
Abstract
Introduction
Clavicular fractures, particularly comminuted fractures, are common injuries that can affect shoulder function and upper limb mobility. The management of these fractures, especially using surgical approaches and fixation methods, remains a key area of clinical focus. Preserving the periosteum during surgery may improve fracture healing and reduce complications. This study explored the clinical efficacy of a periosteum-preserving surgical technique combined with a Nice knot–assisted locking plate for treating comminuted clavicular fractures.
Methods
A total of 85 patients with comminuted clavicular fractures were included in this retrospective study. According to the Allman classification, 56 (65.9%) cases were type IC, 19 (22.4%) were type II, 9 (10.9%) were type III, and 1 (1.1%) involved comminuted fractures across the entire clavicle. All patients underwent surgical treatment using a periosteum-preserving approach combined with a Nice knot–assisted locking plate. Fracture healing time, upper limb function (measured via Constant–Murley score and disabilities of the arm, shoulder, and hand questionnaire), and postoperative complications were assessed 6 and 12 months postoperatively.
Results
The median healing time was 13 weeks, with no cases of nonunion reported. At 6 months postoperatively, the Constant–Murley and disabilities of the arm, shoulder, and hand scores were excellent. Although a statistically significant difference (P < 0.05) was observed in these scores between 6 and 12 months, all patients reported satisfactory recovery of shoulder function and upper limb mobility. No significant differences (P > 0.05) in fracture healing time or upper limb function recovery were observed across different types of clavicular fractures. Six (7.1%) patients experienced temporary numbness in the subclavian region, which gradually resolved by the final follow-up.
Conclusion
The periosteum-preserving approach with Nice knot–assisted locking plate fixation proved to be an effective and reliable treatment for comminuted clavicular fractures. The technique was associated with favorable healing times, excellent functional outcomes, and low complication rates. Preservation of the periosteum and soft tissue during surgery may considerably reduce intraoperative trauma and improve postsurgical recovery. Further studies with larger sample sizes and longer follow-up periods are needed to confirm the long-term benefits of this approach.
Keywords
Background
Clavicle fractures are common injuries, accounting for approximately 5%–10% of all fractures. 1 They primarily occur in young men and elderly women,1,2 often resulting from direct trauma to the shoulder or indirect forces, with traffic accidents and accidental falls being the most frequent causes. 1 Treatment varies depending on the fracture type. Simple clavicle fractures often respond well to nonsurgical methods, such as figure-of-eight bandages or limb suspension, effectively relieving symptoms and promoting healing. 3 However, conservative approaches are less effective for comminuted displaced fractures, occasionally requiring secondary surgery to address nonunion.3,4 In recent years, the frequency of surgical treatment for clavicle fractures has increased. 5 The goal of surgery is to restore shoulder joint function through early mobilization and prevent malunion or nonunion. 6 Achievement of these outcomes relies on proper fracture fixation.
For closed clavicular fractures, efforts have been made to reduce soft tissue damage by exploring surgical techniques and internal fixation methods. Elastic intramedullary nailing offers advantages such as minimal incisions, limited periosteal damage, and enhanced fracture healing. 7 Minimally invasive plate osteosynthesis, a technique developed to achieve minimally invasive plating, has gained widespread popularity.8,9 However, comminuted clavicle fractures pose substantial treatment challenges due to the irregularity and high number of fragments, complicating fracture reduction. Minimally invasive internal fixation techniques are ineffective in repositioning bone fragments, whereas open surgery may lead to nonunion due to excessive soft tissue and periosteal damage during the procedure.
A doubled-suture Nice knot, as described by Boileau et al., 10 offers distinct advantages in stabilizing hard materials such as bone fragments, and its efficacy in clavicle fracture surgery has been validated. In this study, we employed a semi-open surgical approach for comminuted clavicle fractures, avoiding periosteal incision or disruption. Bone fragments were reduced and fixed using doubled-suture Nice knots, whereas locking plate solely stabilized the fracture ends and restored the clavicle length. This technique achieved favorable clinical outcomes.
