
Abstract
Objective
Stroke survivors often face barriers to structured physical activity due to physical or cognitive limitations. A recent feasibility trial of the mobile health (mHealth) version of the i-REBOUND programme (Internet-delivered Rehabilitation for Exercise after stroke) showed that it was safe, well-accepted, and accessible, but findings also highlighted aspects of the exercise support needing improvement. This study aimed to refine the mHealth version of i-REBOUND using a structured user-centred design (UCD) approach, and addressing limitations identified in prior feasibility testing.
Methods
This study applied a collaborative design that followed a three-phase UCD process: (1) review and preparation, using feasibility study data to identify key areas for refinement; (2) define and devise, conducting digital workshops and interviews with stroke survivors (n = 15) and physiotherapists (n = 3) to explore experiences and needs; and (3) develop and test, iteratively prototyping and user-testing modified exercise content based on phase 2 findings.
Results
Key refinements included (1) expanding the exercise components to include a variety of exercises, including seated and hemiplegia specific options; (2) developing new instructional content with embedded explanations of exercise purpose and difficulty modifications; and (3) creating prescribed physiotherapist-led exercise components in the same format as the supervised classes, enabling a more time- and personnel-efficient yet personalised delivery of the programme.
Conclusion
The refinements, such as seated and hemiplegia-specific exercise options and on-demand physiotherapist-led sessions, highlight how tailored mHealth solutions can better meet the needs of diverse stroke survivors and support sustained engagement. The collaborative process also highlighted the value of early and continuous user involvement.
Introduction
Stroke remains a leading cause of mortality and disability globally, with an estimated 12.2 million people affected each year. 1 Advances in acute stroke care have improved survival rates, 2 yet long-term functional impairments remain a challenge for many survivors.3,4 Secondary prevention strategies focus on reducing the risk of recurrent stroke, with international guidelines emphasising blood pressure management and lifestyle modifications, including increased physical activity. The Stroke Action Plan for Europe highlights the importance of accessible, long-term physical activity support to improve stroke outcomes. 5
Despite strong evidence supporting the role of physical activity in stroke recovery and secondary prevention,6,7 stroke survivors engage in low levels of physical activity, often spending < 10% of the day standing or walking and taking only 4000–5500 steps per day. 8 An important component of physical activity is structured physical exercise, 9 which, when delivered in a supervised format, has been shown to enhance cardiovascular health in people post stroke. 10 Still, engaging in physical exercise can be challenging for people post-stroke due to mobility limitations, fatigue, and lack of access to rehabilitation services.11,12 Supervised support, whether in-person or digitally delivered, may help stroke survivors safely engage in exercise and maintain long-term adherence.
Mobile health (mHealth), that is, utilising mobile devices and applications to deliver health services, 13 offers promising solutions for remote physical exercise through flexible access to structured exercise programs. mHealth interventions for stroke survivors have shown promise in certain health outcomes such as upper limb function and activities of daily living, 14 but their effectiveness in increasing physical activity remains uncertain and warrants further research. 15 While many stroke survivors with mild disabilities live independently, 16 they often require structured exercise support to prevent physical decline and maintain function. 17 mHealth interventions can offer this support remotely, yet few are tailored to users’ specific impairments or co-developed with them. A review of publicly available stroke apps found that most lacked end-user involvement in development, 18 despite guidelines emphasising participatory design to improve usability and effectiveness.19,20
User-centred design (UCD), 21 an approach that involves end-users throughout the development process to ensure the solution meets their needs and preferences, is particularly important in stroke populations, where cognitive, motor, perceptual, and communication impairments may affect how individuals engage with digital tools. Involving end-users throughout the design process ensures that mHealth solutions are not only usable, but also tailored to the diverse needs and functional abilities of stroke survivors. Recognising this, the Medical Research Council's (MRC) guidelines for complex intervention development 22 highlight the importance of engaging end-users throughout the intervention design process to enhance usability and real-world applicability.
This study builds on i-REBOUND – a telehealth exercise intervention initially developed in Australia.23,24 To facilitate adoption in Sweden, the intervention was adapted into an mHealth format, including the development of the Stroke Treatment Through Active and Accessible Rehabilitation (STAAR) mobile app. Exercise was provided via the STAAR app in the form of live, weekly, supervised sessions in an individual or group format and prescribed exercises in the form of exercise videos that could be accessed and performed when desired. The mHealth version of the i-REBOUND programme was recently shown to be feasible and acceptable to provide digital support for physical activity to people post stroke across Sweden. 25 The study included 118 participants with mild stroke or TIA and demonstrated high retention (92%) and adherence to the supervised exercise sessions (76%), with no adverse events reported. Participants generally rated the intervention as safe, accessible, and motivating. However, we observed a decline in use of the prescribed exercises over time and participants reported they were less relevant than the supervised exercise sessions. Physiotherapists also noted that delivering supervised sessions was resource-intensive and challenging to scale. Participant feedback reinforced the importance of refining the exercise components to enhance motivation, engagement, and adaptability to diverse functional abilities.
