
Abstract
Background:
No.253 lymph node is the gateway to systemic metastasis for left-sided colorectal cancer. However, the value of D3 resection is still controversial. This study aimed to identify the incidence rate and prognostic value of 253LN metastasis in patients with left-sided colorectal cancer liver metastasis (CRLM) mainly through blood vessels and thus to provide theoretical basis for 253LN resection.
Methods:
From February 2012 to February 2019, a total of 281 patients who underwent curative resection for both primary and metastatic tumors were collected retrospectively. The clinicopathological and genetic characteristics were compared between 58 patients with positive 253LN and 223 patients with negative. Relapse-free survival (RFS) and overall survival (OS) were compared with Kaplan–Meier method. Cox regression analysis and a forest plot were conducted for RFS.
Results:
The incidence of 253LN metastasis in left-sided CRLM was 20.64% (58/281). Those with 253LN positive were T4 stage, N2 stage, and D1/D2 lymph nodes metastatic. About 10.3% (8/78) 253LN positive patients were D1/D2 negative. The 253LN metastasis was an independent risk factor for relapse after curative surgery, but not for OS. Patients with 253LN metastasis had worse RFS, especially in female, adenocarcinoma, poorly differentiated, pT3, preoperative serum CA199 < 37 U/mL, bilobar liver metastasis, without preoperative chemotherapy, KRAS, NRAS, or BRAF wild type.
Conclusion:
The incidence of 253LN metastasis in left-sided CRLM is 20.64%, and skip metastasis rate is 10.3%. The 253LN status is an independent prognostic risk factor for RFS but not for OS after curative surgery. Routine resection of 253LN should be applied in curative surgery of left-sided CRLM.
Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide, which ranks the second in mortality. 1 Colorectal cancer liver metastasis (CRLM) is the main cause of death. 2 Unfortunately, about 50% CRLM patients would develop liver metastasis eventually. 3 Despite hepatectomy provides potential chance of cure, the problem that recurrence rate is up to 50% within 2 years after surgery, 4 is still to be solved.
No.253 lymph node (253LN), also known as inferior mesenteric artery (IMA) lymph node, is categorized as D3 loco-regional lymph node in Japanese Society for Cancer of the Colon and Rectum (JSCCR) guideline. 5 The 253LN is the gateway to systemic metastasis, and positive 253LN has been reported as an independent predictive factor for recurrence and poor prognosis.6,7 However, the value of D3 resection is still controversial. D3 resection, usually along with high ligation of IMA, is considered as radical but of limited benefit for the low positive rate of 253LN, while low ligation without D3 excision reserves the left colonic artery blood supply, thus results in less complications.8-10 As a result, low ligation with D3 excision appeared but results in more complexity and longer surgery time. Whether 253LN should be dissected routinely is subject to debate. Furthermore, previous researches focus mainly on stage I to III CRC patients. Few data and evidence can be referred in stage-IV patients.
This study aimed to identify the incidence rate, prognostic value of 253LN, thus to decide whether D3 resection should be applied routinely in patients with left-sided CRLM, which is mainly through blood vessels.
Methods
Patients
From February 2012 to February 2019, 281 consecutive patients with left-sided CRC (left-sided colon and rectal cancer) liver metastasis at Zhongshan Hospital in Shanghai were enrolled in this retrospective study. Inclusion criteria were as follows: (1) from 18 to 80 years old; (2) primary tumor was located in descending colon (including splenic flexure), sigmoid colon, and rectum; (3) underwent curative resection for both primary and metastatic tumors in one time or two times; (4) No.253 LN status was available; and (5) CRLM verified by pathology reports after surgery. Exclusion criteria were as listed: (1) unresectable extrahepatic metastasis; (2) history of hereditary CRC (FAP, Lynch Syndrome, and so on); (3) multiple primary tumors including right-sided colon; (4) incomplete data. Statistics on 253LN was obtained after surgery. A study flow chart was constructed (Figure 1).

The study flow chart.
Surgical technique
The surgery we adopted was the low ligation of artery with D3 excision. In detailed, for patients with cancer in rectum and distal sigmoid colon, we reserved the left colon artery, and ligated the sigmoid colon artery and the superior rectal artery. For patients with cancer in proximal sigmoid colon, the superior rectal artery and the left colon artery were preserved, and the sigmoid colon artery was severed. For patients with cancer in descending colon including splenic flexure, only the left colonic artery was cut. 253LN was dissected for all patients, and regional lymph node dissection was also performed according to the principle of curative-intent treatment. In the operating theater, 253LN was isolated from the surgical specimen and sent for pathological examination separately, to ensure the quality of pathological report.