Patients and methods
This retrospective study, approved by the ethics committee of the Wuhan Fourth Hospital, was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2013. Written informed consent was obtained from each enrolled patient. Detailed information of all patients was removed. We assessed inpatient clavicle fractures treated at our hospital between September 2019 and April 2023. The inclusion criteria were as follows: (a) comminuted clavicle fractures with three or more fragments (excluding fractures involving the acromioclavicular joint); (b) patients aged 18–70 years; (c) fresh closed fractures treated surgically within 2 weeks of injury; (d) follow-up duration >12 months; and (e) normal shoulder joint function before injury and no other associated injuries. Patients’ demographic and clinical data were collected and analyzed. Clavicle fractures were categorized according to the Allman classification, 11 and all patients were grouped based on the fracture type.
Surgical process
All surgeries were performed by the same surgical team under general anesthesia. Patients were placed in the beach-chair position with a soft pad under the scapular area to elevate the back for fracture reduction. 8 Preoperative fluoroscopy was used to locate fracture fragments, and their positions were marked on the skin to guide intraoperative placement of Nice knots.
After standard disinfection and draping, a longitudinal incision (approximately 8 cm) centered on the fracture site along the clavicle axis was made. Subcutaneous tissue was carefully dissected to protect supraclavicular nerve branches, with blunt dissection performed between the platysma and periosteum. The periosteum was preserved intact by avoiding incisions with scalpels or electrocautery. At the preoperative skin markings, a large curved needle with 3-0 silk sutures was used as a guide, passing around the proximal and distal fracture ends and bone fragments. Silk sutures were used to pull Orthocord sutures (Depuy Synthes, West Chester, PA, USA) into place, forming double-stranded loops, which were set aside for later use. The surgeon used large curved clamps to grasp the fracture ends for reduction, focusing on restoring clavicle length and rotation. The assistant temporarily stabilized the fracture ends with one or two 1.2-mm Kirschner wires. Subsequently, the double-stranded Orthocord sutures were tied into Nice knots to secure the fracture ends and free fragments, without emphasizing precise anatomical reduction. A locking plate of appropriate length was contoured to fit the clavicular shaft and centrally placed on the superior surface. Locking screws of suitable length were inserted as needed based on the fracture pattern, with at least three screws placed on each side of the fracture. Representative cases are shown in Figure 1 and Figure 2.

Case: A 32-year-old woman with a comminuted right clavicular fracture. (a) Preoperative localization to identify fracture ends and the Nice knot—binding site. (b) Intraoperative exposure between the sternocleidomastoid and periosteum, with protection of the supraclavicular nerve. (c) Temporary fixation with Kirschner wires outside the periosteum, followed by fixation of bone fragments with a Nice knot. (d) Intraoperative fluoroscopy confirming fracture reduction and visible bone fragments. (e) Internal fixation with a locking plate and (f) immediate postoperative X-ray.