While previous mHealth exercise interventions for stroke survivors have shown promise, many have lacked structured co-development with end-users and have not adequately addressed the diverse functional needs of this population. In particular, few interventions have offered tailored support for both supervised and prescribed exercises that users can complete independently, or included adaptations for common stroke-related impairments such as hemiplegia or mobility limitations. To address these gaps, this study aimed to refine both the live supervised and on-demand prescribed exercise components of an existing mHealth intervention using a structured, multi-phase UCD process involving stroke survivors and physiotherapists throughout development to ensure the mHealth support meets their diverse needs.
Method
Study design and process
This study adopted a UCD approach, 21 aligning with user-centred recommendations for device technology development 26 and incorporating design thinking principles27,28 to refine the exercise component of an existing mHealth intervention. UCD and design thinking were selected due to their structured emphasis on iterative development, real-world testing, and deep user involvement, all essential for addressing the functional diversity and usability needs of stroke survivors. These approaches have been recommended for digital health intervention development and successfully applied in prior mHealth studies.21,29,30 These methodologies guided the study's three distinct phases: understand and review (Phase 1), where feasibility study data were analysed to identify key areas for refinement; define and devise (Phase 2), involving workshops and interviews with stroke survivors and physiotherapists to explore user needs; and develop and test (Phase 3), where refined exercise components were prototyped and user tested. An overview of these phases is provided in Figure 1.

The three phases of the user-centred process for refinement of the mobile health (mHealth) programme, mapped to the stages of design thinking.
The exercise components within the mHealth version of the i-REBOUND programme
The exercise component of the mHealth intervention was delivered via the STAAR app and included supervised exercise sessions and prescribed exercises. These exercise formats are detailed in a previous publication 31 and summarised here.
Supervised exercise sessions were live video sessions accessed via the STAAR app, offered individually or in groups of up to four participants supervised by a physiotherapist. The sessions, all lasting 20 minutes, aimed to elevate heart rate to at least a moderate intensity. Given the variability in disability and physical function among stroke survivors, exercises were tailored across three difficulty levels (1–3), with groups formed based on the level assigned. All sessions, regardless of level, included four 5-minute blocks, which followed an interval format, alternating between a more demanding exercise and active rest. Levels progressed by interval length of the demanding exercise (Level 1 = 30 seconds, Level 2 = 45 seconds and Level 3 = 60 seconds) as well as differed in the type of exercises performed.
Prescribed exercises were designed as a complement to the supervised exercise sessions, providing participants with additional training opportunities to complete at their convenience. These were short, pre-recorded videos showing functional strength exercises performed by one of three individuals demonstrating the exercise (demonstrators). None of these demonstrators were physiotherapists but instead were performed by people varying in age, background and disability status post stroke. Exercises differed from those performed in the supervised exercise sessions in that they were slower paced with a focus on muscular strength training. A visual analogue scale (VAS) of reported pain (0 = no pain, 100 = worst pain imaginable) was optional to complete before and after the session.
Research team
This study was performed by a core project group responsible for the overall development, planning and running of workshops and production of prototypes. This group included two researchers (SH and DMC) and a physiotherapist with experience in mHealth-supported physical exercise for people post-stroke. A wider multidisciplinary team (with expertise within stroke rehabilitation, physiotherapy and occupational therapy, mHealth intervention development, and physical activity research) was consulted at various points in the process for further input.
Study participants
Stroke survivors were recruited from the feasibility trial with previous experience of the mHealth version of i-REBOUND or via advertisements from patient organisations in Sweden without prior experience of the programme. Recruitment was purposive to capture variation in mobility, prior program experience, and demographics. Criteria for participation were based on criteria from the feasibility trial, which included: > 18 years old, a clinically confirmed diagnosis of stroke or TIA, being able to walk in short bursts independently indoors, with or without a walking aid, and access to a smartphone, tablet device or computer with internet connection. Physiotherapists were recruited through advertisements in the Stroke and Neurological associations, or through word of mouth in the Stockholm rehabilitation clinics. The main inclusion criterion for physiotherapists recruited to workshops included working or previously working clinically within stroke rehabilitation. Eligibility screening was conducted based on self-reported information provided by participants at sign-up and collected via a telephone interview by a member of the project group. This information included the year of the most recent (if applicable) stroke, a description of mobility indoors and outdoors, including the type of walking aid used. The research team reviewed this information if the participant didn’t fully meet the mobility criterion, since no formal testing of the exercise material was required.
