associated with increased risk for several cancers including colorectal cancers. They also found a positive correlation between IGF-1 levels and colon cancer incidence rates within a multiethnic cohort for both sexes. Subsequently, it was Slattery et al. (2005, p 148) who noted that high serum IGF-1 levels are associated with an increased risk of colorectal cancer. Willer (2003, p 283) stated that increased physical activity and weight reduction increases IGF-1 binding protein production and therefore decrease IGF serum level thus diminishing the availability of free sex hormones, an effect that should further decrease the cancer risk. Hou et al. (2004, p 860) observed that physical activity is a strong determinant of insulin resistance and hyperinsulinemia, and that physical activity appears to modify insulin sensitivity.
Of note are also observations by Batty and Thune (2000, p 1424) regarding the fact that physical activity reduces the risk of colon cancer possibly even through the increase in bowel transit time and thereby the duration of contact between fecal carcinogens and colonic mucosa. Hou et al. (2004, p 860) has made similar observations. The increase of transit time, referred to by the authors, likely accompanies only moderate physical activity as intensive activity would diminish the intestinal transit.
Reiter and Robinson (1995, p 7; p 20; p 185) describe melatonin as a substance that plays a primary role in the body's defense against cancer and hence this substance was investigated for its possible relationship to colon cancer and physical activity. The connection of melatonin to the colon cancer etiologic categories and physical activity is highlighted with the following examples: Among its many functions, melatonin protects and enhances the immune system. As previously stated, there is a gradual crippling of the immune system that comes with age which parallels the known age-related decline of melatonin. Reiter and Robinson (1995) also state that calcium is vital for melatonin production thus connecting the vitamin D, calcium, melatonin and colon cancer. Das (2005, p 343) pointed out that calorie restriction which diminishes obesity also enhances melatonin production. Vijayalaxmi et al. (2002, p 2575) stated that the gut seems to produce proportionately more melatonin than does the pineal gland. In addition, they confirmed that melatonin markedly reduces acute inflammation and that it stimulates the production of interleukins. Knight and Thompson (2005, p 1114) confirm that exercise was found to be significantly related to an increase in melatonin production. This study was preceded by Poon et al. (1996, p 77) observation that melatonin binding sites were identified in the mucosa of the human colon. The brain center of circadian rhythm which is related to melatonin production is entrained by incoming light into the eyes; it is the lack of light during night time that allows for the production of beneficial melatonin. The undesirable resetting of the day/night rhythm can be generated by prostaglandin E2 (Tsuchiya et al. 2005). Physical activity lowers the levels of prostaglandin E2. Considering the above information, it seems reasonable to regard melatonin as a likely common denominator to colon cancer and physical activity. In the colon cancer etiologic categories, it is diminished, but with physical activity, its level is enhanced converting the etiologic categories into beneficial health impact groups.
The scientific literature continues to accumulate evidence that physical activity lessens the chances for colon cancer development. Zhang et al. (2006) found that twice per week engagement in recreational activity reduced colon cancer incidence by 30% for all sites, and 40% for the right colon. Those participants who had both high occupational and recreational physical activity experienced the lowest cancer risk (odds ratio of 0.5).
Much remains to be done to fully understand the reciprocal relationship of colon cancer and physical activity. Most recent articles, published by Campbell and McTiernan (Cambpell, McTiernan, 2007), made additional observations in this regard. They found decreases in serum estrogen, testosterone, and insulin in overweight, sedentary postmenopausal women with a 1 year exercise program (aerobic exercise, 45 min/d, 5 days/week). Furthermore, Campbell and co-investigators (Campbell et al. 2007) explored the expression of pro- and anti-apoptotic proteins in colon crypts. They found that the density of Bax, which is an apoptotic promoter, increases in the crypts following a 13-month program in male exercisers.
Conclusions
Colon cancer and physical activity operate through the same categories of influence, labeled either etiologic or health benefit categories, but with an opposite effect. Physical inactivity promotes metabolic abnormalities in each of the colon cancer etiologic categories, thus increasing the risk of colon cancer development. On the other hand, enhanced physical activity normalizes metabolic processes within all such categories, thus contributing to better health and lower cancer incidence. No other currently known colon cancer preventive step, besides physical activity, is involved in a reciprocal fashion with all the potential colon cancer etiologic categories. Societal health might benefit greatly if research effort into colon cancer was proportionate to the epidemiological evidence of its health impact.
This study also identified melatonin as a common denominator to colon cancer and physical activity exhibiting a beneficial and reciprocal relationship.