
Abstract
Introduction
This multicenter phase II study determined the efficacy and safety of new daily oral S-1 and weekly irinotecan (CPT-11) combination schedule in patients with previously untreated advanced or recurrent colorectal cancer.
Patients and Methods
Patients received first-line chemotherapy comprising S-1 80 mg/m2/day given on days 3 to 7, 10 to 14, and 17 to 21 and 60 mg/m2 CPT-11 administered intravenously on days 1, 8, and 15 of a 28-day cycle.
Results
A total of 45 eligible patients were enrolled in this study. The overall response rate was 48.9%. Median progression-free survival and median overall survival was 8.1 months and 20.9 months, respectively. The rates of grade 3 or 4 toxicity were as follows: neutropenia, 8.9%; anemia, 4.4%; anorexia, 6.7%; and diarrhea, 6.7%.
Conclusions
This new S-1 and irinotecan combination schedule appeared to be an effective, well-tolerated, and convenient regimen in patients with advanced colorectal cancer as compared with conventional regimens such as FOLFIRI and IRIS.
Keywords
Introduction
Irinotecan (CPT-11) is a key drug in the management of metastatic colorectal cancer as demonstrated by several randomized studies indicating a survival benefit. It was shown that the response rate to CPT-11 was 11% to 25% in patients with advanced colorectal cancer refractory to 5-fluorouracil (5-FU)-based chemotherapy.1,2 These findings implied a lack in tumor cross-resistance between the two agents CPT-11 and 5-FU. Moreover, favorable results from combination chemotherapy using CPT-11 and 5-FU/leucovorin (LV) for advanced colorectal cancer have been reported.3,4 A CPT-11 and infusion plus bolus 5-FU/LV regimen (FOLFIRI) with or without biologics has been recommended as first-line therapy for advanced colorectal cancer. FOLFOX regimens which add oxaliplatin to intravenous 5-FU/LV have also been recommended. 5 These regimens consist of the conventional maximum tolerated dosage (MTD) of CPT-11 and 5-FU. Consequently, grade 3 or worse adverse effects are not uncommon. Moreover, administration of infusion 5-FU is becoming more complex because of the need for vascular access devices and a portable delivery system.
Dihydropyrimidine dehydrogenase (DPD)-inhibitory fuoropyrimidine (DIF) compounds such as UFT and S-1 have been developed in an attempt to resolve the issue of the rapid reduction in 5–FU by DPD. S-1 is an new oral DIF developed by Taiho Pharmaceutical Co., Ltd. (Tokyo, Japan) that combines tegafur with two 5-FU modulators, 5-chloro-2,4-dihydrooxy-pyridine (CDHP), and potassium oxonate (Oxo) in a molar ratio of 1:0.4:1. 6 Tegafur, a prodrug of 5-FU, is converted to 5-FU mainly in the liver and in the tumor cells. CDHP, a reversible inhibitor of DPD, suppresses the degradation of 5-FU, thereby maintaining high concentrations of 5-FU in plasma and the tumor cells.6,7 CDHP also decreases the cardiotoxic and neurotoxic effects by reducing the production of F-beta-alanine (FBAL), the main catabolite of 5-FU.8.9 After peroral administration, Oxo is selectively distributed to the small and large bowels. High concentrations of Oxo in these organs inhibit the phosphorylation of 5-FU to fuoropyrimidine monophasphate, catabolized by orotate phosphoribosyltransferase within the gastrointestinal mucosal cells, thereby reducing the incidence of diarrhea. 10 DPD is approximately 180 times more potent than the DPD inhibitor uracil, which is a component of UFT. Thus, S-1 results in higher concentrations of 5-FU in the blood and tumor tissue than UFT. 11 Because S-1 is thought to be more potent than UFT with respect to the biochemical modulation effect, one might expect a stronger antitumor effect of S-1.