This study was conducted in Sweden between 2022 and 2024. The ethical review board committee in Stockholm approved this study prior (Dnr 2022-06896-01 and 2024-04655-02). All participants were provided with study information and provided formal written informed consent.
Phase 1: Review and prepare
The goal of Phase 1 was to analyse prior feasibility study findings of the mHealth version of the i-REBOUND programme and define key areas for improvement regarding mHealth-supported exercise. Weekly project team discussions were used to review participant feedback and feasibility study data. Through this, the core project group aimed to develop a clear set of themes and topics related to the exercise components to bring forward to Phase 2 workshops.
Workshop themes and content identification
Project group meetings that focused on understanding user needs and contextual factors were undertaken ahead of workshop planning. This step was important for understanding the diversity of participants and their varied needs relating to the exercise components.
Workshop themes and topics were derived from feedback and data from the feasibility trial. 25 Qualitative data sources, including interviews, researcher logs, and participant interactions, were reviewed to gather an idea of the problem/s related to the exercise components. As a general starting point, the project group participated in group discussions with a focus on physical exercise components of the intervention in the feasibility trial and data sources were reviewed by the core team to identify recurring barriers and themes. These discussions were followed by a round of brainstorming to map out possible workshop themes. A thematic grouping approach was used to synthesise feedback and guide workshop topic development.
The workshop themes were designed to facilitate participation and discussion for both groups and were categorised into supervised exercise and prescribed exercise before delving into more specific themes and topics. The project team conducted multiple review rounds to finalise the themes and content.
Phase 1 results: Key areas for refinement
Findings from the project group meetings informed the key themes for end-user workshops, as outlined in Table 1. The areas for improvement in the exercise components that were highlighted in the feasibility study were as follows: First, supervised exercise sessions were widely utilised and appreciated, but physiotherapists frequently cited time and resource demands. Additionally, there was a need for greater variation in exercise content over the sessions. Second, the prescribed exercises were largely underutilised by participants, underscoring the importance of exploring the reasons behind this and identifying strategies to enhance their engagement and adherence. Themes and topics were divided into workshops with a focus on these findings and split into (1) supervised exercise sessions and (2) prescribed exercises.
Breakdown of workshop themes and topics as decided during project group discussions and based on various data sources from the feasibility trial.

Phase 2: Define and devise
Phase 2 aimed to explore end-users’ perspectives on the exercise components, including both the supervised sessions and prescribed exercises, with each following a distinct refinement process based on the issues identified in Phase 1. Interviews and workshops were conducted separately for the prescribed exercises and the supervised sessions, each reflecting their distinct processes.
For the supervised sessions, the focus was on refining the live, group-based sessions, including variations in exercise intensity, duration, and accessibility. In contrast, the prescribed exercises required different considerations, such as improving instructional clarity and making the exercises more adaptable to users’ needs.