Follow-up
We evaluated patients every 2 to 3 months for the first 2 years since surgery, every 6 months for the following 3 years, and once a year thereafter. Every time follow-up, physical examination, serum CEA and CA19-9 level tests, chest computed tomography (CT) scan, abdominal CT and magnetic resonance imaging results were recorded. The same as colonoscopy once a year. The endpoint consisted of tumor relapse (for relapse-free survival [RFS]) or death (for OS), and loss to follow-up (for both). The median time of follow-up for RFS and OS was calculated with reverse Kaplan–Meier method.
Statistical analysis
Statistical analysis was performed by R project, version 4.0.3 (R Project for Statistical Computing, RRID: SCR_001905). The difference of continuous variables was compared using Wilcoxon rank sum test with continuity correction, and categorical variables were compared using Pearson’s chi-squared test, chi-square with continuity correction, and Fisher’s exact tests when appropriate.
Relapse-free survival and OS were compared using the Kaplan-Meier method with a log-rank test. Variables available before surgery including sex, age, primary tumor location, primary tumor size, histology, differentiation, T stage, preoperative serum CEA and CA199 levels, size of largest LM, number of LM and distribution of LM, extrahepatic metastases, curative surgery, surgery approach, KRAS, NRAS and BRAF, preoperative chemotherapy, were filtrated by univariate cox proportional hazards model first, then those with p < 0.10 was incorporated into multivariate analysis. Nomogram was constructed to calculate the risk of recurrence for the 1 year, 2 year, and 3 year after surgery respectively (Table S1). A forest plot was made for subgroups analysis. Furthermore, recurrence pattern was explored in detailed.
Logistic regression was used to identify the factors available before surgery related to 253LN metastasis. The significant levels for univariate and multivariate were set as 0.10 and 0.05 (Table 1).
Logistic regression analysis for metastatic status of No.253 lymph nodes.
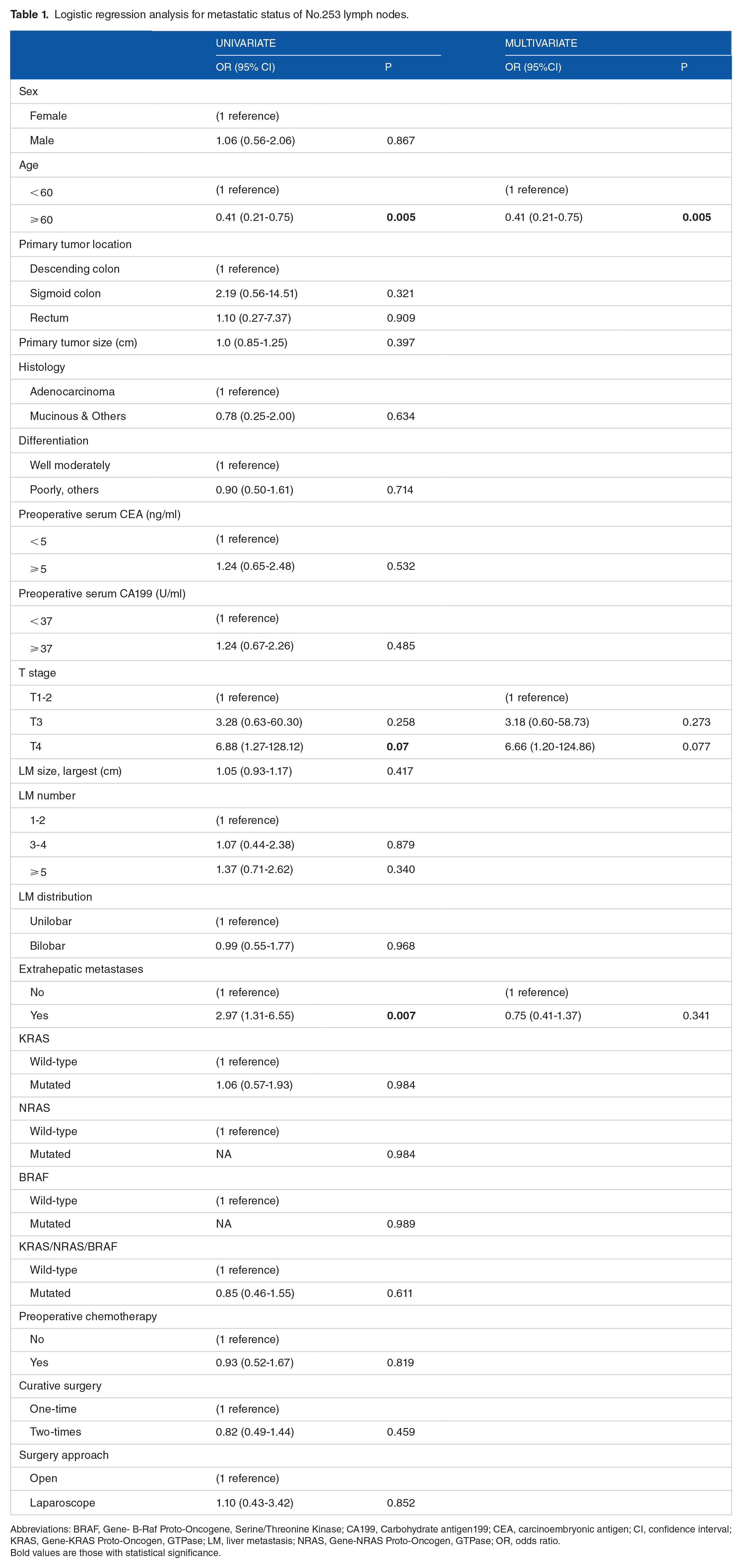
Abbreviations: BRAF, Gene- B-Raf Proto-Oncogene, Serine/Threonine Kinase; CA199, Carbohydrate antigen199; CEA, carcinoembryonic antigen; CI, confidence interval; KRAS, Gene-KRAS Proto-Oncogen, GTPase; LM, liver metastasis; NRAS, Gene-NRAS Proto-Oncogen, GTPase; OR, odds ratio.