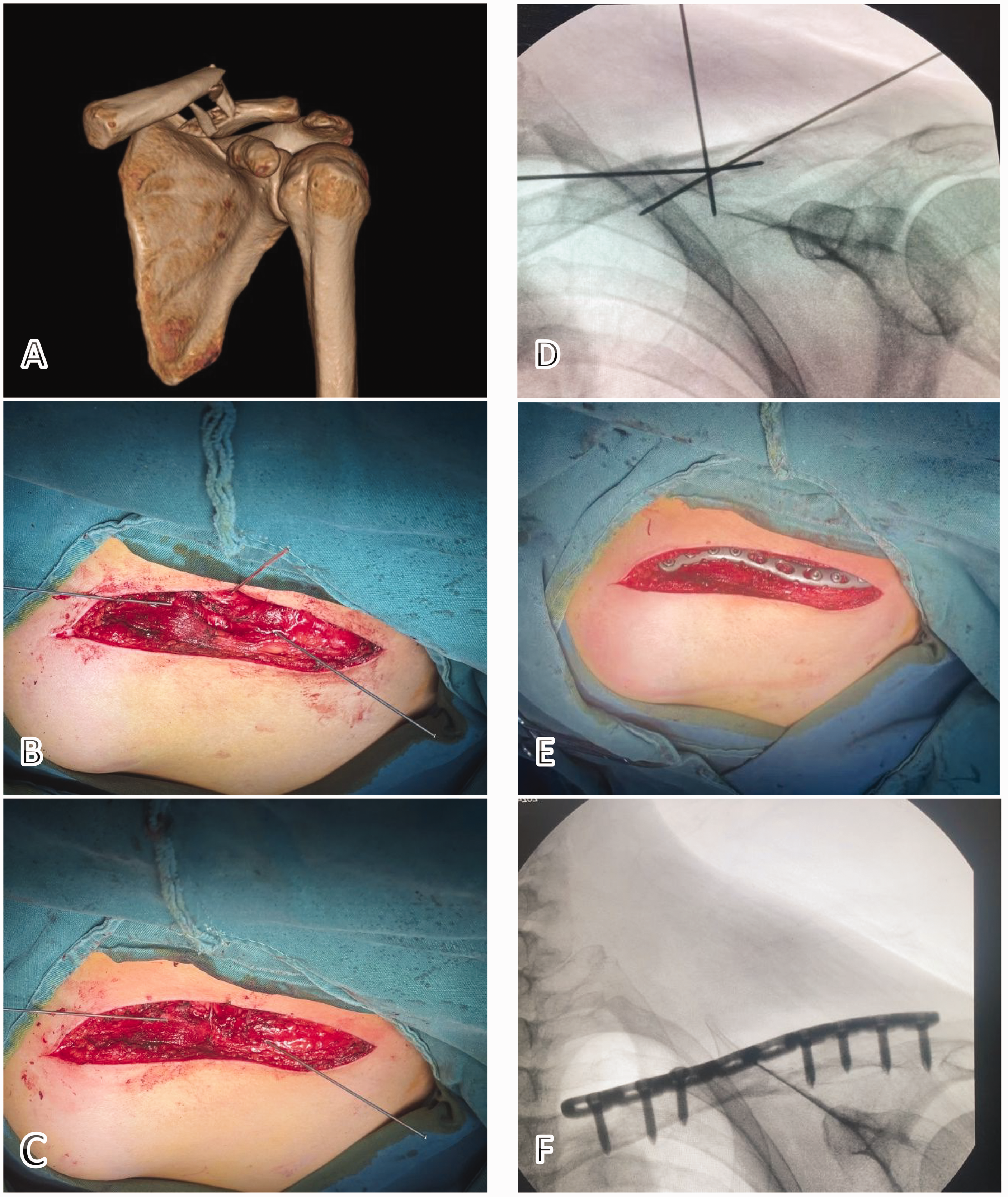
Case: A 50-year-old woman with comminuted fracture of the left clavicle. (a) Preoperative CT-3D reconstruction image of the clavicle. (b) Temporary fixation with Kirschner wires outside the periosteum. (c) Bone block fixation using Nice banding. (d) Intraoperative fluoroscopy showing reduction of the fracture bones. (e) Internal fixation with a locking plate and (f) immediate postoperative X-ray. CT: computed tomography; 3D: three dimensional.
Postoperative management
Prophylactic antibiotics were not required. A clavicle anteroposterior radiograph was obtained on postoperative day 2 to assess fracture reduction. The affected limb was supported with a sling for at least 4 weeks. Passive shoulder mobilization began on postoperative day 3, with prohibition of active movements. Active shoulder exercises started after 4 weeks, whereas weight-bearing activities were restricted.