In phase II trials of S-1 as a single agent in patients with advanced colorectal cancer, response rates ranging from 19% to 39% have been reported.12–14 These studies also demonstrated that S-1 had good compliance in patients with advanced colorectal cancer treated on an outpatient basis. Several regimens combining S-1 and CPT-11 were subsequently developed.15–19 Goto et al 15 conducted a phase II study consisting of 150 mg/m2 of CPT-11 given on day 1 with 40 mg/m2 of S-1 twice daily on days 1 to 14 of a 21-day cycle to assess efficacy and safety. They concluded that the combined treatment was a promising regimen, offering benefits in terms of safety and survival as compared with conventional regimens in patients with advanced colorectal cancer. Muro et al 20 reported a noninferiority of IRIS regimen consisting of 125 mg/m2 of CPT-11 given on days 1 and 15 with 40 mg/m2 of S-1 twice daily on days 1 to 14 of a 28-day cycle to the FOLFIRI regimen in a phase III study as second-line therapy.
Conventional cytotoxic chemotherapeutics affect the endothelium of the growing tumor vasculature in addition to affecting the proliferating cancer cells and various types of normal cells. 21 The antiangiogenic effects of chemotherapy would seem to be optimized by administering a comparatively low dose according to a more frequent (daily, several times a week, or weekly) or continuous schedule, with no extended interruptions, which is sometimes referred to as metronomic chemotherapy. 22 This would also have the advantage of being less acutely toxic, therefore, making more prolonged treatments hypothetically possible. Thus, peroral fuoropyrimidine on a daily schedule such as S-1 would be a reasonable metronomic chemotherapy. High rates of grade 3 or 4 toxicities generally can necessitate temporary suspension of the chemotherapy, especially when CPT-11 is given at a high dosage biweekly or triweekly schedule similar to Goto's regimen 15 and Muro's regimen. 20 This might not allow the metronomic advantage of daily peroral fuoropyrimidine to be realized in combination with CPT-11. We, therefore, postulate that a new combination therapy of low-dose and weekly CPT-11 with daily S-1 could realize the advantages of metronomic administration probably having an antiangiogenic effect in addition to an antiproliferation effect. Ogata et al conducted a phase I study to assess the recommended doses of weekly CPT-11 and S-1 combination therapy, 21 which recommended a CPT-11 dose of 60 mg/m2 on days 1, 8, and 15 with 40 mg/m2 of S-1 twice daily on days 3 to 7, days 10 to 14, and on days 17 to 21 of a 28-day cycle. We report the results of this phase II study to validate the antitumor efficacy and safety of weekly CPT-11 combined with daily S-1 as new combination schedule representing a metronomic advantage in addition to a cytotoxic effect.
Patients and Methods
Eligibility
This was a nonrandomized, open-label, multicenter phase II study. Eligible patients had histological findings of colorectal adenocarcinoma that was either unresectable, locally advanced, metastatic, or recurrent disease. They also had no prior chemotherapy, major surgery, or radiation therapy within 2 weeks of beginning treatment and measurable tumors with at least one lesion having dimensions > 10 mm in longest diameters. A life expectancy of 3 months and a performance status (PS) according to an Eastern Cooperative Group (ECOG) scale of 0 to 1 was mandated along with adequate bone marrow function (leukocytes 4000 per mm3, granulocytes 1500/mm3, platelets 100000 per mm3), adequate liver function (bilirubin 1.5 mg/dL), adequate renal function (creatinine 1.1 mg/dL), no serious or uncontrolled concurrent medical illness, and no other active malignancy. Postoperative adjuvant chemotherapy excluding regimens including CPT-11 or S-1 was allowed. Patients were required to be 20 years of age or greater and 75 years of age or less and not pregnant. All patients were informed of the investigational nature of this treatment and gave their fully informed written consent.
The study has been approved by the ethics committee of Kurume University and each institutional ethical committee.
Treatment Protocol
CPT-11 was administered by infusion intravenously over 90 minutes once weekly for three consecutive weeks followed by one week of rest in 4-week treatment cycles. S-1 was available as capsules containing 20 or 25 mg of tegafur. S-1 was given orally twice daily on days 3 to 7, 10 to 14, and 17 to 21. Patients were assigned one of the following doses to be taken within an hour after breakfast and supper on the basis of body surface area (BSA): 40 mg (BSA < 1.25 m2), 50 mg (1.25 m2 < BSA < 1.50 m2), or 60 mg (BSA ≥ 1.50 m2). Cycles were repeated every 4 weeks until disease progressed.
