
Abstract
Background
The thymidine phosphorylase (TP) enzyme has several tumor-promoting functions. The aim of this study was to explore TP gene expression in relation to clinical and histopathological data obtained from patients with stage III colorectal cancer.
Methods and Results
TP gene expression was analyzed by real-time quantitative PCR in tumor and mucosa samples from 254 patients. TP gene expression in tumors correlated with lymph node staging, with higher expression relating to a higher number of positive nodes and a worse N-stage. Higher TP expression was also associated with a worse histological tumor grade. Patients with rectal cancer had significantly higher TP expression in mucosa and tumors compared with patients having colon cancer.
Conclusion
Higher intratumoral TP expression appears to be related to a worse N stage, and thus, with a worse prognosis. TP gene expression measured in a preoperative biopsy could be of interest in preoperative staging.
Introduction
Worldwide, colorectal cancer is the third most commonly diagnosed cancer, with over 1.2 million new cases a year. 1 The curative treatment for colorectal cancer is surgery with radical tumor removal. Some patients receive adjuvant chemotherapy to improve the long-term outcome. The indication for chemotherapy is founded on risk assessment by TNM, staging and chemotherapy is mainly used in stage III disease, defined by lymph node involvement. 2 The beneficial effect of chemotherapy is well studied, but remains at a group level. 3 The efficacy for the individual is as yet unknown and must be weighed against the risk of treatment-related side effects. Identification of prognostic and predictive markers in colorectal cancer will enable individualized treatment.
The thymidine phosphorylase (TP) enzyme (E.C. 2.4.2.4) catalyzes reversible phosphorylation of thymidine to thymine, thus contributing to the regulation of deoxythymidine monophosphate pools in cells. 4 TP activity is thought to limit possible substrate toxicity and prevent replication errors during DNA synthesis. 5 TP has been shown to be elevated in a wide variety of solid tumors, including colorectal carcinomas.4,6–8 TP is expressed in tumor epithelial cells and in the tumor stroma by fibroblasts and infiltrating macrophages and stimulates tumor growth by promoting angiogenesis and by conferring resistance to apoptosis.7,9–12 In addition, TP is involved in the metabolism of 5-fluorouracil (5-FU), one of the most commonly used chemotherapeutic drugs for colorectal cancer, as well as in the conversion of the oral prodrug, capecitabine, to 5-FU. 10
In a previous study, we found that TP had a predictive value for response to chemotherapy in patients with metastatic stage IV colorectal disease and was also of prognostic value for overall survival. 5 The role of TP in the adjuvant setting has not been thoroughly investigated and is still unclear.13–16 The hypothesis of the present study was that increased TP expression relates to increased tumor activity and thus to a more aggressive tumor or stage. The aim of the present study was to relate TP gene expression to clinical and histopathological data obtained from patients with stage III colorectal cancer treated with adjuvant 5-FU-based chemotherapy.
Materials and Methods
Patients
In the period from November 2001 until August 2009, 375 patients underwent surgery for colorectal cancer and were treated with adjuvant 5-FU-based chemotherapy for stage III disease at the Sahlgrenska University Hospital, Östra. Tissue samples were available for 254 patients, all of whom were included in the study. All patients underwent radical surgery for a colorectal adenocarcinoma. Two hundred and thirty-nine patients were treated according to the Nordic FLV-protocol based on 500 mg/m2 of 5-FU in combination with 60 mg/m2 of leucovorin. The chemotherapy was given as a weekly intravenous bolus injection for six months. Ninety-three of the patients also received intravenous oxaliplatin, 85 mg/m2 every other week, and one patient received additional irinotecan. Fifteen patients received the oral 5-FU prodrug capecitabine. Seventy-five patients with rectal tumors were subjected to preoperative radiotherapy according to national treatment guidelines. Clinical data on demography and pathology were retrieved as well as treatment information, including chemotherapy-related side effects. TP gene expression in tumor tissue and normal-appearing mucosa was assessed in relation to demography and pathology factors such as lymph node involvement and tumor differentiation grade as well as treatment-related risks of adverse effects. Cancer staging was done in accordance with the seventh edition of the UICC/TNM system. 2 The local ethics committee approved the study, and informed consent was obtained from each of the patients.