Assessment indicators
Medical and surgical records of all patients were reviewed, and they were grouped based on the fracture type. During follow-up, operative time, intraoperative blood loss, fracture healing time, upper limb function, and complications (e.g. wound infection, plate breakage, delayed union, nonunion, refracture, supraclavicular nerve injury, and skin irritation) were recorded. Fracture healing was evaluated using imaging, with radiographic union defined as visible callus bridging or the absence of a fracture line on X-ray. Follow-up radiographs were performed every 2 weeks and continued until union was confirmed. Upper limb function was assessed using the Constant–Murley score (CMS) and disabilities of the arm, shoulder, and hand (DASH) questionnaire 6 and 12 months postoperatively.
Statistical analysis
Statistical analysis was performed using SPSS 29.0 (SPSS Inc., Chicago, IL, USA). The Shapiro–Wilk test was used to assess the normality of the data. Analysis indicated that all variables did not follow a normal distribution; thus, the Mann–Whitney U test was used for group comparisons and the Kruskal–Wallis H test for pairwise group comparisons. Owing to the retrospective observational nature of this study, all values were considered explorative and descriptive.
Results
This study was reported according to the relevant EQUATOR checklist. 12 This study included 85 patients with unilateral comminuted clavicle fractures, comprising 55 (64.7%) men and 30 (35.3%) women, with a median age of 46.0 (interquartile range (IQR): 32.5–55.5) years. According to the Allman classification, 56 (65.9%) cases were type IC, 19 (22.4%) were type II, 9 (10.9%) were type III, and 1 (1.1%) involved comminuted fractures across the entire clavicle. The operative time was 65.0 (IQR: 60.0–76.0) min, and intraoperative blood loss was 29.0 (IQR: 25.0–32.0) mL.
Radiographic and functional outcomes and complications
The postoperative follow-up period was 15 (IQR: 13–17) months. Immediate postoperative X-ray showed satisfactory fracture reduction, with no revision surgeries performed during hospitalization. Based on the study’s criteria for fracture healing, the median healing time was 13 (IQR: 12–14) weeks. One patient experienced locking plate breakage approximately 1 month postoperatively, and 6 patients reported subclavicular skin numbness. No other complications, such as wound infection, malunion, delayed union, nonunion, or implant irritation, were observed. For the patient with locking plate breakage, a sling was used to immobilize the shoulder, and weight-bearing activities were restricted; the fracture line resolved on X-ray by 3 months postoperatively. At 6 months postoperatively, the CMS was 92.0 (IQR: 90.0–94.0) and the DASH score was 2.0 (IQR: 0.8–3.0). At 12 months postoperatively, the CMS improved to 95.0 (IQR: 95.0–97.0) and the DASH score improved to 1.8 (IQR: 1.0–2.4). All patients expressed satisfaction with postoperative shoulder function recovery.
We performed statistical analysis of fracture healing times and upper limb functional recovery across different clavicle fracture types, along with a comparative analysis of functional recovery at various time points, as shown in Figure 3, Figure 4, and Table 1.