The CPT-11 administration was temporarily suspended for grade 2 or higher mucositis, any grade of diarrhea, other nonhematological toxicity grade 3 or higher, or for leucocytes < 3000/mm3, granulocytes < 1500/mm3, or platelets < 100,000/mm3. The S-1 administration was also temporarily suspended for grade 2 or higher diarrhea, grade 2 or higher mucositis, other nonhematological toxicity grade 3 or higher, or for leukocytes < 2000/mm3, granulocytes < 1000/mm3, or platelets < 75,000/mm3. The therapy was alternatively reinstituted using reduced dosages after all toxicity had recovered if leukocytes < 2000/mm3, granulocytes < 1000/mm3, platelets < 50000/mm3, or grade 3 or higher nonhematological toxicity (excluding nausea/vomiting and general fatigue) was noted during the cycle or if the treatment delay was longer than 14 days. The dosage of CPT-11 was reduced by 10 mg/m2 for subsequent courses, and the 60 mg, 50 mg, and 40 mg doses of S-1 were reduced in subsequent courses to 50 mg, 40 mg, and 25 mg twice daily, respectively. Once lowered, the doses of S-1 and irinotecan were not increased. All treatment was performed on an outpatient basis.
Evaluation
Within 2 weeks before initiating the chemotherapy, all patients were assessed by a physical examination, laboratory analyses, ECG, and computed tomography (CT) scans of the abdomen and chest to define the extent of disease. Complete blood cell counts with platelet and differential counts were recorded weekly during chemotherapy, and serum chemistries were repeated once or twice within every treatment cycle. Subjective symptoms, body weight, physical examination, performance status, and all adverse effects were recorded before each treatment course. Measurement of serum tumor marker carcinoembryonic antigen (CEA) level was performed at least once every 4 weeks.
Measurable lesions were reassessed every 8 weeks or 2 chemotherapy cycles using CT scan that allowed retrospective and independent evaluation. The response rate was assessed every 8 weeks using the RECIST criteria version 1.0. 24 All tumor measurements were reviewed and confirmed by an independent panel of radiologists. The overall survival (OS) and the progression-free survival (PFS) were calculated as the time from the first infusion until death or until disease progressed using the Kaplan-Meier product-limit method.
Adverse reactions were evaluated according to the National Cancer Institute Common Toxicity Criteria (NCI-CTC) version 3.0. Relative dose intensity was determined for up to six courses of treatment per patient.
Statistical Analysis
Response rates with 5-FU plus LV or with irinotecan as a single agent were approximately 20% in previous clinical trials in patients with advanced colorectal cancer. With a combination of irinotecan, 5-FU, and LV as first-line treatment for advanced colorectal cancer, the response rate was about 40%. We calculated the required sample size for this study on the basis of a target activity level of 40% and a minimum activity level of 20%, with alpha and beta error of 0.15. The required number of patients was estimated to be 41. A stopping rule was included in this study. All data were compiled and analyzed using Statistical Analysis Software (SAS) version 6.12, (SAS Institute, Cary, NC, USA). The exact binominal confidence interval was applied to estimate the response rates.
Results
Patient Characteristics
Between April 1, 2006 and October 31, 2007, we enrolled 46 patients with advanced colorectal carcinoma. One patient did not have any measurable tumor. In all, 45 patients met all eligibility requirements. The patients’ characteristics are shown in Table 1. All eligible patients received at least one course of treatment. The average age was 62 years, ranging from 38 to 75 years. Twenty-seven were male, and 18 were female. The PS was 0 in the majority of patients. Thirty-four patients had recurrent tumors. Among them, twenty-seven patients received prior adjuvant chemotherapy, and the most commonly affected site of metastasis was the liver. One half of patients had more than one organ affected by metastases. Two patients had primary site with metastatic lesions at study entry. The median follow-up time was 21 months. The eligible 45 patients had received a total of 255 treatment cycles (5.7 ± 2.7 courses; range, 1–14 courses).
Characteristics of the eligible patients.

Antitumor Efficacy
All eligible 45 patients had at least one measurable lesion. One patient achieved a complete response (CR), while 21 patients achieved partial responses (PR). Seven patients did not respond to chemotherapy and the disease progressed (PD); 16 patients showed a stable disease (SD) condition. The objective response rate was 48.9% with the 95% confidence interval (95% CI) being from 33.7% to 64.2%. The disease control rate was 84.4% with the 95% CI being from 70.5% to 93.5% (Table 2). At a median follow-up time of 21 months, the median progression-free survival (PFS) time was 8.1 months (range, 1–22 months; 95% CI, 6.2–9.0 months) (Fig. 1), and the median overall survival time (OS) was 20.9 months (range, 2–59 months; 95% CI, 15.5–27.3 months) (Fig. 2).