Total RNA extraction, cDNA preparation and real-time quantitative PCR
Tumor samples (n = 254) and matched macroscopically normal-appearing mucosa (obtained approximately 10 cm from the tumor, n = 252) were snap-frozen in liquid nitrogen after removal and stored at −70 °C until used. Total RNA was isolated from 10–30 mg of fresh-frozen tissue using the High Pure RNA Tissue Kit (Roche Diagnostics GmbH) according to the manufacturer's instructions. cDNA was synthesized using the High Capacity cDNA Reverse Transcription Kit (Applied Biosystems) and run on a Perkin Elmer Gene Amp PCR System 9600 system. The presence of DNA was checked by using samples without addition of reverse transcriptase. Real-time quantitative polymerase chain reaction (PCR) was performed using the 7500 Fast Real-Time PCR system (Applied Biosystems). The expression of the target gene, thymidine phosphorylase, was quantified using assay-on-demand from Applied Biosystems (Hs00157317_m1). The TaqMan® assay consisted of unlabeled PCR primers, a TaqMan® MGB probe [carboxyfluorescein-labeled, emission maximum 518 nm] and a nonfluorescent quencher. The reporter dye signal was measured against the internal reference signal [6-carboxy-X-rhodamine, emission maximum 610 nm] to normalize for non-PCR-related fluorescence. The housekeeping gene, β-actin, was used as an endogenous control to compensate for variation in the amount of RNA and to check the efficiency of the reverse transcription reaction. The reporter dye for β-actin was VIC (emission maximum 552 nm) and the quencher dye was 6-carboxytetramethylrhodamine (TAMRA, emission maximum 582 nm). The following primer and probe sequences were used, TP, probe:5′-CAG CCA GAG ATG TGA CAG CCA CCG T-3′, forward primer:5′-CCT GCG GAC GGA ATC CTA TA-3′, reverse primer:5′-TGT GAT GAG TGG CAG GCT GT-3′; and for β-actin, probe:5′-CCT GAA CCC CAA GGC CAA CCG-3′, forward primer:5′-CGT GCT GCT GAC CGA GG-3′, reverse primer:5′-GAA GGT CTC AAA CAT GAT CTG GGT-3′. The PCR primers and the TaqMan fluorogenic probes were designed using the Primer Express software program. Multiplex PCR was performed as follows:27.5 μL of the TaqMan Fast Universal PCR master mix (with no AmpErase UNG), were mixed with 2.75 μL of the target primers (final concentration 300 nM) and probe (final concentration 200 nM), and 9.75 μL of β-actin primers and probe (final concentration 100 nM). Next, 10 μL of the samples were added in triplicates to the 96-well plate and analyzed. A negative control was included in each run. The program started with incubation for 20 seconds at 95 °C and thermal cycling then proceeded with 40 cycles of 95 °C for 3 seconds and at 60 °C for 30 seconds. Quantitative data were calculated according to the instructions given by Applied Biosystems.
Statistical Methods
The JMP 8.0/SAS software program (SAS Institute, Cary, NC) was used for the statistical analysis. The data were assessed by descriptive statistics, and t-testing, analysis of variance, or Spearman correlation was used for parametric data. Contingency tables with the Chi-square/Kruskal-Wallis test were used for nonparametric data. Results found to be significant by parametric tests were cross-checked by nonparametric tests. The Pearson correlation coefficient (r) was used to compare sets of continuous parameters measured in the same tissue. The confidence level was set at 95%.
Results
TP gene expression according to patient characteristics
Patient and pathology data are presented in Table 1. The median age of the patients was 64 (interquartile range 57–75) years with an even gender distribution. The expression of TP in mucosa (mTP), correlated negatively with age (r = −0.14, P = 0.026) but not in tumor samples (tTP). No difference in tTP or mTP expression was seen according to gender. The mean ± standard deviation (SD) mTP was 0.32 ± 0.25 and the mean tTP was 0.35 ± 0.43. The mean difference between tumor and mucosa expression was 0.035 ± 0.47. There was no correlation between mTP and tTP gene expression. As shown in Table 2, a worse local T stage was not related to higher tTP The higher the tTP expression, the worse was the N group (P = 0.0020, Table 2). Furthermore, there was a positive correlation between tTP gene expression and the number of positive lymph nodes (r = 0.15, P = 0.014), as well as a significant association between tTP and TNM node stages. The tumor differentiation grade was also associated with the tTP level, which increased as the grade worsened (P = 0.033, Table 2). Mean tTP expression was higher in rectal tumors than in colon tumors (0.46 ± 0.54 and 0.27 ± 0.29, respectively, P = 0.0002). In rectal mucosa, the level was 0.37 ± 0.25 compared with 0.28 ± 0.24 in colon mucosa (P = 0.0018). When patients with rectal tumors were subgrouped according to preoperative radiation (yes/no), the TP expression was found to be significantly higher in irradiated than in non-irradiated mucosa (0.40 ± 0.26 versus 0.30 ± 0.22, P = 0.035). However, there was no significant difference in TP expression between irradiated and nonirradiated rectal tumors (0.46 ± 0.45 and 0.44 ± 0.67, respectively, P = 0.097).
