
Abstract
Objective
To study the benefit of surgery in different types of isolated concha bullosa.
Design
Prospective case series.
Setting
Academic Medical Center.
Patients
Forty seven symptomatic patients complaining of nasal congestion and block, headache and facial pain having concha bullosa without any other sinonasal finding. Their conchae bullosa were classified as lamellar, bulbous and extensive concha bullosa. They were subjected to endoscopic operation.
Main outcome measures
Subjective evaluation of postoperative improvement of sinonasal symptoms and objective pre- and postoperative measurement of total nasal resistance by rhinomanometry.
Results
Two patients (25%) of lamellar type showed complete improvement, 5 patients (62.5%) showed partial improvement and 1 patient (12.5%) showed no improvement. Regarding bulbous type, 16 patients (72.72%) showed complete improvement, 6 patients (27.28%) showed partial improvement and no patient (0%) showed no improvement. Regarding extensive type, 15 (88.24%) patients showed complete improvement, 2 patients (11.76%) showed partial improvement and no patient (0%) showed no improvement. The total nasal resistance was 0.25 Pa/cm3 per second postoperatively compared with 0.37 Pa/cm3 per second preoperatively in patients having lamellar type; 0.28 Pa/cm3 per second postoperatively compared with 0.71 Pa/cm3 per second preoperatively in patients having bulbous type; and 0.27 Pa/cm3 per second postoperatively compared with 0.67 Pa/cm3 per second preoperatively in patients having extensive type.
Conclusions
With proper patient selection, the operative management is of great value in relieving the sinonasal symptoms in patients having isolated Concha bullosa. This will be more obvious in certain types as bulbous and extensive types especially of large sizes.
Introduction
Anatomic variations in paranasal sinus region have been shown to be of clinical importance. 1 Concha bullosa (CB) is a hypertrophy and pneumatization of the nasal turbinate, occurring most often in the middle, and less commonly, in the inferior or superior turbinates. Its association with high incidence of sinus infection is not sure.2,3
CB is one of the most common variations of the sinonasal anatomy. A 14%–53.6% frequency of concha bullosa was reported by various studies. 4 Bolger et al have classified pneumatization of the concha based on the location as lamellar concha bullosa (LCB), bulbous concha bullosa (BCB) and extensive concha bullosa (ECB). 1
The aim of this study is to demonstrate the relation between CB and symptomatology of the nose and the benefits of doing surgery in different types of isolated CB.
Patients and Methods
Prospective study obtained between August 1, 2008 and September 30, 2010 in Saudi German Hospital in Jeddah; Saudi Arabia. A total of 47 patients of different age groups, who were admitted to our clinic complaining of symptoms related to sinonasal region and their paranasal CT studies showed pneumatization of the middle concha, were included in this study.
The most common symptoms encountered in these patients were nasal obstruction, headache and intermittent pain in the periorbital area, between the eyes, or in the cheeks and frontal bone. The occurrence of such pain is accompanied by the congestion and feeling of the pressure deep inside the nasal cavity. Mostly, the pain is unilateral lasting between few hours up to several days. The intensity of pain varies from an individual to the other but it is more of dull, boring character and typically unresponsive to common pain relieving medications. We tried medical treatment for all patients as systemic antibiotics, systemic analgesics, systemic antihistaminics, local corticosteroids and nasal decongestants for 15 days with no or mild improvement.
Any patient who had a sinus problem, sinonasal polyposis or previous sinus surgery was excluded from the study.
All examinations were performed for evaluation of symptoms referable to the sinonasal region. If presenting at the time of headache, a Xylocaine test was done, provided there is no sign of infection. This is done by inserting a cotton wool probe soaked in Xylocaine (2% or 4%), between the CB and the lateral wall and nasal septum where they touch one another, to see if this aborts headache. The pain disappeared within 5 to 10 minutes in 19 out of the 28 patients presenting at the time of headache.
Pneumatization of the middle concha was classified depending on the pneumatization of the lamellar and bullous portions of the middle concha as lamellar and bulbous, respectively. Pneumatization of both the lamellar and bullous portions of the middle concha was classified as the extensive type.