Anti-tumor efficacy.

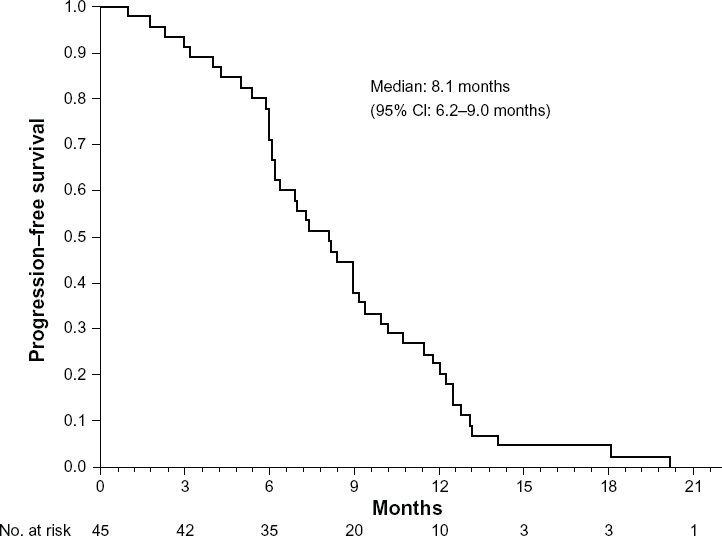
Progression-free survival of 45 patients with previously untreated colorectal cancer who received new combination chemotherapy of S-1 and irinotecan.

Overall survival of 45 patients with previously untreated colorectal cancer who received new combination chemotherapy of S-1 and irinotecan.
Adverse Effects
A total of 260 treatment cycles were administered to the 45 eligible patients and 1 ineligible patient to define safety profiles. Toxicity is summarized according to the worst grade per patient in Table 3. There were no treatment-related deaths. The most common type of hematological toxicity was neutropenia (leukopenia); however, the incidence of grade 3 or 4 neutropenia was very low (8.7%). The patient with the grade 3 elevation of bilirubin was confirmed to have severe multiple liver metastasis at study entry. The most common types of nonhematological toxicity were anorexia and diarrhea, which were usually mild. Cumulatively, myelosuppression and gastrointestinal toxicity were the most common adverse events but were generally mild. The incidence of grade 3 or 4 toxicity was less than 10% altogether. Treatment was discontinued because of toxicity in 6 of the 46 patients (13%). The reasons for discontinuing treatment were as follows: (1) treatment delay longer than 14 days due to grade 2 neutropenia, (2) treatment delay longer than 14 days due to grade 2 diarrhea, (3) grade 3 confusion due to trouble in stoma care associated with grade 3 diarrhea, (4) patient's refusal to continue treatment because of grade 3 anorexia, (5) patient's refusal to continue treatment because of grade 2 diarrhea, and (6) patient's refusal to continue treatment because of prolonged mild fatigue and nausea.
Adverse events (n = 46).

Relative Dose Intensity
The administration of CPT-11 was skipped on a few occasions mainly because of grade 2 or 3 neutropenia, diarrhea, or a patient's request due to nausea/vomiting, anorexia, or general fatigue. Table 4 lists the amount of CPT-11 and S-1 chemotherapy actually administered, relative to the normal full dosage, in each treatment cycle up to 6th cycle (a total of 219 cycles). The mean relative dose intensity of CPT-11 was 90% with a range from 86% to 94% in each treatment cycle. The mean relative dose intensity of S-1 was 92% with a range from 87% to 97% in each treatment cycle. All patients received the initial doses of irinotecan and S-1 on day 1 and day 3 of the first treatment cycle on an outpatient basis. Three patients were subjected to dosage reduction in CPT-11 and S-1 according to the dosage-reduction criteria. One patient required dosage reduction in CPT-11 because of grade 2 fatigue, and another patient required dosage reduction in S-1 because of grade 1 diarrhea and fatigue.
Administered dosage of CPT-11 and S-1 as a function of normal full dosage.