Workshops with people post-stroke
To capture diverse perspectives on mHealth-supported physical exercise, this study included both former participants of the feasibility trial and individuals new to the intervention. Participants were divided into three groups (approximately 5 participants per group) for a total of nine workshops. One of these groups consisted solely of participants with previous experience of the mHealth version of the i-REBOUND programme to allow for experience-specific discussions. The remaining participants had no prior experience with the intervention and were assigned to one of the two remaining workshop groups, with the aim of ensuring a mix of demographics, disability levels, and other relevant characteristics to facilitate varied discussions. Workshops, facilitated by two project team members (SH and DMC), followed a structured format, including brief presentations by researchers, guided discussions, and brainstorming exercises. Each workshop lasted ∼ 2 hours and was conducted over Zoom. Sessions were recorded, transcribed and detailed notes were taken. Facilitators ensured that all participants were invited to share their views, aiming to minimise dominance effects and promote inclusive participation. Participants accessed example videos via the STAAR app to facilitate informed discussions. Participant demographics and stroke-related information were collected via questionnaires in the app prior to the first workshops. Standardised questionnaires included the Walk 12 questionnaire 32 and Fatigue Severity Scale (FSS 9-version item). 33
Individual interviews with people post-stroke
Following the workshops, stroke survivor participants were invited to test the STAAR app, including some prescribed exercises, and provide individual feedback. Exercises were matched to participant mobility status (e.g. independent ambulators/or dependence on a walking aid) screened over the telephone by a physiotherapist. Participants post-stroke were encouraged to watch exercise videos and, optionally, perform the exercises. Two weeks later, semi-structured interviews were conducted to assess perceived relevance, current exercise format, pace, instructional clarity, exercise demonstrator, and difficulty level. Responses were rated on an ordinal scale from 0 (do not agree at all) to 10 (completely agree), followed by open-ended questions. Qualitative responses from workshops and interviews were analysed using thematic grouping. Notes and transcripts were reviewed by the core research team, and user feedback was iteratively discussed and organised into themes and user requirements through team-based consensus. No formal coding software was used, but recurring ideas were documented systematically and reviewed across researchers to ensure consistency. Quantitative data from rating scales were summarised descriptively (mean and range), and interpreted alongside qualitative insights to inform the prioritisation of user requirements.
Workshop with physiotherapists working in stroke rehabilitation
A separate digital workshop was conducted with three physiotherapists working in stroke rehabilitation. This session explored professional end-user needs related to delivering an mHealth intervention for physical exercise and addressing diverse patient needs. The workshop followed the same structured discussion format as the stroke survivor sessions.
User requirements and prioritisation
Findings from workshops and interviews were summarised and then compiled to form a list of requirements relating to the exercise components. User requirements were compiled, discussed, and prioritised by the research team. Prioritisation was categorised as (1) needed immediately, (2) needed but can wait, (3) nice to have, or (4) outside study scope. Prioritisation was based on frequency of mention, perceived impact on user experience, and feasibility of implementation into the programme. Items discussed by multiple participants and with clear alignment to engagement or accessibility were typically rated as ‘needed immediately’.
Ideation – brainstorming and discussions
Once the research team had agreed on the list of requirements, several brainstorming sessions and discussions were carried out by the research team. This stage of Phase 2 involved building ideas for the mHealth exercise components development based on the requirements from end-users and designing new content for later prototyping. These ideas became solidified after several rounds of discussion. Once these were agreed upon, a plan for the next phase was created.
Phase 2 results: User requirements and prioritisation
A total of 18 participants were recruited and included in at least one workshop. Of these participants, 15 were stroke survivors (see Table 2 for detailed characteristics of stroke survivors), and three participants were physiotherapists working within neurological rehabilitation. The stroke survivors had a mean age of 63 years (range: 34–78), 60% were women and 67% reported using a walking aid. The majority (93%) spoke Swedish as their first language, and education levels varied, with 40% holding a university degree.
Workshop demographic, clinical and background information for stroke survivors participating in the workshops.

Themes that emerged from the workshops and interviews with stroke survivors were analysed and grouped into user requirements, which were then prioritised and refined into actionable solutions. The final prioritised requirements and corresponding proposed solutions are summarised in Table 3. Main findings regarding the supervised exercise sessions where the need for greater variation in class content and level of difficulty to accommodate participants with reduced mobility or difficulty performing standing exercises. Additionally, some participants – specifically stroke survivors with previous experience of the mHealth intervention – expressed a desire for supervised classes to be available as prescribed exercise classes (e.g. as pre-recorded videos guided by physiotherapists), allowing for greater flexibility and accessibility. Stroke survivors also emphasised the need for more variation in difficulty levels, clearer guidance on the purpose of each exercise (e.g. targeted muscle groups and relevance to daily activities), and more detailed instructions on how to perform the exercises correctly.
The prioritised user requirements that were considered essential (‘needed’) and the proposed solutions developed during the ideation phase.