If a CB was present, it was graded in size as small, moderate or large. If bilateral concha were present, sizes were compared and when one was larger, it was identified as dominant.
All patients were subjected to endoscopic partial lateral middle turbinectomy. Nasal tampons were removed 2 days after surgery and followed clinically over next 3 months. Endoscopic examination visits were performed 7, 15, 30, 60 and 90 days after surgical treatment.
Assessment of the effect of surgery was determined by subjective patient questionnaire given to the patients 6 months postoperative. Then the results were graded either complete improvement if there is complete disappearance of the nasal obstruction, headache and facial pain, partial improvement if the patient reported improvement of nasal obstruction and headache without complete cure or no improvement if nasal obstruction, headache and intermittent pain nasal obstruction, headache and facial pain persist.
All patients were subjected to anterior rhinomanometry preoperatively and 6 months postoperatively. The anterior rhinomanometry procedure included the placement of a pressure sensor in one nostril and detected the flow of air in the other nostril. Hence, the resistance of each nasal cavity and total nasal resistance could be calculated separately.
We got approval for doing this work from the Saudi German Hospital ethical committee dated July 1st 2008.
Statistical method
The data were coded and entered using the statistical package SPSS version 12. The data were summarized using descriptive statistics: mean, standard deviation, minimal and maximum values for quantitative variables and number and percentage for qualitative values. Statistical differences between groups were tested using Chi Square test for qualitative variables. The cutoff level for P-value is 0.05. P-values less than, or equal to 0.05 were considered statistically significant.
Results
A total of 47 patients were included in this study. There were 30 females (63.8%) and 17 males (36.2%). The mean + standard deviation of age of the patients included in the study was 30 + 19, ranging from 18 to 57.
Unilateral conchae bullosa were noted in 25 (53.2%) patients (Fig. 1) and bilateral conchae bullosa were noted in 22 (46.8%) patients (Figs. 2–4).

Unilateral bulbous concha bullosa.
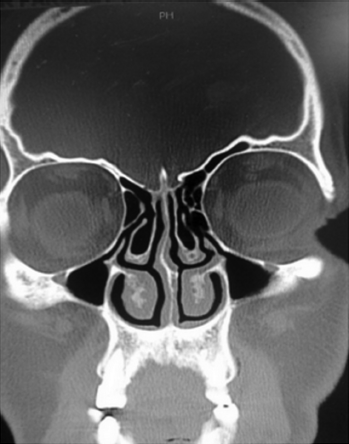
Bilateral concha bullosa (Lt. Lamellar, Rt. Extensive).
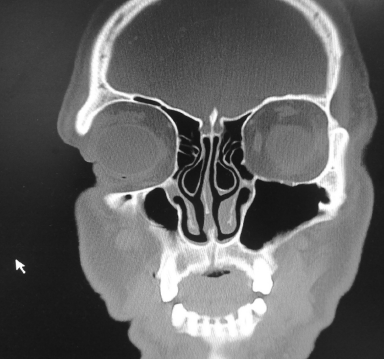
Bilateral bulbous concha bullosa.

Bilateral extensive concha bullosa.
A total of 69 conchae bullosa were detected. Of the conchae bullosa, 37 (53.6%) were at the left and 32 (46.4%) at the right side.
Eight (17%) patients had lamellar type (Fig. 2), 22 (46.8%) had bulbous type (Figs. 1 and 3) and 17 (36.2%) had extensive type (Figs. 2 and 4) (Fig. 5).
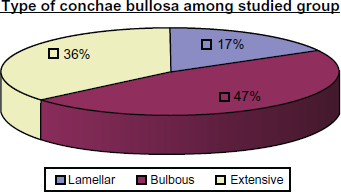
Type of Conchae bullosa among studied group.