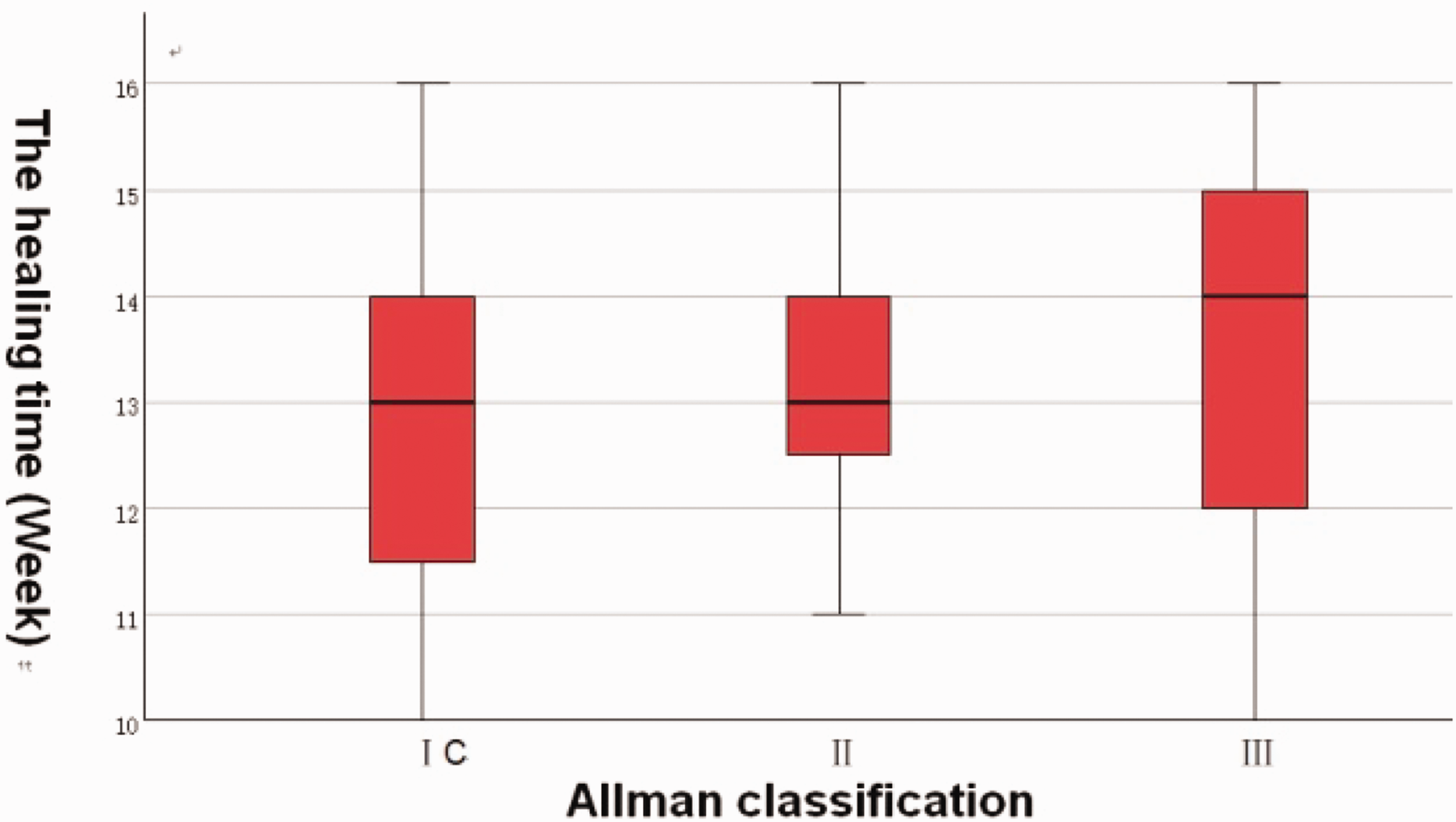
Pairwise comparisons of fracture healing times among different fracture types showed no statistically significant differences (P > 0.05).