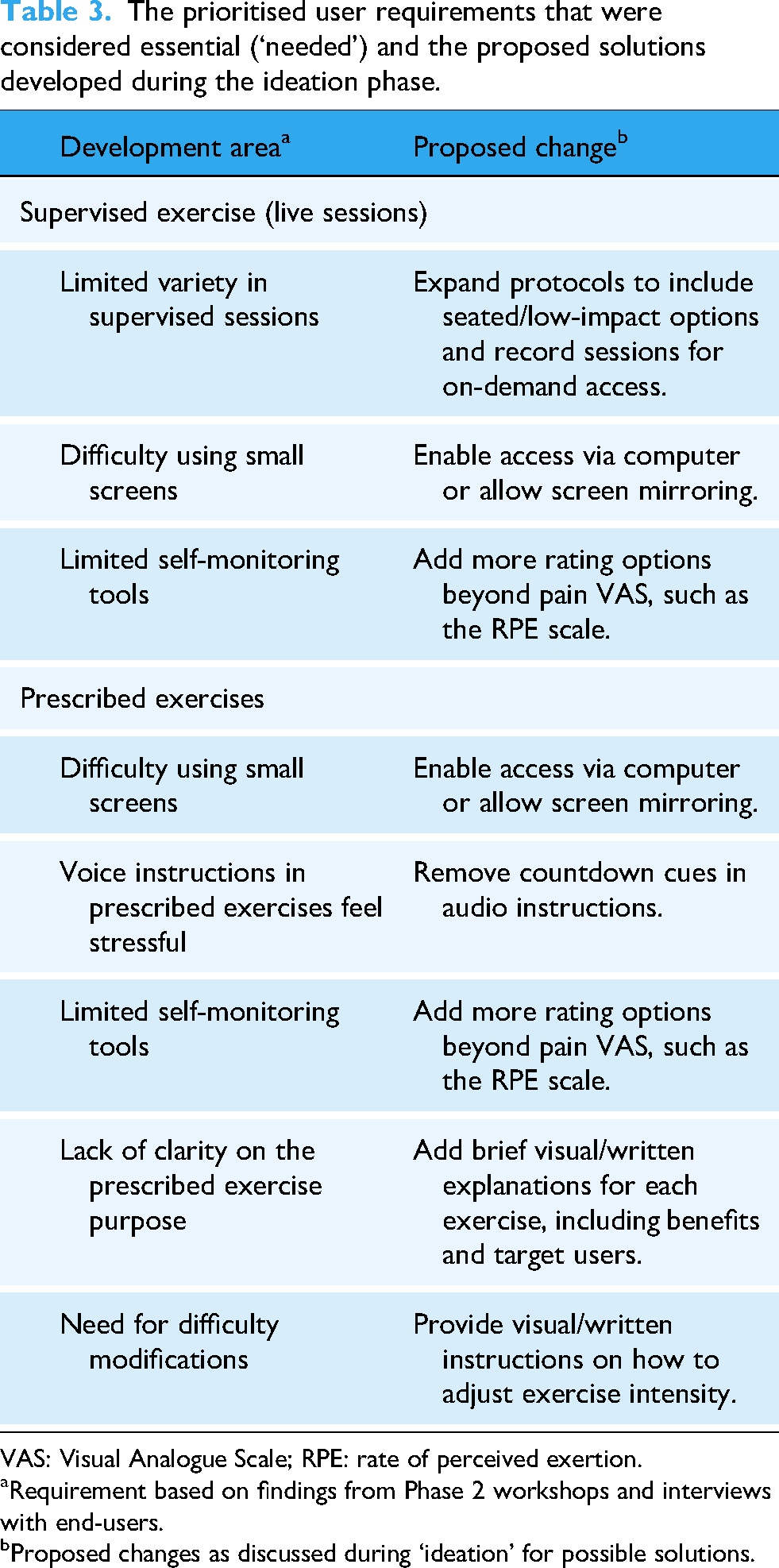
VAS: Visual Analogue Scale; RPE: rate of perceived exertion.
Requirement based on findings from Phase 2 workshops and interviews with end-users.
Proposed changes as discussed during ‘ideation’ for possible solutions.
Findings from the workshop with physiotherapists highlighted the importance of adherence to mHealth support for exercise in general and progression and safety aspects when exercising through mHealth technologies compared to in-clinic.
User requirements and prioritisation
All requirements deemed ‘needed’ were taken forward to ideation for suggestions on how to overcome or improve these problems.
Ideation – brainstorming and discussions
Solutions focused on content creation while also considering modifications to existing materials. These included both app-based solutions, such as developing new digital content within the app, and program-related improvements.
Phase 3: Develop and test
Prototyping and user testing
Building on the prioritised user requirements identified in Phase 2, multiple new elements were developed for testing and refinement. Prototyping involved an iterative process combining content creation, design modifications, and technical integration within the STAAR app. The project team developed and refined exercise protocols, designed new instructional materials, and recorded videos to enhance the intervention. This included scripting and filming exercise demonstrations, creating instructional voiceovers, and refining visual elements. Multiple prototype versions were produced and integrated into the STAAR app for user testing.