Bold values are those with statistical significance.
Ethical statements
This study was approved by the Ethics Committee of Zhongshan Hospital, Fudan University. Approval number: B2017-166R. Approval date: January 23, 2018.
Result
Clinicopathological characteristics
Clinicopathological characteristics were summarized (Table 2). Among a total of 281 patients who underwent curative resection, 58 (20.64%) were 253LN metastatic. The median age of diagnosis is 59 (IQR:53-67). Positive rate of 253LN was higher in patients with more advanced T and N stage, as 0 in T1, 1 (6.7%) in T2, 35 (17.9%) in T3, 22 (31.4%) in T4, and 0 in N0, 15 (25.9%) in N1, 43 (74.1%) in N2. Especially, 8 (10.3%) patients were 253 LN positive while D1/D2 negative (Figure 2). Other clinicopathological characteristics were similar between the two groups, including sex, primary tumor location, primary tumor size, histology, differentiation, preoperative serum CEA and CA199, size of largest LM, number and distribution of LM, extrahepatic metastases, curative surgery, surgery approach, KRAS, NRAS, BRAF, and preoperative chemotherapy. The median number of harvested lymph nodes is 17 (14.0-22.0).
Baseline of clinicopathological characteristics of patients.

Abbreviations: BRAF, Gene- B-Raf Proto-Oncogene, Serine/Threonine Kinase; CA199, carbohydrate antigen199; CEA, carcinoembryonic antigen; KRAS, Gene-KRAS Proto-Oncogen, GTPase; LM, liver metastasis; NRAS, Gene-NRAS Proto-Oncogen, GTPase.
Bold values are those with statistical significance.

Distribution of No.253 LN: (A) T stage: T1-2 < T3 < T4, P = .046; (B) N stage: N0 < N1 < N2, P < .001; (C) D1 and D2 status: D1 and D2 ⩽ D1 or D2+, P = .012.
Relapse-free and overall survival
RFS in negative 253LN group was significantly better than that in positive group (median RFS time:16.6 vs 12.3 months, P = .012; 1 year RFS, 2 year RFS, 3 year RFS: 60.0% vs 50.0%, 35.1% vs 22.2%, 29.2% vs 12.7%, respectively) (Figure 3A), while OS was not (median OS time: 62.3 vs 52.6 months, P = .18; 1 year OS,2 year OS, 3 year OS,5 year OS: 97.2% vs 94.8%, 85.2%vs 75.3%, 72.9% vs 67.3%, 50.3% vs 47.0%, respectively) (Figure 3B). The median follow-up time for RFS was 31.6 months, and for OS was 45.8 months. Multivariate cox regression analysis showed that 253LN status was an independent risk factor for left-sided CRLM relapse after curative surgery (HR, 1.42; 1.01-1.99), P = .043; Table 3).
