
Abstract
Juxtacortical chondrosarcoma is a rare primary malignant cartilaginous tumor accounting for 0.2% of all bone tumors. Wide surgical resection is the treatment of choice for juxtacortical chondrosarcomas. Accurate preoperative diagnosis is important in ensuring appropriate management, staging, and treatment of the patient. A combination of radiographs, three-dimensional imaging with computerized tomography (CT) scan and magnetic resonance imaging (MRI) can typically allow accurate diagnosis of juxtacortical chondrosarcomas. Bone scan and chest x-ray or CT chest scans are indicated for appropriate staging of the patient. Pet scan, ultrasound, bone scan, etc. are not typically needed for the diagnosis. Certainly, pulmonary imaging and bone scan are required for staging and could be commented upon.
Introduction
This report presents a rare case of juxtacortical chondrosarcoma arising from the diaphysis of the left clavicle. Also discussed is the strategy for an accurate and safe preoperative diagnosis.
All types of tumors that have been described to occur in the clavicle contribute to less than 0.5% of all skeletal tumors. Clavicular primary chondrosarcoma is extremely rare and to our knowledge, there is only one detailed report discussing its radiologic and clinicopathological findings. 1
The patient was a 54-year-old man who presented with a soft tissue tumor over the left clavicle and in the left side of his neck. Radiography and computerized tomography (CT) scan demonstrated cortical thickening and periosteal reaction of the diaphysis of the left clavicle without any osteolytic lesion. Magnetic resonance imaging (MRI) showed a mass with heterogeneous isosignal intensity in T1-WI and high-signal intensity in T2-WI. Imaging findings were more consistent with a juxtacortical chondrosarcoma rather than any other periosteal bone tumor.
Histological findings of the surgical biopsy specimens were in accordance with the clinical and radiologic preoperative diagnosis of a juxtacortical chondrosarcoma.
Case Report
A 54-year-old man presented with a 5 year history of a swelling mass in the left side of the neck and above the clavicle. He visited the E.R. in our hospital claiming severe pain in the neck. He also reported that the swelling appeared to be gradually increasing in size over the last several months (Figs. 1 and 2). There was no history of trauma hereditary disease or major illness.

54-year old male with soft-tissue tumor in left supraclavicular fossa.

54-year old male with soft-tissue tumor in left supraclavicular fossa.
Clinical examination revealed tenderness of a hard mass measuring approximately 11 × 10 cm in size located in the left side of the neck and the left supraclavicular fossa. The tumor caused poor mobility, while movements of the left shoulder and the neck induced pain in his neck and around the shaft of his left clavicle.
Radiographs demonstrated a soft tissue mass overlying the left clavicle with matrix formation consistent with chondroid calcifications; neither cortical changes nor osteolytic lesions of the clavicle were detected (Fig. 3).

54-year old male with soft-tissue tumor in left supraclavicular fossa.
Chest CT examination revealed a large, well-defined, ovoid soft tissue mass arising from the distal part of the diaphysis of the left clavicle, extending up to the left sternocleidomastoid muscle beneath the platysma muscle.
The matrix of the mass revealed coarse peripheral and multiple central spotty calcifications. There was extrinsic thickening and erosion of the upper cortex of the clavicle with no accompanying osteolysis or expansion of the clavicular cortex (Fig. 4). The non-mineralized parts of the mass revealed low attenuation compared to the muscles.

54-year old male with soft-tissue tumor in left supraclavicular fossa; (
Chest CT scan of the lungs was negative for any metastases.
MR images confirmed the presence of an ovoid, well-defined, soft-tissue mass in broad and direct contact with the diaphysis of the left clavicle with no associated bone marrow edema. The mass exhibited heterogeneous isosignal intensity on T1-WI sequences, heterogeneous high signal intensity on T2-WI sequences (Fig. 5), and heterogeneous vivid enhancement after the administration of contrast medium (Figs. 6 and 7). Centrally, the mass revealed ill-defined areas of high signal intensity mainly on T2-WI and less on T1-WI consistent with areas of myxoid degeneration or hemorrhage (Fig. 5).
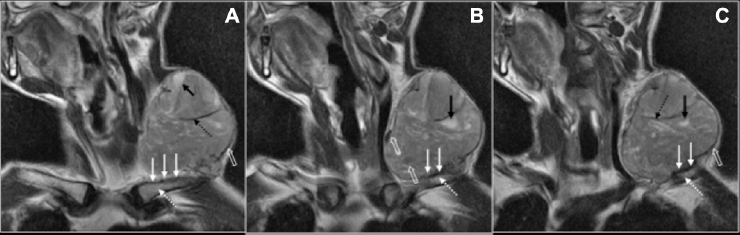
54-year old male with soft-tissue tumor in left supraclavicular fossa; (

54-year old male with soft-tissue tumor in left supraclavicular fossa; (

54-year old male with soft-tissue tumor in left supraclavicular fossa; Oblique coronal spin-echo, fat saturated T1 weighted MRI post-gadolinium enhanced image (time repetition: 520, time echo: 11.9, echo train length: 6).
Peripheral and central linear areas of low T1 and T2 signal intensity were consistent with calcifications (Fig. 5).
Technetium-99m-methylene-diphosphonate (MDP) demonstrated strong accumulation of the radiopharmaceutical agent only in the left clavicle, as well as soft-tissue calcifications (Fig. 8).