All participants from the previous workshops in Phase 2 were invited to evaluate prototypes through follow-up interviews or a final full-group workshop. The workshop included two types of feedback: a traffic light system (green = positive, orange = promising but needs refinement, and red = needs major revision) and A/B-style testing, where participants viewed two different versions of prototype elements but were not explicitly told the difference (e.g. voiceover styles) and asked to indicate their preference. 34 For the traffic light system, feedback categorised as ‘green’ was typically retained with minimal changes, ‘orange’ elements were flagged for revision or clarification, and ‘red’ items were either substantially redesigned or removed. This colour-coded system helped the team quickly prioritise which elements required iterative refinement. A/B comparisons were shown sequentially, and participants provided written and verbal feedback on which version they preferred and why. This input was discussed thematically.
As part of Phase 3, individual interviews were conducted to assess the acceptability and opinions of the prototypes developed based on Phase 2 findings. While the Phase 2 interviews specifically focused on prescribed exercises, Phase 3 introduced the opportunity for stroke survivors to test supervised classes in a prescribed format, on demand. This adjustment emerged directly from feedback in Phase 2 workshops, where participants indicated a desire for greater flexibility in accessing supervised exercise sessions. In the Phase 3 individual interviews, we used the same testing method as in Phase 2, but with a different format for the exercises. Participants tested these on-demand sessions individually, allowing for a deeper understanding of how the shift from live supervised sessions to prescribed, on-demand availability impacted their experience.
Phase 3 results: User testing of prototypes
Table 4 presents the prototype created, how the prototype was user-tested and the feedback received for both the supervised exercises and the prescribed exercises. Figure 2 shows an example of the prototype creation process specific to prototype number 1 in Table 4. Out of the 15 stroke survivor participants, 13 took part in the Phase 3 testing and interviews.

A shows an example of recording new material for prototype testing in the studio, B and C show how the prototype was presented in the Stroke Treatment Through Active and Accessible Rehabilitation (STAAR) app for user testing.
Summary of user testing and feedback on exercise video prototypes.

Supervised exercise (live sessions)
The main development involved a revised and extended supervised exercise protocol, which is detailed in Supplemental Material 1. The updated protocol expanded the original three-level structure to four levels. The new format includes multiple sub-levels within each level that vary in session duration and intensity. Key improvements to the protocol include (1) a new entry-level (Level 1.0) focused on seated exercises to enhance inclusivity for stroke survivors with impaired mobility, (2) greater variation in session duration and number of exercises across sub-levels, (3) three different versions of each session at each level to reduce repetition and enhance engagement, and (4) an exercise program of each level adapted for participants with hemiplegia. These updates were designed to improve inclusivity, accommodate a wider range of physical abilities, and support individual progression through the program.
Furthermore, we also recorded a new form of exercise videos that were similar in style to the original supervised exercise sessions at 20 minutes per session, with three possible levels (1–3) and a low-impact session version of level 2 specific for knee pain, with reduced strain on joints. Participants highly valued the ability to access supervised exercise in a prescribed format, instructed by a physiotherapist, which blended elements of the prescribed exercise and supervised sessions. Following feedback, these were amended and made to follow the new protocol, which included variation in exercises, levels and length of sessions as well as hemiplegia-specific exercises for those with difficulty performing bilateral exercises. Table 4 highlights these prototypes and the feedback received in user testing. An illustration of a prototype during development is shown in Figure 2. See Supplemental Material 2 for participant ratings of this prototype from individual interviews.
Prescribed exercises
The main prototype that was developed relating to prescribed exercise was an introduction video, designed to be added at the start of each exercise video. It explained the purpose and the importance of the exercise and offered suggestions for variations and adjustments. This video was found to be clear and easy to follow, and it was well-received by participants across ability levels. The inclusion of exercise adaptation options for individuals with post-stroke disabilities was particularly appreciated.
Additionally, two voiceover prototypes were created for the exercise instructions: one with a more enthusiastic and encouraging tone, and another with a calm, purely instructional delivery. While some participants did not notice a significant difference between the versions, others had distinct preferences, highlighting that individual variation exists. Overall, clarity was considered the most important aspect of the voiceover. With this in mind, we decided not to proceed with further development of the voiceovers during this refinement cycle. Given the divergent preferences, further work (such as developing a prototype with a clearer yet neutral tone and returning to user testing) would be needed to arrive at a more acceptable solution. However, this was outside the scope and time frame of the current study.