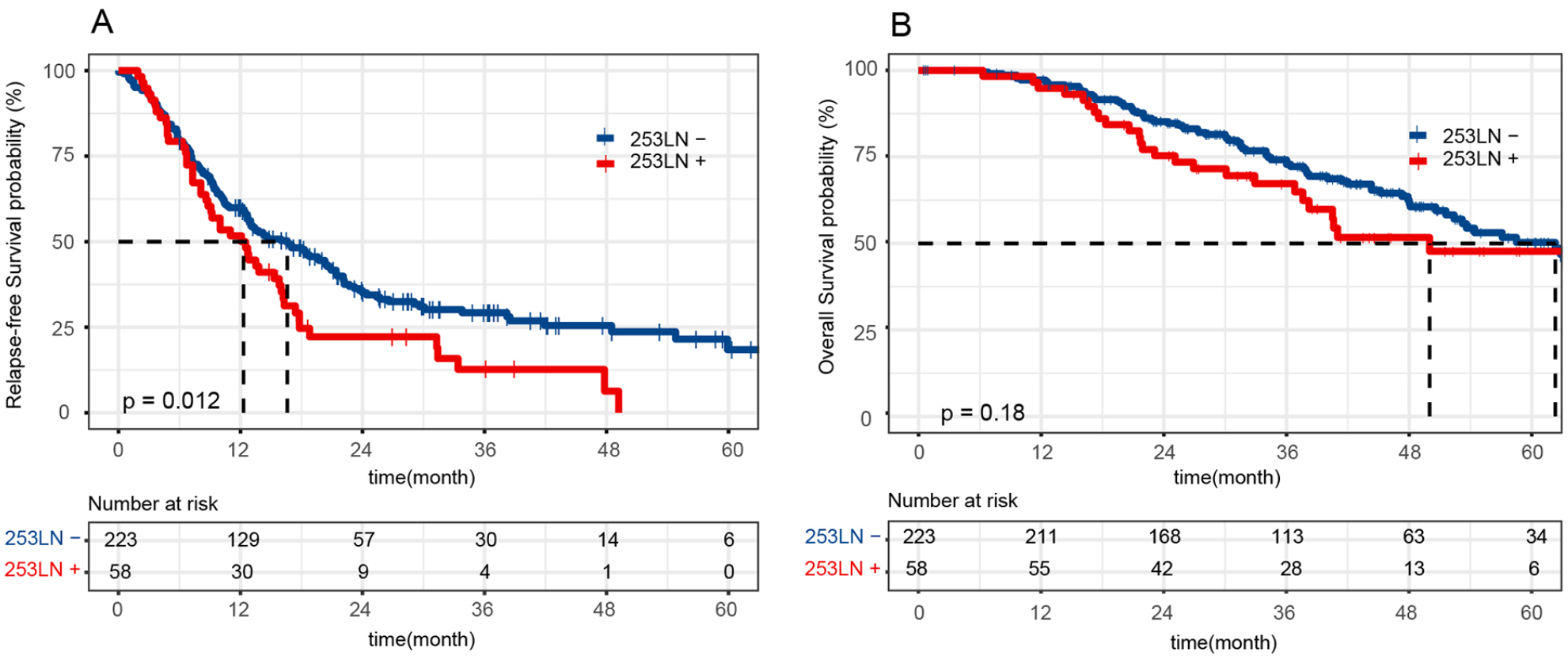
Kaplan–Meier survival plots for RFS and OS: (A) median RFS time of 253LN− and 253LN+: 16.6 vs 12.3 months, P = .012; 1 year RFS, 2 year RFS, 3 year RFS: 60.0% vs 50.0%, 35.1% vs 22.2%, 29.2% vs 12.7%, respectively. (B) Median OS time: 62.3 vs 52.6 months, P = .18; 1 year OS, 2 year OS, 3 year OS, 5 year OS: 97.2% vs 94.8%, 85.2%vs 75.3%, 72.9% vs 67.3%, 50.3% vs 47.0%, respectively.
Cox regression analysis for relapse-free survival of CRLM.