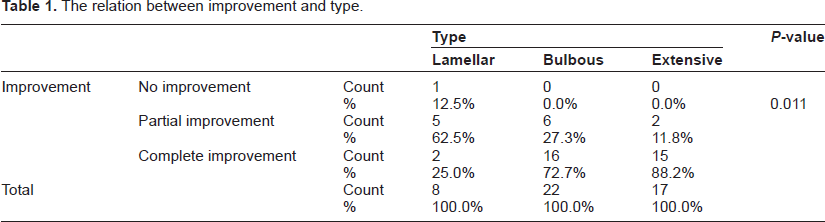
Regarding the patient questionnaire given to the patients 6 months postoperative, with the lamellar type, 2 patients (25%) showed complete improvement, 5 patients (62.5%) showed partial improvement and 1 patient (12.5%) showed no improvement.
Regarding the patients with the bulbous type, 16 patients (72.72%) showed complete improvement, 6 patients (27.28%) showed partial improvement and no patient (0%) showed no improvement.
Regarding the patients with the extensive type, 15 (88.24%) patients showed complete improvement, 2 patients (11.76%) showed partial improvement and no patient (0%) showed no improvement. There were no important complications.
A statistically significant difference was found between different types and improvement among them (Table 1) (Fig. 6).
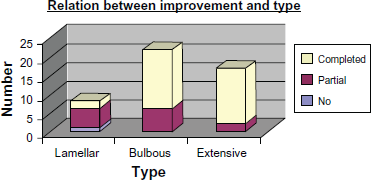
Relation between subjective improvement and type.
The relation between improvement and type.
Regarding the preoperative results of rhinomanometry, the minimum, maximum, and median total nasal resistance calculated at 150 Pa of pressure in patients having lamellar conchae bullosa was 0.17, 1.14, and 0.37 Pa/cm3 per second, respectively, compared with 0.17, 0.46, and 0.25 Pa/cm3 per second 6 months postoperatively.
Regarding the patients with the bulbous type, the minimum, maximum, and median total nasal resistance calculated at 150 Pa of pressure was 0.23, 2.38, and 0.71 Pa/cm3 per second, respectively, compared with 0.16, 0.49, and 0.28 Pa/cm3 per second 6 months postoperatively.
Regarding the patients with the extensive type, the minimum, maximum, and median total nasal resistance calculated at 150 Pa of pressure was 0.28, 1.92, and 0.67 Pa/cm3 per second, respectively, compared with 0.20, 0.51, and 0.27 Pa/cm3 per second 6 months postoperatively (P = 0.018) (Table 2) (Fig. 7).
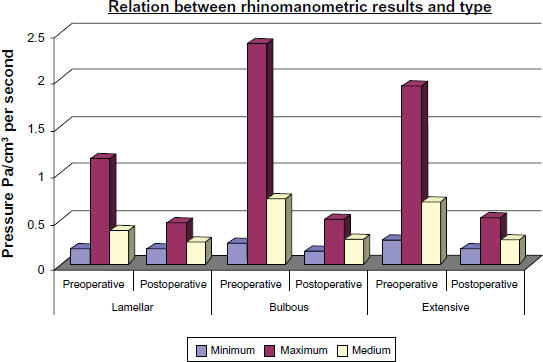
Relation between rhinomanometric results and type.
The relation between the result of rhinomanometry and type of concha bullosa.

P-value demonstrates the difference in improvement between various types with the highest percentage of complete improvement among extensive followed by bulbous types and the least among lamellar type. In this study, P-value is less than 0.05. This means the presence of statistically significant difference between groups.
Discussion
Concha bullosa (CB) is the pneumatization of the concha and is the most frequent variation of the sinonasal anatomy. 4 It is most commonly encountered in the middle concha. It is rarely found in the superior and inferior conchae. This pneumatization results when ethmoid air cells migrate to the middle concha. 5
The CB incidence in the literature ranges from 14%–53.6%. Some authors have not included small-sized or lamellar type conchae bullosa in their studies. 4 Scribano et al have reported incidences up to 67% and Perez-Pinas et al up to 73%.6,7 Presence of bilateral conchae bullosa ranges from 45%–61.5%.4–8 Zinreich et al used coronal CT to evaluate 320 patients for sinus disease, and found that 34% exhibited CB on at least one side. 5 CB was bilateral in 46.88% of the cases in our study.