Discussion
This study's development and refinement of the mHealth version of the iREBOUND programme highlight the value of iterative, user-centred, and participatory methods to ensure the intervention meets the needs, preferences, and capabilities of stroke survivors. Engaging stroke survivors and physiotherapists in the design and testing phases provided valuable insights into how mHealth solutions can better accommodate user needs. This may ultimately improve adherence and engagement, which could, in turn, enhance the effectiveness of mHealth-supported exercise interventions. The study aligns with existing literature that emphasises the need for tailored interventions to support long-term secondary stroke prevention through physical activity promotion.29,30
The integration of UCD principles ensured that refined mHealth support for exercise was not only based on clinical recommendations but also shaped by the real-world experiences of stroke survivors. The workshop findings and feasibility trial feedback revealed several critical aspects that needed improvement, including the variety and adaptability of exercise content, ease of access to digital tools, and the integration of features that support autonomy and self-monitoring.
Key modifications derived from the workshops include increasing the variety of supervised and prescribed exercises, offering customisable exercise options, and improving accessibility by allowing access on larger screens, such as computers. Similar needs have been identified in digital interventions for other populations living with neurological conditions such as multiple sclerosis and Parkinson's disease, where users also report valuing adaptable content, clear instructions, and accessibility features to support digital engagement.35–37 Additionally, feedback highlighted the importance of clear instructional content, including explanations of exercise benefits, which was subsequently integrated into the intervention. These changes mirror broader trends in digital health interventions, where user experience and ease of access significantly impact engagement.
The successful implementation of mHealth interventions for stroke survivors requires addressing both technological and behavioural challenges. Stroke-related motor, cognitive, visual, and perceptual impairments,19,20 can reduce usability and engagement with digital health tools. This underscores the importance of intuitive design, strong accessibility features, and tailored content delivery. 38 Studies have shown that user experience and ease of access significantly impact engagement in digital health interventions, with optimised interfaces and clear guidance improving adherence. 39 In this study, the two exercise modalities – supervised and prescribed exercises – emerged as complementary components in supporting long-term engagement. Supervised sessions focused on structured, interactive support, whereas on-demand prescribed exercises offered flexibility and self-paced progression. Both formats catered to most stroke survivors, regardless of disability. This dual-modality approach for exercise support aligns with broader trends in digital health. Blended delivery models that combine human-delivered and digitally delivered care have been shown to improve access and enhance care quality. 40
A recurring theme from reviewing the feasibility findings in Phase 1 was the underutilisation of prescribed exercise videos compared to supervised sessions. This finding suggests that while mHealth interventions can facilitate physical activity engagement, they must also address motivational and behavioural factors influencing adherence. The introduction of structured video content with embedded explanations and difficulty modifications was a direct response to these barriers. Furthermore, features such as countdown timers and self-monitoring tools (e.g. Borg scale) could be included to enhance user control and encourage self-efficacy. Future iterations should further explore how integrating behavioural change techniques—such as goal setting, real-time feedback, and social support mechanisms—can enhance engagement and long-term adherence. 41 These insights contribute to a growing body of evidence on optimising mHealth for stroke rehabilitation, 42 emphasising that digital interventions should not only facilitate exercise participation but also support a person's transition from structured rehabilitation to long-term self-management of physical activity.
While the intervention was developed within a Swedish context, many of the identified needs, such as flexibility, clarity, and adaptation for disability, are relevant across healthcare systems worldwide. However, transferability may be influenced by contextual factors. For instance, Sweden has a high level of digital literacy and widespread use of digital identification tools like BankID, which may not be the case in all settings. Similarly, the feasibility of implementing digital exercise support may depend on the availability of physiotherapists to deliver or supervise such services. These healthcare system differences should be considered in future studies aiming to adapt or implement similar approaches in other countries.
Strengths and limitations
One of the primary strengths of this study is its methodological rigor, particularly the incorporation of UCD and participatory design principles. This study extends previous work on mHealth exercise interventions for stroke survivors by applying a structured, three-phase user-centred design process involving both stroke survivors and physiotherapists. The level of user involvement throughout the development process, spanning review, ideation, and prototype testing, distinguishes this work from prior studies. Moreover, the refinements addressed both supervised and prescribed exercise components, resulting in a dual-modality approach tailored to stroke-related impairments, including hemiplegia-specific adaptations, seated protocols, and on-demand physiotherapist-led sessions. Digital exercise solutions often lack the flexibility to accommodate personalised or specialised needs. However, the structured, participatory design approach used in this study may support more effective integration of the refined intervention into existing stroke rehabilitation services.