Patients (n = 254) and tumor characteristics.
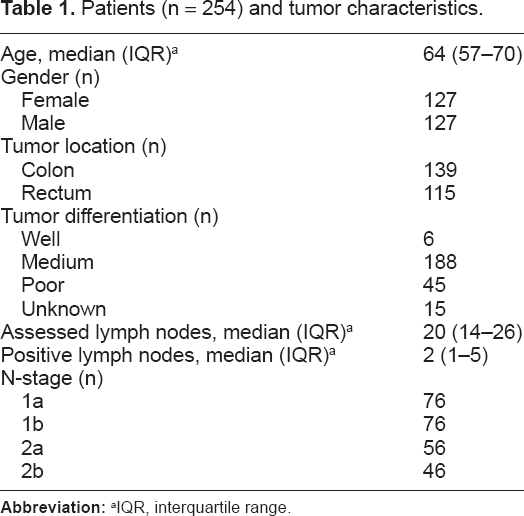
IQR, interquartile range.
TP gene expression in colorectal tumors of stage III patients by pathology factors.

Ten tumors with unknown T-stage were excluded from the statistical calculation
fifteen tumors of unknown grade were excluded from the statistical calculation.
TP gene expression according to treatment and side-effects
The tTP or mTP expression levels were not associated with risk or degree of specific chemotherapy-related side effects, including diarrhea, stomatitis, lethargy, nausea, vomiting, leucopenia, thrombocytopenia, or dermatologic or ophthalmologic problems. However, the risk of need for dose reduction during treatment was linked to higher tTP expression (P = 0.007). Patients who pre-emptively terminated their adjuvant treatment due to toxicity (n = 44) had higher mTP (but not higher tTP) expression than patients completing therapy at the normal dosage (n = 176, P = 0.034).
Discussion
Lymph node involvement is the most important feature of stage III colorectal cancer and thus is a marker of a worse prognosis. The finding of a correlation between TP gene expression in the tumor and the degree of node metastasis in the present study is interesting, given that node positivity, both in absolute figures and as a ratio, is strongly linked with outcome.3,17–19 The differentiation grade has been shown to correlate with both local T stage, and nodal N stage and is thus linked to the overall cancer stage. 20 The result showing that the TP expression was lowest in well differentiated and highest in poorly differentiated tumors might thus be of importance.
In a previous study, Mimori et al 21 showed that TP mRNA detected by in situ reverse-transcriptase PCR was comparable with TP enzyme activity detected by high-performance liquid chromatography and enzyme assay. A higher tTP expression was associated with a more advanced Dukes’ stage which is in line with our findings. Similar results have been reported by Takebayashi et al 11 who, using immunohistochemistry, found a positive TP protein expression associated with a more advanced Dukes’ stage, as well as with lymph node metastasis and extensive angiogenesis. However, no significant association between TP protein expression and histological grade was found. In addition, Nishimura et al 13 found no differences in clinicopathological features between high and low TP protein expression levels.