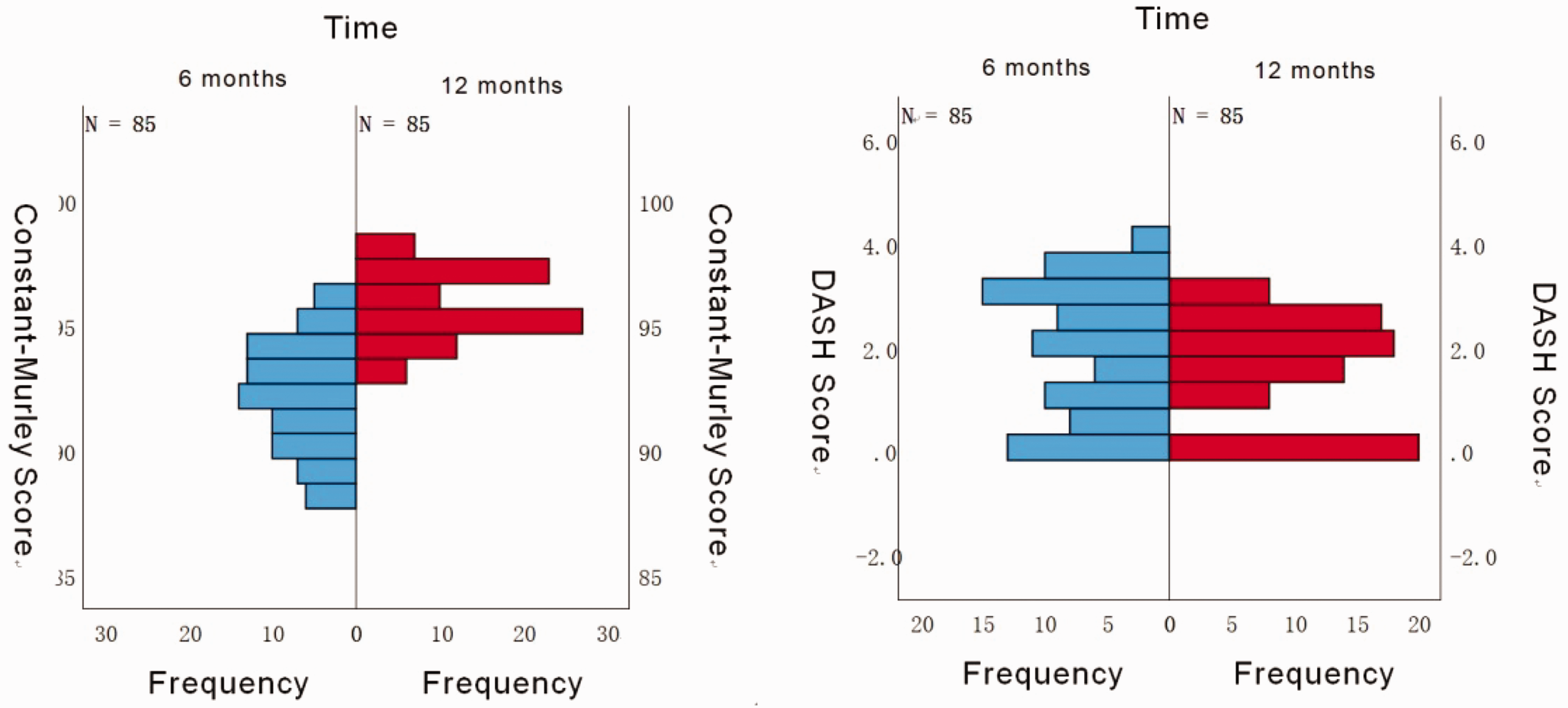
Group comparisons of functional scores at different time points using the Mann–Whitney U test showed statistically significant differences in Constant–Murley (P < 0.01) and DASH scores (P = 0.04), indicating superior upper limb function at 12 months postoperatively compared with 6 months postoperatively. DASH: disabilities of the arm, shoulder, and hand.
Pairwise comparisons of different fracture types using the Kruskal–Wallis H test at various time points (6 or 12 months) under the same functional scoring system showed no statistically significant differences (P > 0.05).