54-year old male with soft-tissue tumor in left supraclavicular fossa.
Imaging findings were more consistent with juxtacortical chondrosarcoma rather than periosteal osteosarcoma or chondroma.
A surgical biopsy was performed in order to establish diagnosis preoperatively.
Pathological Findings on Open Incisional Biopsy Specimens
Dense storiform arrangement of small ovoid shaped cells with atypical nuclei in a myxoid stroma with focally cartilaginous differentiation was noted. Some scattered calcifications were found in the biopsy specimen. Mitotic figures were not observed.
Immunohistochemically positive results were obtained for vimentin whereas the results were negative for S-100 protein, pan-cytokeratin, CD-31, CD-34, CD-56, and synaptophysin.
Surgery
Patient was referred to the Department of Othopaedic Surgery for surgical treatment. A very wide segmental en bloc resection of the left clavicle was performed and a reconstruction plate was inserted and fixed with screws.
Histological Features of the Tumor
The histological features of the tumor were observed. Specifically, (a) the periphery of the tumor showed a predominantly myxoid pattern; (b) the center of the tumor showed cartilaginous differentiation containing scattered matrix calcifications, without tumor osteoid; and (c) in the myxoid area, the tumor cells were ovoid shaped with moderate nuclear atypia. The frequency of mitoses was low (1 mitotic figure/10HPF, 400×). Tumor necrosis was not present.
Immunohistochemical findings were the same as in the initial biopsy specimens.
Therefore, the diagnosis was a low-grade juxtacortical chondrosarcoma and the surgical resection margins were negative.
On the advice of the oncologists no further treatment was undertaken.
Follow-up
Chest x-ray was performed 4 weeks after surgery to check the reconstruction plate, and chest CT scans were scheduled and performed at 6 and 12 months postoperatively. During these clinical visits at 6- and 12-month's time after surgery, the patient was still free of disease without signs of local recurrence and distant metastases, and the patient was functioning adequately. There was no 2-year follow-up visit, since the patient was abroad, but there was a consultation by phone. The patient reported that he was well and that CT scans were normal without any signs of local or disease recurrence.
Discussion
Clavicular primary tumors and tumor-like lesions are uncommon and they only contribute to less than 0.5% of all primary bone tumors. 2 Additionally, primary chondrosarcoma is reported to be the third most common primary malignant bone tumor, constituting 20%–27% of all primary malignant osseous neoplasms. 3 Primary chondrosarcomas arise de novo, while chondrosarcomas developing on pre-existing enchondromas or osteochondromas are referred to as secondary chondrosarcomas. 3
Chondrosarcomas can be categorized according to their location in bone into central, peripheral, and juxtacortical. The majority (>85%) are primary chondrosarcomas located centrally within the medullar cavity, while the minority (<15%) are secondary chondrosarcomas developing from the surface of the bone as a result of malignant transformation of a pre-existing osteochondroma.
Chondrosarcomas occurring at the surface of the bone (<1%) are referred to as periosteal, parosteal, or juxtacortical with the descriptive term emphasizing the close relationship of the tumor to the adjacent bony cortex. 4
Furthermore, the WHO classification accepts juxtacortical chondrosarcoma as a distinct entity which should be distinguished from conventional peripheral chondrosarcoma. 4
Therefore, juxtacortical chondrosarcoma is reported as a rare malignant cartilaginous tumor accounting for less than 2% of all chondrosarcomas and 0.2% of all bone tumors with an excellent prognosis after adequate local surgery alone.3,4
Histological grading (grades 1–3) for chondrosarcomas is related to clinical behavior and prognosis. Grade 1 chondrosarcomas are lowly cellular, with chondroid-matrix and absent mitoses. In Grade 2, chondrosarcomas mitoses are found (inset). While in Grade 3 chondrosarcomas, high cellularity with mucomyxoid matrix changes, cytonuclear atypia, and mitoses are seen. Grade 1 chondrosarcomas rarely metastasize, while Grade 3 chondrosarcomas develop metastases in 70% of patients. 4
Favorite locations for the development of these chondrosarcomas are posterior distal femoral and humeral diaphysis or metaphysic, followed by the innominate bone. Most of these tumors primarily occur in the deep soft tissues of proximal extremities and limb girdles, and only occasionally do they first involve subcutaneous tissue. 5
A review of the published data revealed that there are two detailed case reports and two case series of clavicular chondrosarcoma, but only the case reported by Nakazora et al 1 refers to a primary myxoid extraskeletal chondrosarcoma arising from the clavicle.1,2,6,7 Deik et al 8 also reported a case of extraskeletal myxoid chondrosarcoma arising supraclavicularly, causing an interesting clinical presentation.
To the best of our knowledge, this is the first detailed case report of a juxtacortical chondrosarcoma arising specifically from the clavicular periosteum. We presented a detailed report of the radiologic and clinicopathological features of this rare case, as well as the diagnostic difficulties encountered with imaging examinations and sometimes with histological findings in biopsy specimens.
Surgery is the only treatment for juxtacortical chondrosarcoma and includes excision of the primary tumor along with a wide surgical margin with a very good prognosis.4,9 However, in cases that a wide margin cannot be obtained, the rate of recurrence is very high with poor response to chemotherapy and radiotherapy. 1