Additionally, the iterative nature of the study ensured that feedback loops were integrated into the design, allowing for continuous improvement. Another strength is the practical value of these refinements. By enabling physiotherapist-led sessions to be accessed on demand in a standardised format, the programme offers a more time and personnel-efficient mode of delivery compared with traditional approaches. These features, alongside the expanded variety of exercises and seated/hemiplegia-specific adaptations, may help support sustained engagement among stroke survivors over the long term.
However, some limitations should be acknowledged. First, while the study leveraged digital workshops and user testing, in-person evaluations might have provided additional insights into usability and engagement in a real-world setting. Second, the study focuses on the refinement and short-term testing of the mHealth intervention. Long-term adherence to the exercise program and its sustained impact on physical activity and health outcomes were not assessed, which could be important for evaluating the intervention's effectiveness over time. Additionally, participants may have been more motivated or digitally engaged than the broader stroke population due to a potential self-selection bias. Moreover, much of the feedback was self-reported, which could be influenced by recall or social desirability bias. The study sample included only independently mobile stroke survivors, which may limit generalisability to those with more severe impairments. Lastly, implementing certain features, such as customisable voice instructions or more advanced self-monitoring tools, may be challenging due to resource constraints. This could limit the scalability and practicality of the intervention.
The refinements tested here may have practical implications for rehabilitation services. For example, on-demand physiotherapist-led sessions could be incorporated into community-based or hospital-based programmes as a complement to in-person care, potentially easing physiotherapist workload while maintaining individualisation. Seated protocols and hemiplegia-specific adaptations could broaden access for stroke survivors with reduced mobility, thereby extending the reach of rehabilitation services without necessarily increasing personnel resources. However, the intervention was developed with mobile-using stroke survivors who were independently mobile, and transferability to patients with more severe impairments or lower digital literacy may be limited. Future work should evaluate adaptations for those with higher support needs and consider equity of access where digital infrastructure is less established.
Future research should evaluate the scalability of the intervention within different healthcare contexts, including settings with varying levels of digital infrastructure and physiotherapy availability. Randomised controlled trials are needed to assess the effectiveness of the refined programme on long-term adherence to physical activity, functional outcomes, and even health-related quality of life. Additionally, longitudinal implementation studies could explore real-world uptake, sustainability, and cost-effectiveness.
Conclusions
This study underscores the critical role of user involvement in the development and refinement of mHealth interventions for exercise support following stroke. The prototypes developed in response to user feedback focused on increasing content variety, offering customisable exercise options, and improving accessibility through clear instructions. These refinements directly address the barriers to long-term engagement and personalisation identified in the feasibility study, thus improving accessibility, usability, and motivational support for stroke survivors using mHealth-delivered exercise. These findings contribute to the growing body of evidence supporting the integration of mHealth technologies into stroke rehabilitation and highlight the potential for digital tools to bridge gaps in post-stroke care. Longitudinal implementation studies based on the study's findings could explore real-world uptake, sustainability, and cost-effectiveness, which will be critical to inform policy and practice.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076251387052 - Supplemental material for Refining mHealth exercise support for stroke survivors: A user-centred design approach
Supplemental material, sj-pdf-1-dhj-10.1177_20552076251387052 for Refining mHealth exercise support for stroke survivors: A user-centred design approach by Sophia Humphries and David Moulaee Conradsson in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076251387052 - Supplemental material for Refining mHealth exercise support for stroke survivors: A user-centred design approach
Supplemental material, sj-docx-2-dhj-10.1177_20552076251387052 for Refining mHealth exercise support for stroke survivors: A user-centred design approach by Sophia Humphries and David Moulaee Conradsson in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors would like to thank Frida Wallén and Annett Johansson for their extraordinary help and involvement with this project. We would also like to thank our workshop participants for their invaluable input.
Ethical considerations
The ethical review board committee in Stockholm approved this study prior (Dnr 2022-06896-01 and 2024-04655-02).
Consent to participate
All participants were provided with study information and provided formal written informed consent.
Consent for publication
Informed consent for publication was provided.
Authors’ contributions
Both authors contributed to the conceptualization, investigation, methodology and reviewing and editing of the article. SH was solely responsible for writing the original draft and overseeing the project administration. DMC was responsible for supervising the project and external oversight.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Swedish Stroke Foundation [2022-06896-01] and Stiftelsen Promobilia [A22135].
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article, as no datasets were generated or analysed during the current study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.