CMS: Constant–Murley score; DASH: disabilities of the arm, shoulder, and hand
Discussion
The clavicle is an important structure that connects the sternum and scapula, supporting the upper limb and transmitting mechanical loads. For most clavicular fractures, anatomical reduction is typically not required, as they do not directly involve the joint surface. Functional reduction is typically sufficient, aligning with the principles of conservative treatment for clavicle fractures.6,13 However, no clear standard for functional reduction exists. Studies14,15 have suggested that surgical intervention is warranted if clavicular shortening is ≥15 mm, if displacement is ≥21 mm, or if fracture displacement exceeds one shaft width with a shortening of >2 cm. 16 In contrast, minimal shortening or displacement generally does not affect upper limb function.13,17 In this study, we used a semi-open surgical approach, achieving reduction without periosteal incision or fracture end exposure. Despite limited visualization, some patients experienced minor shortening or lateral displacement postoperatively, with all patients meeting functional reduction criteria. At 6 months postoperatively, the CMS and DASH scores were recorded for all patients. Although there was a statistically significant difference (P < 0.05) in scores between 6 and 12 months, all patients reported satisfactory recovery of shoulder joint and upper limb function at both follow-up time points.
Reduction and fixation of free bone fragments during surgery are essential, as substantial displacement increases the risk of nonunion.
18
Additionally, the loss of cortical integrity can reduce plate stiffness,
5
and rotational displacement of butterfly fragments due to ligament traction may compress the subclavian nerve, causing symptoms. Nice knots, known for their simplicity, secure fixation, stable centripetal compression, and minimal disruption to surrounding tissues and blood supply, are widely used for fragment reduction and fixation in comminuted midshaft clavicle fractures.19–21 Its advantages have been extensively validated in previous studies.10,21,22 This study provided the following clinical insights on using Nice knots in semi-open surgeries:
Preoperative planning: Mark fracture ends and fragment locations on the skin using fluoroscopy, and plan the number and placement of Nice knots. For larger or butterfly fragments, knots are recommended at both ends for secure fixation. Simplified technique: Use a single guidewire initially, followed by threading of a double suture via the guidewire, to avoid repeated needle passes and streamline the procedure. Needle handling: Keep the needle close to the bone surface within the periosteum to avoid damaging underlying vessels and nerves. Suture positioning: Although outer cerclage wirings provide greater biomechanical stability for locking plates in comminuted midshaft clavicle fractures, inner cerclage wirings (ICWs) are recommended. ICWs are closer to the bone surface, offering stronger centripetal compression while effectively aiding fragment reduction and fixation.
23
Wu et al. 20 argued that the application of Nice knots requires the fracture line to not be overly perpendicular to the radial axis of the clavicle, as clavicle fractures with an angle of ≥45° between the fracture line and radial axis of the clavicle can become increasingly challenging or impossible to treat with this method. Although this perspective is geometrically and mechanically valid, we believe that it is less concerning in clinical practice. For fractures where the fracture line is perpendicular to the clavicle axis, such fractures typically lack bone fragments and can be treated with intramedullary nails. 7 If bone fragments are present, the fragment and thicker soft tissues attached to these fragments can act as a “bridge,” allowing the Nice knot to elastically stabilize the fracture ends, followed by locking plate fixation. In this study, stable fixation was achieved in all 84 patients, with only one case of plate breakage observed. We attribute this complication to the patient initiating weight-bearing activities 2 days postoperatively and failing to follow medical advice for limb suspension. Although locking plates provide reliable fixation, avoiding early weight-bearing and ensuring proper limb suspension postoperatively remain crucial.