Abbreviations: BRAF, Gene- B-Raf Proto-Oncogene, Serine/Threonine Kinase; CA199, carbohydrate antigen199; CEA, carcinoembryonic antigen; CI, confidence interval; CRLM, colorectal cancer liver metastasis; HR, hazard ratio; KRAS, Gene-KRAS Proto-Oncogen, GTPase; LM, liver metastasis; LN, lymph nodes; NRAS, Gene-NRAS Proto-Oncogen, GTPase.
Bold values are those with statistical significance.
Subgroup analysis
Forest plot was designed for subgroup analysis, and we recognized that patients with 253LN metastasis had worse RFS, especially in those who were female, adenocarcinoma, poorly differentiated or others, T3 stage, preoperative serum CA199 < 37 U/mL, bilobar liver metastasis, without preoperative chemotherapy, KRAS, NRAS, and BRAF wild-type (Figure 4). Furthermore, result of recurrence pattern showed that patients with 253LN positive tented to have recurrence in lung, celiac lymph nodes (P < .001) or multiple sites (P = .003) (Table 4). The difference between the location of recurrence and the location of extrahepatic metastases are significant in statistics (P = .025), but no meaningful trend was found in medicine (Table S1).

Forest plot for subgroups analysis of relapse-free survival.
Recurrence pattern after curative operation for left-sided CRLM.

Abbreviation: CRLM, colorectal cancer liver metastasis.
Discussion
In this study, 58 (20.64%) were 253LN positive, which was higher than that of stage-III CRC patients, ranging from 0.3% to 13.5%.8,11 Furthermore, we found that 253LN metastasis stood for shorter RFS time, even in those with LM. Therefore it is meaningful to resect 253LN routinely in left-sided CRLM.
Unlike tumor node metastasis (TNM) system, JSCCR guidelines takes the distribution of lymph nodes into account, in which 253LN is defined as local lymph nodes, as well as the last gate of lymph drainage before systemic metastasis. In theory, metastatic 253LN without D3 resection is not curative-intent, which brings the risk of recurrence and distant metastasis after surgery. That is the reason why most authors studied the value of 253LN in stage-III CRC patients. Jin-Wook Yi et al 11 thought only 253LN could not indicate a poor outcome, while Xiao-Jie Wang et al 12 recognized it as an independent prognostic factor for 5 year RFS (24.4% vs 61.8% for 253LN+ and 253LN−). Whether positive 253LN influence CRC patients’ prognosis is still in debate. On one hand, traditionally, those were opposed to routine D3 resection mainly because low positive rate of 253LN in stage-III CRC.8,11 However, in our study, we found 20.64% positive rate in left-sided CRLM, almost double than stage III, which meant greater benefit after D3 resection. On the other hand, patients with negative 253LN had significantly better RFS than 253LN positive (median RFS time: 16.6 vs 12.3 months, P = .012; 1 year RFS, 2 year RFS, 3 year RFS: 60.0% vs 50.0%, 35.1% vs 22.2%, 29.2% vs 12.7%, respectively), and 253LN was identified as an independent prognostic factor by cox regression analysis. Then, forest plot for subgroup analysis showed that positive 253LN was relative to poorer RFS in patients, especially who were female, adenocarcinoma, poorly differentiated or others, T3 stage, preoperative serum CA199 < 37 U/mL, bilobar liver metastasis, without preoperative chemotherapy, KRAS, NRAS, and BRAF wild-type. Moreover, recurrence pattern was analyzed, and we found pulmonary, celiac lymph nodes (P < .001) and multiple sites metastasis (P = 0.003) occurred more frequently in patients with positive 253LN, which might be the reason why positive 253LN stood for poorer RFS. The difference between the location of recurrence and the location of extrahepatic metastases are significant in statistics, but not meaningful in medicine. As a result, it is reasonable to believe that, even though liver metastasis has occurred, 253LN metastasis still results in worse RFS after curative resection surgery.
In Operation for CRC: low anterior resection, Cohen pointed out that even if 253LN was resected routinely in surgery, better curative-intent outcome was still hard to achieve for patients’ advanced stage. Similar research was also published later, 13 and we only found that patients with 253LN metastases had worse RFS but not OS either in this study. However, with reference to Evolving Oncology Endpoints — A New Horizon for Oncology Endpoints reported by IQVIA Institute, there seems a link between RFS and OS, and benefits in RFS may be translated into potential benefits in OS. 14 Since this is a retrospective study and the total number of patients enrolled is limited, the prediction value of 253LN for OS may not be fully reflected. Moreover, better RFS mean higher quality of life for patients after curative surgery, even if there is really no improvement in OS, we still believe that it is worthwhile to resect 253LN in left-sided CRLM patients.