Poststudy Therapy
Among the 45 patients, 30 patients received post-study chemotherapy, 5 patients received surgery, 1 patient received radiotherapy for intrapelvic reccurent tumor, and 9 patients received best supportive care only. Oxaliplatin-containing regimens were administered to 28 patients (93%). Second-line chemotherapy was administered to 9 patients, third-line chemotherapy to 16 patients, and fourth-line chemotherapy to 5 patients. Bevacizumab was administered to 9 patients, and cetuximab was administered to 2 patients. Surgery for 2 patients with unresectable disease was converted to resection after second-line chemotherapy.
Discussion
Metronomic chemotherapy has been summarized by Kerbel et al 22 as showing that (1) conventional cytotoxic anticancer drugs have antiangiogenic effects that could contribute to their efficacy, and (2) the antiangiogenic effects of chemotherapy seemed to be optimized by administering such drugs metronomically, that is, in small dosages on a frequent schedule (daily, several times a week, or weekly) in an uninterrupted manner. The present phase II study assessed the efficacy and safety of a new S-1 and CPT-11 combination therapy in patients with previously untreated metastatic or recurrent colorectal cancer. Our results showed that the new combination schedule was effective, with a response rate of 48.9%, median PFS of 8.1 months, and median OS of 20.9 months, whereas a total dosage of CPT-11 was relatively low. In previous phase III studies of CPT-11 plus intravenous 5-FU and LV, response rates ranged from 31% to 62%.4,25–28 Median time to progression (TTP) or PFS was 6.7 to 8.7 months, and median OS was 14 to 21.5 months. Although there are limitations in comparing the results of different studies, the response rate, PFS, and OS in our study were similar to those reported in previous studies of CPT-11 plus intravenous 5-FU and LV. Moreover, our results were not inferior to those of the regimens, combination therapies using S-1 and conventional MTD administration of CPT-11, with response rates of 52.5% to 62.5% and with a median PFS of 7.7 to 8.6 months as a first-line therapy (Fig. 3).14–18 In these regimens, 80 mg/m2 of S-1 was administered at 3.5 days to 4.7 days per week, and CPT-11 was administered at dosage of 32 mg/m2 to 50 mg/m2 per week and 0.33 times to 0.5 times per week. A key characteristic of our regimen was the frequency in CPT-11 administered 0.75 times per week.

Treatment protocols of various combination chemotherapies of S-1 and irinotecan in advanced or recurrent colorectal cancer.
In our preclinical study of metronomic chemotherapy using CPT-11 for colon cancer implanted in nude mice, the metronomic chemotherapy was more effective than the conventional MTD therapy via antiangiogenic effect associated with a consistent inhibition of circulating endothelial progenitor cells (CEPs). 29 Both frequent administration of CPT-11 and S-1 would be reasonable to enhance significant antiangiogenic activity compared with oral S-1 regimens combined with MTD administration of CPT-11, as reported by Munoz et al 30 using combination oral UFT-cyclophosphamide metronomic chemotherapy against breast cancer in mice. Since our concept of this new combination schedule consisted of inhibition of tumor angiogenesis and cytotoxic activity, optimal biological doses of cytotoxic agents should be determined using both toxicity and surrogate marker for antiangiogenesis such as CEPs. 31 Moreover, antitumor efficacy of the new schedule may be significantly increased when administered in combination with bevacizumab, an antiangiogenic biologic that is used worldwide for colorectal cancer. 32
Another advantage of our regimen is the interval of administration of CPT-11 and S-1. The in vitro studies have shown that CPT-11 downregulates thymidylate synthase expression in tumor cells leading to synergy between CPT-11 and 5-FU that was maximal when CPT-11 was given 24 hours prior to 5-FU.33,34 Therefore, the weekly administration of CPT-11 followed by S-1 with a 2-day interval in our regimen seems to be reasonable in terms of the cytotoxic activity and of gastrointestinal toxicity such as anorexia, nausea, and vomiting. Yoshioka's regimen using the 2-day interval between CPT-11 and S-1 administrations also resulted in a low toxicity. 29
Toxicity was generally mild and manageable on an outpatient basis. The most common hematological toxicity was neutropenia. However, the incidence of grade 3 or 4 neutropenia was low. The most common types of nonhematological toxicity were diarrhea and anorexia, which were not severe. The incidences of grade 3 or 4 diarrhea and anorexia were also low. Of interest, however, patients with anorexia had many other related adverse effects, such as diarrhea, dehydration, fatigue, and neutropenia (data not shown). In patients who had moderate anorexia or diarrhea, treatment with S-1 was temporarily discontinued. Consequently, grade 2 of either neutropenia or leucopenia was the most common reason for skipping the day 15 dose of CPT-11 in the treatment cycle. However, it was rare that the start of the next treatment cycle was delayed. Neutropenia, diarrhea, nausea, and vomiting frequently occurred in previous studies of combined treatment with CPT-11 plus infusional 5-FU/LV4,25–28 or with metronomic administration of S-1 and MTD administration of CPT-11.15–19 Our results suggested that both the incidences and intensities of these toxic reactions with S-1 plus weekly CPT-11 were lower than those with a combination of CPT-11 plus infusional 5-FU/LV or with metronomic administration of S-1 and MTD administration of CPT-11.