An important factor in bone regeneration is the periosteum and blood supply. Knudsen et al. 24 found that the clavicle lacks nutrient artery, with the periosteum being the primary source of blood supply. A part of clavicular fractures experiences delayed union or nonunion healing due to unrestricted periosteal stripping and disruption of blood supply during surgery.25,26 Preserving the periosteum helps retain blood supply and local hematoma, which is formed from the blood within the marrow cavity and contains a large number of mesenchymal stem cells. 27 These cells are key contributors to the formation of callus at the fracture site; thus, preserving the periosteum and hematoma aids in the rapid healing of fractures.28,29 Owing to the protection of the periosteum and blood supply during surgery, the median healing time of 85 patients in our study was 13 weeks, which was comparable to that achieved via minimally invasive plate fixation or intramedullary nailing, as reported in the literature.7–9 No cases of nonunion were observed during follow-up. Preserving the periosteum maximizes fixation of fracture fragments and prevents detachment. The periosteum attached to the bone fragments can form a periosteal chain, assisting in fracture reduction and improving reduction stability. 21 Wang et al. 30 analyzed the relationship between soft tissue injury and postoperative complications, suggesting that more severe soft tissue damage is often associated with higher levels of postoperative exudate and swelling, increasing the risk of infection and soft tissue healing issues. We found that preserving the periosteum and a small amount of surrounding muscle tissue serves as a buffer, reducing postoperative inflammatory response and alleviating pain. Although no antibiotics were used for infection prevention in this study, no postoperative infections occurred, and all wounds healed well.
During the surgery, we carefully freed and protected the supraclavicular nerve and its branches. However, 6 (7.1%) patients developed numbness in the subclavian region postoperatively. At the final follow-up, all patients reported a reduction in numbness, with no impact on daily life. We hypothesized that this may be related to intraoperative traction, postoperative scar formation, and plate compression. Ou et al. 31 reported that skin sensation loss due to supraclavicular nerve injury is most severe in the first month postoperatively; however, it does not significantly affect daily activities, with 98.5% of patients experiencing gradual symptom resolution. Intraoperative nerve dissection and protection are crucial to avoid iatrogenic nerve damage, which can lead to neuroma formation and subsequent pain and neck–shoulder discomfort.31,32
We performed a grouped analysis of comminuted clavicular fractures based on the Allman classification. We found no significant differences in fracture healing time or upper limb function recovery across different types of clavicular fractures, with all clinical outcomes being satisfactory. This also suggests that the surgical approach is suitable for treating comminuted clavicular fractures at various locations. In this study, we prioritized soft tissue preservation and successful fracture healing over achieving perfect anatomical reduction and aesthetic imaging. This change in approach, or more accurately, the shift in concept, allows the surgeon to complete the procedure quickly (65.0 min) with minimal tissue trauma and blood loss (29.0 mL).
This study had several limitations. It did not include a control group and primarily introduced a novel surgical technique and concept, summarizing the clinical efficacy of Nice knot–assisted locking plates for treating comminuted clavicular fractures with periosteal preservation. As such, attributing the positive clinical outcomes solely to periosteal protection and the use of double-suture Nice knot may lead to bias. Additionally, this is a single-center retrospective study with a relatively short follow-up period, and long-term outcomes require further investigation. A larger sample size is needed to validate the comparisons between different types of clavicular fractures.
Conclusions
The semi-open surgical approach—periosteum-preserving clavicular internal fixation—offers advantages such as minimal trauma, simplicity, low intraoperative blood loss, and rapid fracture healing, allowing for rapid functional reduction of clavicular fractures. This method remains unaffected by fracture type, with satisfactory clinical outcomes and high safety, making it a reliable treatment option.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to our colleagues for their unwavering support and collaboration throughout the research process. Their invaluable insights and assistance have greatly contributed to this study. We also extend our heartfelt thanks to the hospital administration for providing the necessary platform and resources that facilitated the execution of our research.
Author contributions
Jingquan Guo: Conceptualization, Experimental design, Methodology, Writing—original draft.
Bo Wu: Surgical technique guidance, Experimental design, Writing—review & editing.
Fei Xiao: Surgical technique guidance, Statistical analysis.
Keke Cheng: Surgical assistance, Data curation, Data analysis.
Tianrun Lei: Surgical assistance, Data collection.
Consent to participate
Written informed consent was obtained from each enrolled patient.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Data availability statement
The data supporting the findings of this study are openly available. The data can be accessed without any restriction.
Ethics considerations
Ethical approval for this retrospective study was obtained from the ethics committee of the Wuhan Fourth Hospital (KY2024-176-01).
Funding
No funding was received for this research.