Some authors pointed out that tumor size, number of metastatic lymph nodes, T-stage and N-stage were related to 253LN metastatic,11,15,16 but some of these data can only get during or after surgery. Few models have been constructed to predict 253LN status before surgery, which is critical for precise treatment. Based on data available preoperative to predict 253LN status, only age < 60 years old was recognized as independent factor by logistic regression analysis, and the effect of prediction was not ideal enough, which reminded that genomics or proteomics might be needed as predictive factors.
Interestingly, “skip metastasis” was also observed in our study. “Skip metastasis” was defined as local lymph nodes metastasis in a discontinuous pattern. We found skip metastasis occurred in 10.3% left-sided CRLM patients, higher than 6% in stage-III CRC patients, 7 which supported D3 resection for a more precious N stage.
There were many poorly differentiated tumors in this study. CRLM tends to indicate aggressive behavior, which often results in poor prognosis. 17 However, there is no relevance in statistics between tumor differentiation and 253LN metastasis in this study. The reason may be that the biology of CRLM is poor generally, and which subgroup is worse could not be distinguished just by the status of 253LN. Furthermore, we failed to find the difference on 253LN positive rate and the influence on RFS among descending colon, sigmoid colon and rectum, which was similar to the results of previous studies.11,15,16 Although the pattern of lymphatic drainage is not the same exactly, 253LN is still a key station, and we believe that D3 resection is equally important for left-sided CRLM.
As a retrospective study, we did not compare the prognosis between 253LN resection group and unresection group, because D3 resection was routinely performed in our institution. Then, we failed to construct a useful model only based on clinicopathological data, to predict 253LN status in patients with left-sided CRLM before surgery. Third, the number of patients enrolled in this study is limited, and more convincing results need to be conformed in a larger clinical research in the future.
Conclusion
The incidence rate of No.253 lymph node metastasis in left-sided CRLM is 20.64% and of skip metastasis is 10.3%. The 253LN status is an independent prognostic risk factor for RFS but not for OS after curative-intent surgery. We recommend to resect 253LN in left-sided CRLM.
Supplemental Material
sj-docx-1-onc-10.1177_11795549221084841 – Supplemental material for No.253 Lymph Nodes Metastasis in Left-Sided Colorectal Cancer Liver Metastasis (CRLM) Patients: Incidence and Prognosis
Supplemental material, sj-docx-1-onc-10.1177_11795549221084841 for No.253 Lymph Nodes Metastasis in Left-Sided Colorectal Cancer Liver Metastasis (CRLM) Patients: Incidence and Prognosis by Jiang Chang, Yihao Mao, Qingyang Feng, Yijiao Chen, Qi Wu, Peng Zheng, Zhiyuan Zhang, Shanchao Yu, Yudong Jiang, Ye Wei, Jianmin Xu and Guodong He in Clinical Medicine Insights: Oncology
Supplemental Material
sj-jpg-2-onc-10.1177_11795549221084841 – Supplemental material for No.253 Lymph Nodes Metastasis in Left-Sided Colorectal Cancer Liver Metastasis (CRLM) Patients: Incidence and Prognosis
Supplemental material, sj-jpg-2-onc-10.1177_11795549221084841 for No.253 Lymph Nodes Metastasis in Left-Sided Colorectal Cancer Liver Metastasis (CRLM) Patients: Incidence and Prognosis by Jiang Chang, Yihao Mao, Qingyang Feng, Yijiao Chen, Qi Wu, Peng Zheng, Zhiyuan Zhang, Shanchao Yu, Yudong Jiang, Ye Wei, Jianmin Xu and Guodong He in Clinical Medicine Insights: Oncology
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was Supported by the National Key R&D Program of China (2017YFC0908200), the National Natural Science Foundation of China (No. 82173164, No. 82002517), and the Shanghai Sailing Program (20YF1407100).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conception and design, manuscript writing, and final approval: All authors. Administrative support and provision of study materials or patients: G.H., J.X., and Y.W. Collection and assembly of data: J.C., Y.M., Q.F., Y.C., and Q.W. Data analysis and interpretation: J.C., Y.M., Q.F., P.Z., Z.Z., S.Y., and Y.J.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.