The low toxicity in the present study has resulted in higher relative dose intensity. The mean relative dose intensity of both S-1 and CPT-11 exceeded 90% up to 6th cycle. The relative dose intensity of S-1 and CPT-11 in our study was higher than that of combination therapy with metronomic administration of S-1 and MTD administration of CPT-11. 15 In Tsunoda's regimen,16,35 S-1 was administered twice daily for 3 weeks in combination with MTD administration of CPT-11 on days 1 and 15 of a 5-week cycle. The recommended dose was 80 mg/m2 of CPT-11. The dose intensity of CPT-11 in a 5-week schedule was very similar to that with Goto's regimen. 15 These findings suggest that the use of higher doses of CPT-11 would probably require a lower dose of S-1 or temporary discontinuation of S-1 to control toxicity, especially neutropenia, diarrhea, or prolonged fatigue, within acceptable levels.
Capecitabine is a widely used oral fluoropyrimidine derivative. Studies of a combination of capecitabine plus CPT-11 have shown significant efficacy, response rates ranging from 47% to 61%, and a median PFS or TTP of 6.1 to 8.3 months in patients with colorectal cancer.36,37 However, the incidence of grade 3 or 4 diarrhea with capecitabine plus CPT-11 was greater than 20%, clearly higher than that with our study and other regimens with S-1 and CPT-11. Both CPT-11 and capecitabine are metabolized by carboxylesterases in the liver to an active metabolite, 7-ethyl-10-hydroxy-camptothecin (SN-38), and to an intermediate metabolite, 5′-deoxy-5-fuoropyrimidine, respectively. The complex metabolism of both capecitabine and CPT-11 can thus theoretically lead to pharmacokinetic drug-drug interactions. 38 In contrast, a previous phase I trial using S-1 and CPT-11 showed no change in the plasma concentrations of 5-FU, FBAL, or SN-38 as compared with the concentrations after administration of S-1 or CPT-11 alone. 39 When CPT-11 is combined with S-1, it may, therefore, be safer and more convenient than a combination of capecitabine and CPT-11.
Conclusion
New combination chemotherapy using daily S-1 and low-dose weekly CPT-11 appeared to be an effective, well-tolerated, and convenient regimen in patients with advanced colorectal cancer. Our findings suggest that this new combination chemotherapy is a promising regimen, offering benefits in terms of safety and survival as compared with conventional regimens. Future studies must objectively confirm that the new S-1 and CPT-11 combination therapy can replace the standard FOLFIRI without negatively affecting efficacy or safety.
Funding
This work was supported by a Grant-in-Aid for Scientific Research (C) (No. 20591597) from the Ministry of Education, Culture, Sports, Science and Technology, of Japan.
Author Contributions
The principal investigator: KS. Responsible for study concept and design: YO. Provided patients: YO, TT, YA, NI, YT, KM, MI, SS, and AK. Collected and analyzed the data: YO, YA, and NI. Interpreted the data: YO, YA, and KS. Wrote the manuscript: YO. All authors reviewed and approved the final manuscript.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
This phase II study was conducted to validate the antitumor efficacy and safety of a new combination schedule of weekly low-dose irinotecan and daily S-1. The new combination schedule is an effective, less toxic, and convenient regimen in patients with advanced colorectal cancer.
Footnotes
Acknowledgements
We are indebted to the physicians and all other comedical staff who contributed to this study.