The cause of these discrepancies may be explained on several levels. For instance, the tissue material used for analysis might be obtained and handled in different ways, and different experimental techniques (eg, immunohistochemistry or real-time quantitative PCR) might be used for detection of TP expression. Lassmann et al 22 for example, performed quantitative reverse-transcriptase PCR on microdissected tumor cells. The results showed a significant reduction in TP with increasing N and T stages. In the present study, biopsy samples containing both epithelial and stroma cells were analyzed and the opposite result was found. Given that much of the TP expression seems to be localized to tumor-associated macrophages (TAMs) in the stroma, 23 the amount of epithelial cells in relation to stroma cells in the analyzed tissue will surely affect the mean TP expression level. The composition of the patient cohort with regard to demographic and clinicopathological parameters may also influence the results. In the present study, TP gene expression in the mucosa was found to decrease with patient age, and significantly higher TP expression was detected in rectal mucosa and tumor tissue than in colon mucosa and tumor tissue.
The carbamate, capecitabine, has evolved as a candidate in the management of colorectal cancer. 23 This oral prodrug is metabolized to 5-FU in three steps, the last of which is catalyzed by TP. Thus, higher expression of TP, which has been found in tumor tissue compared with normal tissue by several groups,4,6,15,24 might allow for selective toxicity in tumors during treatment with capecitabine. However, the results of the present study did not show any significant difference in mean TP expression between tumor tissue and mucosa, nor did the earlier results of Zimovjanova et al 25 or Lassman et al. 22 The origin of the mucosa sample (eg, colon or rectal) and the distance between the mucosa sample site and tumor (10 cm in the present study) may have possibly affected the results.
The present study showed that TP expression was high in both irradiated and nonirradiated rectal tumors. However, TP expression in rectal mucosa was significantly higher in patients who had been treated with, preoperative radiotherapy than in those who were not treated in this way. As shown by Kim et al, 23 radiation induced monocyte-chemoattractant protein-1 expression in cancer cells, causing circulating monocytes to be recruited into TAMs, which then upregulated TP expression in rectal cancer tissue. Expression of TP was significantly elevated by low doses of radiotherapy (9 Gy) in most rectal cancer tissues. Thus, improvement of the efficacy of capecitabine through enhanced levels of tTP may be achieved by radiotherapy. These findings could support the use of capecitabine in combination with radiotherapy in neoadjuvant treatment of rectal cancer, and especially in patients with high TP expression, because it might further enhance the chances of tumor downstaging and downsizing, as has been shown by Sawada et al 26 in colorectal human cancer xenografts. The finding that higher mTP expression was related to pre-emptive termination of treatment could be of future predictive interest when adjuvant chemotherapy using 5-FU-related drugs is considered. However, the absence of any significant correlation between TP expression and specific side effects makes use of TP as a predictive marker difficult to evaluate.
The risk of dying from cancer is mainly linked to the development of generalized disease with distant metastasis, and has not been changed by improvements in surgery. Current studies address the possibility of starting with a systemic treatment to target circulating tumor cells and minor tumor cell complexes before introducing the inflammatory trauma of surgery and the treatment delay it may cause. We conclude that TP is a potential marker for the risk of node metastasis and stage III disease that could aid in patient selection and in optimizing individual treatment. The results of the present study could thus be of future interest in a preoperative setting where both radiological findings and tissue analysis of biopsy samples could be assessed for the risk of node metastasis.
Conclusion
Intratumoral TP gene expression was related to the degree of lymph node metastasis and the tumor differentiation grade, with a higher expression relating to worse staging, which, through the strong prognostic factors of the TNM system, relates to a worse prognosis. Such information regarding TP expression, obtainable from analysis of a preoperative biopsy, could be of importance when considering neoadjuvant chemotherapy.
Author Contributions
Conceived and designed the experiments: EBL, YW, KD, EO, BG. Analysed the data: EBL, YW, KD. Wrote the first draft of the manuscript: EBL. Contributed to the writing of the manuscript: YW, KD. Agree with manuscript results and conclusions: EBL, YW, EO, BG, KD. Jointly developed the structure and arguments for the paper: EBL, YW, KD. Made critical revisions and approved final version: EBL, YW, EO, BG, KD. All authors reviewed and approved of the final manuscript.
Funding
This work was supported by grants from the Swedish Cancer Society; and Grants from the Swedish state under the LUA-ALF agreement, the Assar Gabrielsson Foundation for Cancer Research, the Gothenburg Medical Society, and the Anna-Lisa and Bror Björnsson Foundation.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgements
We acknowledge the technical skills of M Åkerström and J Flach in this work. We also thank H Björkqvist and A-L Helminen for collecting the surgical samples and L Munro and B Sjöberg for their work on the clinical database.