Bolger et al have divided the pneumatization of the middle concha into three groups: lamellar type is the pneumatization of the vertical lamella of the concha; bulbous type is the pneumatization of the bulbous segment (inferior portion of the turbinate); pneumatization of both the lamellar and bulbous parts is called extensive CB. 1 They studied anatomic variations of the paranasal sinuses in 202 patients based on CT images, and observed lamellar-type CB in 46.2% of the cases, bulbous-type CB in 31.2%, and extensive CB in 15.7%. 1 In this study; eight (17%) of the conchae bullosa were lamellar type, 22 (46.8%) were bulbous type and 17 (36.2%) were extensive type.
There is no consensus on the frequency of CB or frequency of types of CB. The variances may be due to differences between the study groups, differences in pneumatization parameters and the analytical methods used. There are studies pointing out that the size of CB is important for the presence of symptoms.5,9
ENT specialists believe that especially bulbous type CB with large dimensions may have a role in nasal complaints. 10 The degree of pneumatization determines the severity of symptoms. The lamellar type usually does not cause severe symptoms, whereas the bulbous and extensive forms typically are symptomatic. 8 The most common symptoms are nasal obstruction and facial pain. Swelling of the nasal turbinates particularly in the middle part of the nasal cavity may result in contact with the nasal septum or lateral nasal wall in especially sensitive area creating a “trigger” for development of headache. This type of headache is called: Middle turbinate headache syndrome and is characterized by intermittent pain located in the periorbital area, between the eyes, or in the cheeks and frontal bone. The occurrence of such pain is accompanied by the congestion and feeling of the pressure deep inside the nasal cavity. Mostly the pain is unilateral lasting between few hours up to several days. The intensity of pain varies from an individual to the other but it is more of dull, boring character and typically unresponsive to common pain relieving medications.
We studied the importance of surgical intervention to different types of CB (lamellar, bulbous and extensive) in relation to nasal symptoms relief and change in the total nasal resistance as measured by rhinomanometry. Total nasal resistance is less variable than unilateral nasal resistance because it incorporates both nasal airways and, thus, is not affected by the nasal cycle. Consequently, it is a better predictor of the presence of nasal obstruction. The patients included in our study were symptomatic cases suspected of having sinonasal disease. Therefore the statistical interpretations of the conclusions of our study are valid only for the symptomatic population. The results should not be generalized to the whole population.
Postoperative follow-up of our patients for 6 months revealed complete improvement of the patient symptoms in 25% of the lamellar type, compared with 72.72% of the bulbous type and 88.24% of the extensive type. Also, there is partial improvement in 62.5% of the lamellar type compared with 27.28% of the bulbous type and 11.76% of the extensive type. In the whole study group, only one patient showed no improvement. His CB was of the lamellar type. In general, the patients showed marked improvement in symptoms. There were no important complications.
Our rhinomanometric results revealed that the median total nasal resistance was 0.25 Pa/cm3 per second postoperatively compared with 0.37 Pa/cm3 per second preoperatively in patients having lamellar conchae bullosa. Also, it was 0.28 Pa/cm3 per second postoperatively compared with 0.71 Pa/cm3 per second preoperatively in patients having bulbous type. Lastly, it was 0.27 Pa/cm3 per second postoperatively compared with 0.67 Pa/cm3 per second preoperatively in patients having the extensive type. The rhinomanometric change corresponded with the patients' subjective improvement in the relief of nasal obstruction.
P-value in this study is less than 0.05 that denotes the presence of statistically significant difference in improvement between different groups with the highest percentage of complete improvement among extensive followed by bulbous types and the least among lamellar type.
These results suggest that there is intimate relation between CB and sinonasal symptoms. Also, there is variation in sinonasal symptoms regarding the size and type of CB. The symptoms are more severe and prominent in certain types of CB as bulbous and extensive types especially in large size conchae. So, those patients having bulbous and extensive types especially of large sizes usually express marked improvement in response to the operative management.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers of this paper report no conflicts of interest. The author confirms that they have permission to reproduce any copyrighted material.