Additionally, segmental, wide, en bloc excision is the preferred surgical treatment in all grades of peripheral chondrosarcomas.1,4,9
In central chondrosarcoma, extensive intralesional curettage followed by local adjuvant treatment and filling the cavity with bone graft has often satisfactory local control and clinical result when the tumor is low-grade and confined to the bone.4,9 Nevertheless, in large chondrosarcoma with a huge soft tissue mass, claviculectomy is the key treatment.
Therefore, an accurate preoperative diagnosis is important in ensuring appropriate management, staging and treatment of the patient. Typically, size and location of primary tumor, grade, resection margins, local recurrence or metastatic disease are the most important factors affecting survival.
There are numerous types of primary chondrosarcomas with a pathological appearance that varies with the specific lesion type. 3 Imaging examinations often reflect this pathological appearance and show distinctive features in the various subtypes.
On radiography, juxtacortical chondrosarcoma appears as a well-defined periosteal soft tissue mass that may contain popcorn, spotty, peripheral or ring-and-arc calcifications (as in this case), characteristic of cartilaginous tumors.5,9
CT is the method of choice to depict matrix mineralization and calcifications characteristic of cartilaginous tumors. Due to its superior contrast resolution, MRI is the optimal imaging technique for detecting intramedullary and soft tissue extensions.
On MR images the tumor matrix has low to intermediate signal intensity on T1-WI, and very bright signal intensity on T2-WI associated with hypointense septa. Low signal foci can be seen on both T1 and T2-WI, and hemorrhagic or myxoid changes may sometimes be recognized on T1-weighted MR images as areas of high signal intensity 1 , as in our case.
Published data supports the idea that current imaging techniques provide numerous methods, such as MR imaging, CT, MR angiography, ultrasonography, and PET to diagnose and stage suspected soft tissue sarcomas. 13
Although plain radiography, CT, and MR images remain the primary diagnostic modalities for staging bone and soft tissue sarcomas, nuclear medicine investigations including gamma camera scintigraphy and positron emission tomography (PET) are being used to provide complementary information in specific clinical situations. These include guided-biopsy in anatomically complex masses, assessment of therapeutic response, or evaluation of residual disease after treatment.
Bone scan with Tc-99m (technetium) diphosphonate is the standard scintigraphic modality for the evaluation of local tumor conditions and bone involvement. T1-201 (thallium), Tc-99m-sestamibi, Tc-99m-tetrofosmin and metabolic positron (PET) radiopharmaceuticals are characterized as tumor seeking agents, and many times have been found to be useful in the initial diagnosis, grading, and post-therapy evaluation of primary bone tumors. Nevertheless, the importance of bone scintigraphy for the evaluation of bone tumors has decreased over the last several years, with the exception of osteosarcomas, where this method is still valuable; however, the accuracy of a bone scan can be increased by using SPECT and SPECT/CT.7,8
Radiologic differential diagnosis mainly consists of juxtacortical chondroma, parosteal osteosarcoma and periosteal osteosarcoma. Juxtacortical chondromas are usually smaller than 2 cm, with chondrosarcomas ranging from 3 to 14 cm. Periosteal osteosarcoma radiologically exhibits periosteal reaction perpendicular to the cortex on radiographs, and favors a more diaphyseal location. Parosteal osteosarcoma may be the most challenging differential diagnosis from a radiological perspective; however, it usually has a stalk of attachment to the cortex and extensive osteoid. 1
On account of the above radiologic features noted in our case, CT and MR images strongly suggested the diagnosis of juxtacortical chondrosarcoma.
From the pathological view, juxtacortical chondrosarcoma is characterized by lobular growth of oval or spindle-shaped cells, arranged in cords or strands in a prominent myxoid stroma.1,12
Our case showed a dense storiform arrangement of ovoid-shaped cells poor in eosinophilic cytoplasm and rich in myxoid stroma, which was positive only for vimentin and negative for S-100 protein.
This case report presents a rare location of a primary juxtacortical chondrosarcoma and highlights that the combination of MR and CT images can suggest, with relative safety, the preoperative diagnosis of various types of chondrosarcomas.
In conclusion, imaging findings along with pathological assessment in biopsy specimens offer a valuable preoperative evaluation in all types of chondrosarcomas, which is important in ensuring appropriate clinical management of these patients.
Ethics
Patient consent has been obtained. Written and signed consent from the patient is at the disposal of the editors.
Author Contributions
EIE has participated in the design of the study and in drafting the manuscript; AO participated in the inter pretation of data and helped to draft the manuscript; EP participated in the acquisition and analysis of data; GD revised the manuscript for intellectual content; AK participated in coordination, and revised the manuscript critically for intellectual content; NL participated in coordination, revised the manuscript critically for important intellectual content, and has given final approval of this version to be published. All authors have read and approved the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.